


Abstract
A 48-y-old man with a history of colon cancer presented with recurrent hepatic metastasis along a prior microwave ablation bed. Split-bolus, intraprocedural 18F-FDG PET was performed to guide repeat microwave ablation and immediately confirm complete treatment. PET-guided ablation is highly accurate for targeting and treating malignant hepatic lesions and feasible for nonspecialized tertiary care hospitals without an onsite cyclotron.
For detection of local cancer recurrence or progression after therapy, 18F-FDG PET/CT is a powerful imaging tool (1). In particular, it can detect progression after thermal ablation of liver metastases with sensitivity of 92%–95% and specificity of 100% (2). Ryan et al. (3) showed that PET/CT can be used as an intraprocedural technique for targeting of anatomically occult lesions, with immediate confirmation of treatment success.
CASE REPORT
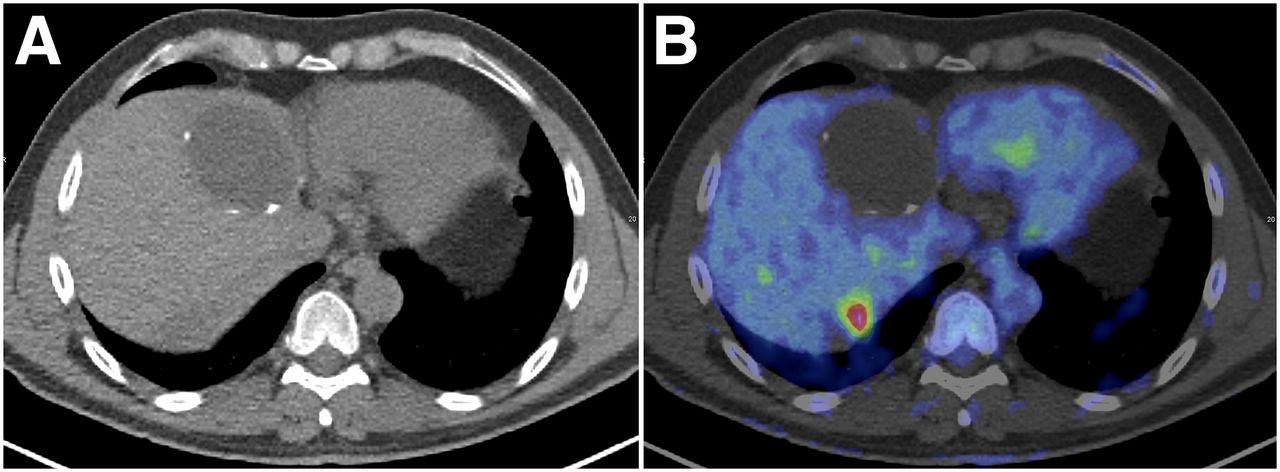
A 48-y-old man with a history of colon cancer underwent combined CT- and ultrasound-guided microwave ablation of an unresectable liver metastasis. Five months later, his carcinoembryonic antigen level was elevated and trended upward despite a lack of correlation on serial CT. Because of prior treatment effects, the lesion could not be identified by follow-up ultrasound and CT (Fig. 1A), precluding repeat ablation using standard guidance. Seven months after ablation, PET/CT identified an 18F-FDG–avid recurrence along the ablation bed (Fig. 1B). Based on a novel technique from Memorial Sloan Kettering Cancer Center (3), split-dose 18F-FDG PET/CT was selected for lesion targeting and immediate assessment of treatment.
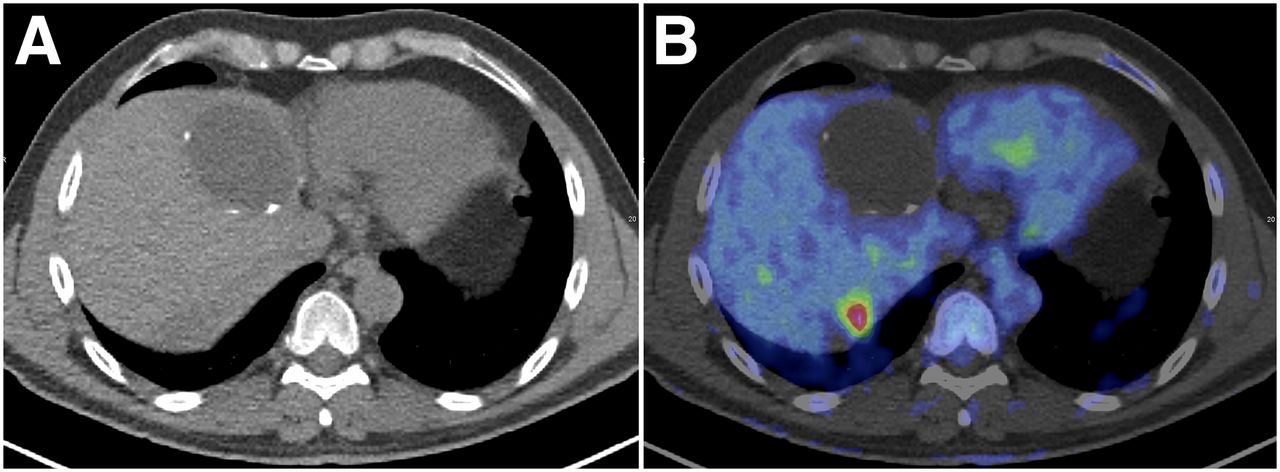
CT (A) and PET/CT (B) show ill-defined, hypodense region of hepatic segment 7, representing anatomically stable ablation bed of previously treated lesion. Fused image reveals metabolically active tumor along ablation bed. Anterior hypodense, metabolically quiescent lesion represents chronic asymptomatic biloma.
Doses of 18F-FDG were obtained from a local radiopharmaceutical supplier. The first (targeting dose) was calibrated for 148 MBq (4 mCi), and the second (treatment efficacy dose) was calibrated for 296 MBq (8 mCi) 3 h later. This interval was based on a 45-min uptake time for the targeting dose and an estimated 195 min for the ablation. Using a similar timeline and 30-min uptake period for the second dose, Memorial Sloan Kettering Cancer Center showed that approximately 90% of the postprocedural PET image is derived from the postablation dose, thereby reflecting the tumor’s posttreatment metabolic state (3).
The initial targeting PET/CT was obtained using a limited field of view, low-dose CT, and a 1-min PET scanning time per bed position (Fig. 2A). Using 3 serial CT scans fused with the initial targeting PET scan, the microwave ablation antenna was advanced into the 18F-FDG–avid lesion (Fig. 2B). The procedure was completed in 127 min, versus the planned 195 min; therefore, the treatment efficacy dose was reduced to 296 MBq (8 mCi) by removing the excess activity. Repeat limited PET/CT showed a complete lack of 18F-FDG avidity (Fig. 2C), confirming therapeutic success.
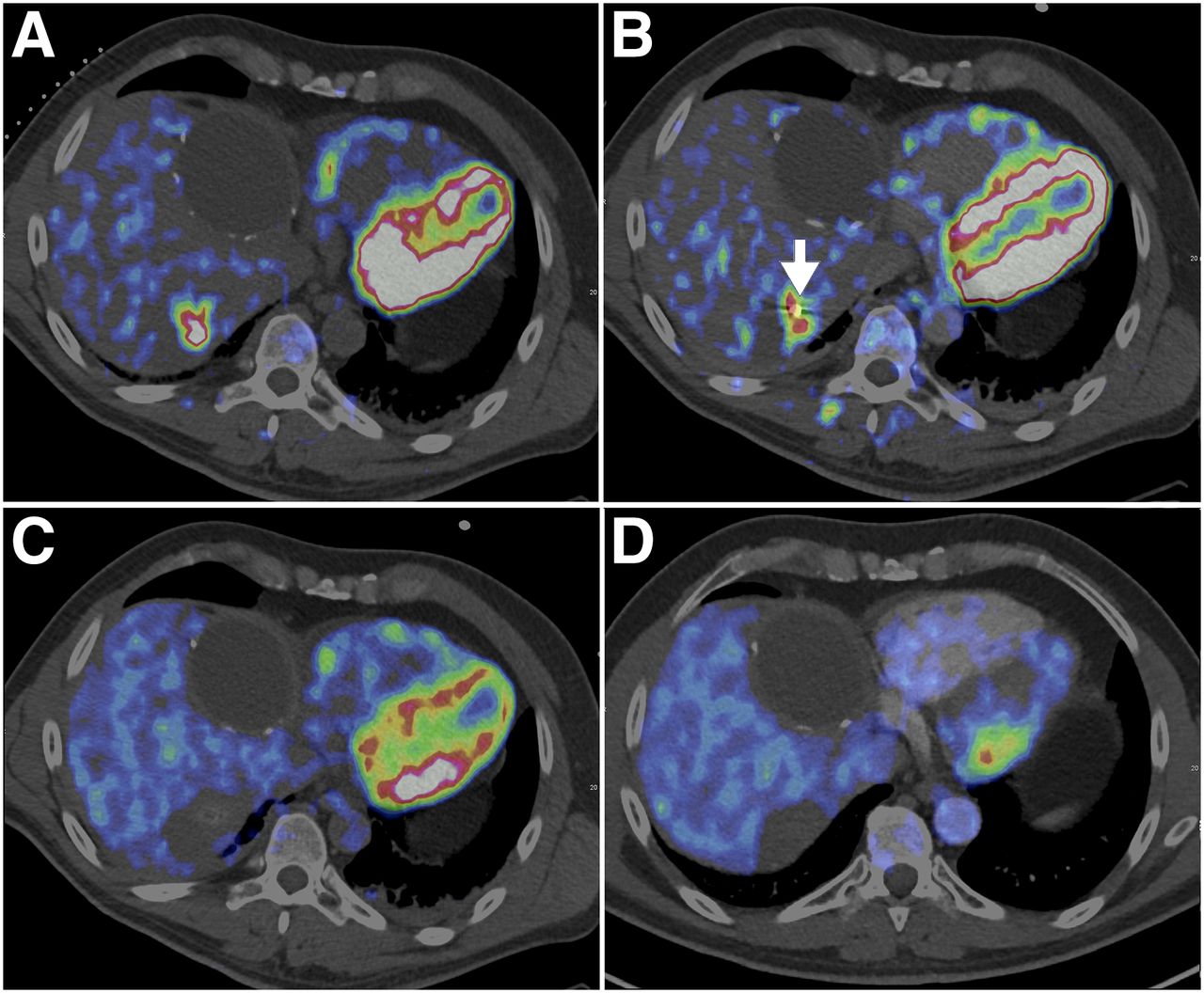
(A and B) Images before (A) and during (B) PET/CT-guided microwave ablation of metastasis using split-bolus approach. Arrow in intraprocedural image denotes microwave antenna. (C) Image immediately after ablation shows resolution of 18F-FDG avidity, confirming treatment efficacy. (D) PET/CT 1 mo after ablation demonstrates no focal PET avidity.
DISCUSSION
Ablative therapy is commonly used for oligometastatic hepatic lesions. However, small lesions or recurrence near previous treatment beds may be difficult to target by CT or ultrasound. PET can delineate the metabolically active focus for ablation, thereby minimizing the likelihood of undertreatment. Furthermore, our experience shows that split-dose, PET-guided microwave ablation is feasible in a nonspecialized tertiary care hospital using commercially procured 18F-FDG.
CONCLUSION
Intraprocedural PET can guide and confirm ablation of hepatic lesions that are otherwise occult on CT and ultrasound.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Dr. Stephen Solomon of Memorial Sloan-Kettering Cancer Center for helpful input.
Footnotes
Published online Jan. 25, 2019.
- Received for publication July 9, 2018.
- Accepted for publication September 7, 2018.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.