


Abstract
Transformed small cell carcinoma of the prostate represents a tumor biology distinct from its adenocarcinoma counterpart, and penile metastasis from prostate cancer is a rare phenomenon. Biologic heterogeneity among metastatic lesions in a patient with prostatic adenocarcinoma with SCPCa transformation is presented here. The case report shows the significance of using dual-tracer PET/CT with 68Ga-prostate-specific membrane antigen and 18F-FDG in diagnosing small cell carcinoma of prostate transformation in certain lesions, thereby guiding therapeutic strategies. Furthermore, the value of sequential dual-tracer PET/CT in assessing overall disease status, theranostics, and response to multimodality therapy is illustrated.
- oncology
- 177Lu-PSMA therapy
- 18F-FDG PET/CT
- 68Ga-PSMA PET/CT
- penile metastases
- small cell carcinoma of prostate
Small cell carcinoma of the prostate (SCPCa) is relatively uncommon, with an estimated incidence of less than 1% of all prostate cancer. Pure SCPCa at initial presentation is observed in 50% of cases, whereas 25%–50% are mixed with adenocarcinoma or with adenocarcinoma transformed into SCPCa during hormonal therapy. The salient features of SCPCa transformation include a worse prognosis, a preponderance of visceral metastasis, and hypermetabolism on 18F-FDG PET/CT. The serum prostate-specific antigen (PSA) level is low or undetectable in SCPCa relative to tumor burden and not predictive of disease severity or useful for surveillance. The present case illustrates the features and utility of dual-tracer 68Ga-prostate-specific membrane antigen (PSMA) and 18F-FDG PET/CT in assessing transformed SCPCa and guiding treatment strategies.
CASE REPORT
A 70-y-old man diagnosed with prostatic adenocarcinoma (Gleason score, 4 + 3 = 7) and serum PSA of 60 ng/mL had undergone bilateral orchidectomy and, on bicalutamide, demonstrated an increasing level of serum PSA (2014: 1.31 ng/mL; 2015: 1.73 ng/mL; 2016: 4.7 ng/mL). 68Ga-PSMA PET/CT (Fig. 1A) showed 68Ga-PSMA–avid prostatic primary dorsal (D9) vertebral lesions and faint uptake in a pelvic mass with central necrosis. CT-guided biopsy from the pelvic mass showed features of SCPCa transformation from prostate cancer. The patient received chemotherapy and external-beam radiation therapy (30 Gy) to the pelvic mass in September 2016. 68Ga-PSMA PET/CT in December 2016 (Fig. 1B) showed reduction of the pelvic mass, decreased uptake in the prostate lesion, and decreasing serial serum PSA levels until January 2017. Subsequently, the patient presented with complaints of lower abdominal pain, backache, and dysuria and had an increasing level of serum PSA (3.7 ng/mL in January 2017 and 8.0 ng/mL in June 2017). 68Ga-PSMA PET/CT (Fig. 2A) showed intensely tracer-avid foci in multiple dorsal and lumbar vertebrae, bilaterally in the ribs, and in the pelvic bone, with nonavid lesions in the left pelvic soft tissue and penile shaft (without skin ulceration and break), and 18F-FDG PET/CT (Figs. 2B and 2C) showed avid skeletal lesions similar to those on 68Ga-PSMA PET/CT, intensely avid left pelvic soft-tissue (SUVmax, 45) and penile shaft lesions (SUVmax, 44), commensurate with transformed SCPCa. Considered for radioligand therapy targeting 68Ga-PSMA–avid skeletal lesions, the patient received 4,440 MBq of 177Lu-PSMA. Follow-up 68Ga-PSMA PET/CT (Fig. 2A) showed an appreciable reduction in uptake in the skeletal lesions and a reduced serum PSA level (down to 3 ng/mL from 8 ng/mL);18F-FDG PET/CT (Figs. 2B and 2D) showed reduced uptake in the skeletal lesions but an increase in the size and avidity of the left pelvic soft-tissue lesion (SUVmax, 60; 4.8 × 4.9 cm), resulting in left hydronephrosis with hydroureter, and in the penile shaft lesion (SUVmax, 58; 5.0 × 3.6 cm). He received a second cycle of 177Lu-PSMA (4,810 MBq) and intensity-modulated radiation therapy/image-guided radiation therapy of 30 Gy to the non–PSMA-avid left pelvic soft tissue. Follow-up 68Ga-PSMA PET/CT in December 2017 (Fig. 2A) showed a substantial decrease in uptake in most skeletal lesions and a reduction in the serum PSA level (1 ng/mL), and 18F-FDG PET/CT (Figs. 2B and 2E) showed a decrease in size and uptake in the left pelvic soft tissue lesion (SUVmax, 6; 1.5 × 1.7 cm) related to intensity-modulated radiation therapy, with the penile shaft lesion showing persistence of 18F-FDG uptake.
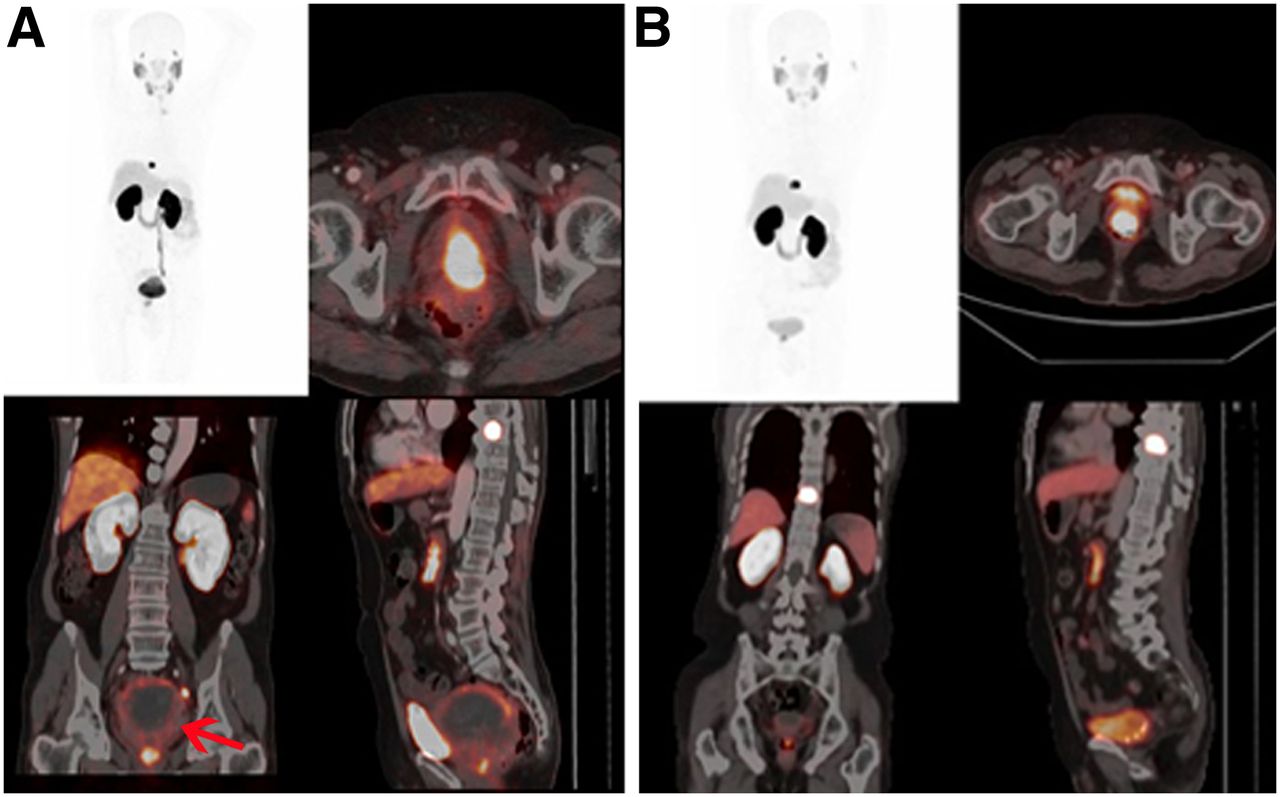
(A) 68Ga-PSMA PET/CT (March 2016) showing intensely avid prostatic and D9 vertebral lesions, faint uptake in large pelvic mass, and central necrosis infiltrating prostate and rectum (arrow). (B) 68Ga-PSMA PET/CT (December 2016) showing significant reduction of pelvic mass and decreased uptake in prostatic lesion.

(A) 68Ga-PSMA PET/CT demonstrating intense avidity in multiple dorsal and lumbar vertebrae (pink arrows), bilaterally in ribs, and in pelvic bone, with nonavid left pelvic soft-tissue (red arrows) and penile shaft lesions. 18F-FDG PET/CT (B and C) showed intense skeletal lesions similar to 68Ga-PSMA, intensely avid left pelvic soft-tissue lesion (SUVmax, 45; 3.0 × 2.2 cm; red arrow) and 18F-FDG–avid penile shaft lesion (SUVmax, 44; 2.5 × 2.0 cm; green arrow). Follow-up 68Ga-PSMA-PET/CT (A) showed decrease in uptake in skeletal lesions; 18F-FDG PET/CT (B, D, and E) showed decrease in size and uptake in left pelvic soft-tissue lesion (red arrow; SUVmax, 6; 1.5 × 1.7 cm), indicating response to intensity-modulated radiation therapy, and untreated penile shaft lesion demonstrated persistence of 18F-FDG uptake (green arrow).
DISCUSSION
18F-FDG PET/CT is not routinely recommended in prostate adenocarcinoma for both biologic and technical reasons: low 18F-FDG uptake as compared with other malignancies (low glycolytic activity in prostatic cancer cells) and urinary excretion of 18F-FDG masking pathologic uptake in the adjacent areas. Prostate cancer metastatic to the penis is rare and may present with asymptomatic nodules in the penile shaft or with symptoms of pain at erection and dysuria (1).
In this case report, biologic heterogeneity among metastatic lesions is presented in a patient with prostatic adenocarcinoma with SCPCa transformation, harboring 68Ga-PSMA–avid skeletal lesions demonstrating a favorable response to 177Lu-PSMA therapy, whereas metastatic SCPCa transformed pelvic and penile lesions were nonavid with 68Ga-PSMA but avid with 18F-FDG. The pelvic mass demonstrated disease progression after the first cycle of 177Lu-PSMA therapy but regression after intensity-modulated radiation therapy. After a multimodal therapeutic approach (177Lu-PSMA and radiotherapy), serial serum PSA examination showed a trend toward a decrease in PSA level.
CONCLUSION
The present case illustrates the significance of dual-tracer PET/CT and theranostics in metastatic prostate adenocarcinoma with evidence of SCPCa transformation. Such an approach helped in guiding treatment decision making and in monitoring the response to multimodality therapy.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Aug. 23, 2018.
- Received for publication June 2, 2018.
- Accepted for publication August 6, 2018.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.