


Abstract
We describe the role of 18F-sodium fluoride (18F-NaF) PET/CT bone scanning in the staging of breast and prostate cancer. 18F-NaF PET was initially utilized as a bone scanning agent in the 1960s and early 1970s, however, its use was restricted by the then-available γ-cameras. The advent of hybrid PET/CT cameras in the late 1990s has shown a resurgence of interest in its use and role. After a brief introduction, this paper describes the radiopharmaceutical properties, dosimetry, pharmacokinetics, and mechanism of uptake of 18F-NaF. The performance of 18F-NaF PET/CT is then compared with that of conventional bone scintigraphy using current evidence from the literature. Strengths and weaknesses of 18F-NaF PET/CT imaging are highlighted. Clinical examples of improved accuracy of diagnosis and impact on patient management are illustrated. Limitations of 18F-NaF PET/CT imaging are outlined.
Many people with cancer will develop bone metastases during the course of their disease. The American Cancer Society estimated that of the 569,490 people who died of cancer in 2010, approximately 350,000 had bone metastases (1).
There are 2 main types of bone metastasis: osteoblastic and osteolytic. Osteoblastic disease occurs when the cancer cells cause an increase in bone formation, resulting in denser or sclerotic features. This is often associated with prostate cancer tumor types. Osteolytic disease occurs when the cancer cells cause increased bone mineral turnover or resorption, resulting in a decrease in bone density. This can cause weakening of the bone structures, which can result in bone fractures upon minimal trauma. Osteolytic disease is more commonly associated with lung or renal cancer tumor types. Some bone metastases, including those originating from breast cancer, will include a mixture of both osteoblastic and osteolytic types because a bone metastasis of solely one type is rare in breast cancer.
Primary cancers in the body can metastasize to bone, especially in patients with late-stage or recurrent disease, but also earlier in the course of the disease. This is especially true in patients with breast and prostate cancer, but bone metastases can also be seen in lung, thyroid, and renal malignancies as well as in many other cancers.
The staging of a primary malignancy is essential to categorize the malignancy as either locally based or with further spread to either local or distant lymph nodes or to distant organs or tissues such as the lungs, liver, brain, adrenal glands, bony skeleton, or peritoneum.
Several classifications have been created to stage different types of cancers, the most commonly used being the TNM classification (2), which describes the main tumor size and extent (T), the degree of involvement of lymph nodes (N), and the presence or absence of distant metastatic spread (M). If a cancer is found to be only locally based after having been treated for spread to the liver, for example, then the cancer is said to be downstaged. If spread to lymph nodes or distant organs is confirmed in a cancer that initially was based locally in the primary organ, then the cancer is said to be upstaged.
Accurate delineation of bone metastases is important because the cancer is either upstaged or downstaged according to whether bone metastases are present or absent, and upstaging and downstaging have a clear impact on patient management in that they help to determine whether curative surgery or palliative care is to be used.
Accurately determining the location of bone metastases also allows monitoring of their response to therapy and occasionally acts as a guide to an appropriate bone biopsy site, should definitive histologic confirmation be required, such as in solitary bony lesions.
Although the incidence of bone metastases at initial diagnosis is 1%–2%, this increases significantly to approximately one third in patients diagnosed at an advanced stage or who have disease recurrence (3).
Imaging of bone metastases has for several decades been undertaken via planar isotope bone scintigraphy using 99mTc labeled with diphosphonate (e.g., methylene diphosphonate [99mTc-MDP]). A more bone-specific PET tracer, sodium fluoride labeled with 18F (18F-NaF), was first proposed as a bone scanning agent back in 1962 by Blau et al. using animal models (4) and was approved by the U.S. Food and Drug Administration in 1972. Its properties included rapid and high uptake in the bony skeleton, yet clinical use was restricted by the γ-camera technology available at that time. Conventional γ-cameras can optimally image the 140-keV photons from 99mTc-MDP but are insensitive in detecting the high-energy 511-keV photons emitted by 18F-NaF, resulting in the dominance of 99mTc-MDP imaging from the mid to late 1970s.
An example of an early 18F-NaF image obtained on a rectilinear bone scanner is demonstrated in Figure 1. Figure 2 shows an example of a rectilinear bone scanner.

Early 18F-NaF image of breast cancer patient with bone metastases (arrows). Examination was undertaken on rectilinear scanner at Guy’s Hospital, London, 1973. (Reproduced by permission of Taylor & Francis Books UK from (20).)

Photograph of rectilinear bone scanner.
There has been a resurgence of interest in using 18F-NaF for bone metastasis imaging since the first clinical hybrid PET/CT scanner was introduced in 1998 at the University of Pittsburgh Medical Center. The high-energy 511-keV photons produced by 18F-NaF can be detected accurately by the hybrid PET/CT scanner. PET/CT allows high-resolution functional imaging of bone metastases with significantly greater sensitivity, specificity, and accuracy than conventional planar bone scintigraphy (5,6). The low-dose CT component also provides a unique platform with which to differentiate between benign and malignant bone lesions, both of which can take up the PET tracer. The low-dose CT component also allows for more accurate anatomic localization within the bony skeleton. However, low-dose CT does not provide a gold standard diagnosis.
In the United Kingdom, a recent publication (7) from the Royal College of Physicians, Royal College of Radiologists, and British Nuclear Medicine Society stated that 18F-NaF is recommended for the assessment of benign and malignant diseases of the bone in selected patients and produces high-quality images.
The European Association of Nuclear Medicine also produced procedure guidelines specifically for the use of 18F-NaF PET/CT, outlining minimum standards for the performance and interpretation of 18F-NaF PET/CT scans (8). Both the U.K. and the European publications refer to guidance from the Society of Nuclear Medicine and Molecular Imaging published back in 2009 (9).
It is therefore apparent that there is an international recognition of the need to replace conventional bone scintigraphy with 18F-NaF PET/CT to detect bone metastases. This process is currently restricted by a lack of funding and availability of PET/CT scanners. No national form of funding (e.g., United Kingdom) or reimbursement (e.g., United States, Canada, and Australia) is set up for these scans, as can be seen in the case of oncologic PET/CT scans with 18F-FDG.
This article explores the resurging role of 18F-NaF PET/CT in the detection of bone metastases, with an emphasis on production; pharmacokinetics; mechanism of uptake; comparisons with conventional imaging such as planar bone scintigraphy, CT, SPECT, and SPECT/CT; clinical protocol; radiation dosimetry; clinical performance of 18F-NaF PET/CT, compared with conventional bone scintigraphy; and strengths and weaknesses.
PRODUCTION AND PHARMACOKINETICS
18F-NaF is produced within a cyclotron by particle acceleration from water-enriched 18O. 18F ions are trapped in an aqueous solution in a cation exchange column. The eluent from the cation exchange cartridge is passed through an anion exchange (HCO3− form) cartridge to trap the 18F-NaF.
The anion exchange cartridge is then flushed with 10 mL of sterile water, and the 18F-NaF is eluted with 10 mL of sterile normal saline and passed through a sterile filter into a sterile multidose vial (10).
18F decays by positron emission. After colliding with an electron, two 511-keV annihilation photons are produced 180° apart: these are detected by a circular array of PET detectors.
The half-life of 18F-NaF is 110 min, and hence it is widely available from the same facilities that produce 18F-FDG for oncologic diagnosis, with no further additional special facilities required.
MECHANISM OF UPTAKE
Once injected intravenously, most of the 18F-Na F is deposited within the bony skeleton after only a single pass of blood; the first-pass uptake is considerably higher than that of 99mTc-phosphates (11).
Uptake of 18F-NaF in the bones is twice that of 99mTc-MDP because 18F-NaF has only minimal binding with serum proteins, allowing for a rapid single-pass extraction and fast clearance from the soft tissues. Conversely, 30% of 99mTc-MDP is protein-bound after injection, and hence this protein-bound 99mTc-MDP is cleared slowly (11). 18F-NaF equilibrates with plasma and is then rapidly cleared after bone deposition and excreted by the kidneys.
Patients can therefore be imaged at only 1 h after injection of 18F-NaF (compared with 3–4 h with 99mTc-MDP). The higher bone uptake leads to a higher bone-to-background ratio and therefore better-resolved images (Fig. 3).
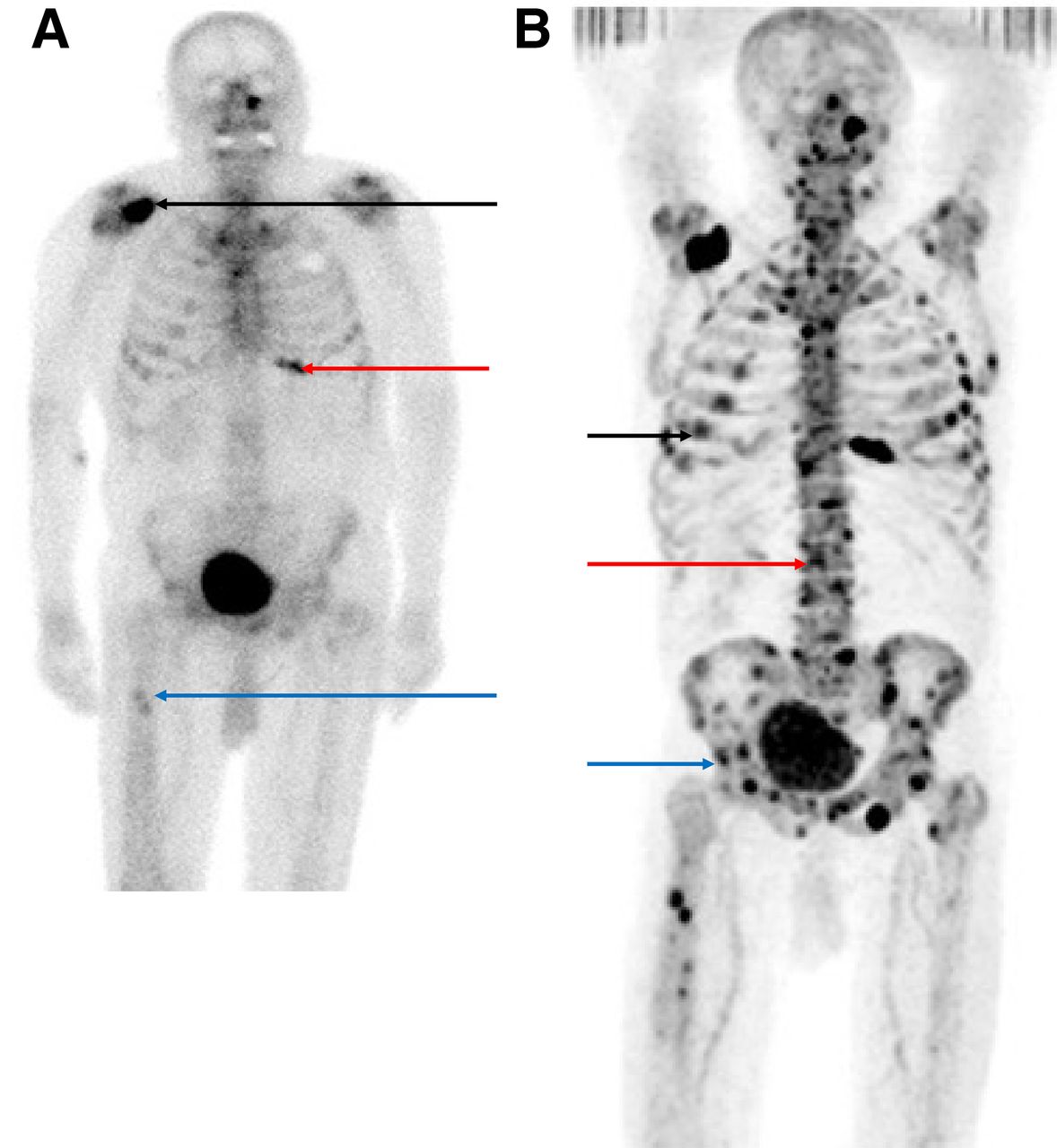
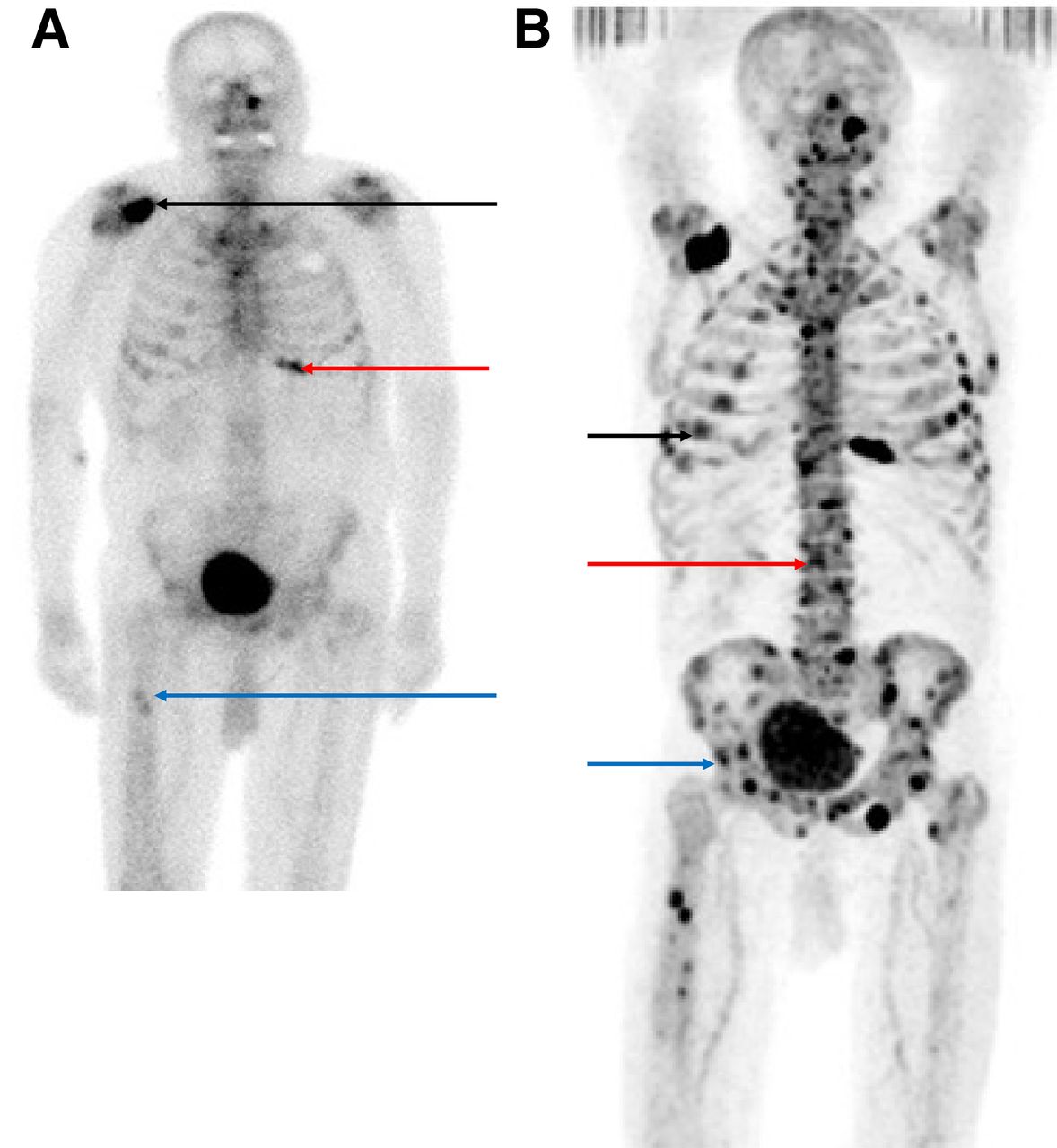
(A) Conventional 99mTc-MDP planar scintigraphy shows several bone metastases in right scapula (black arrow), left lower anterior ribcage (red arrow), and right proximal femoral shaft (blue arrow) in patient with prostate cancer metastases. (B) 18F-NaF PET/CT bone scan obtained shortly afterward clearly shows greater burden of bone metastases than was seen on the 99mTc-MDP scan, especially in ribcage (black arrow), spine (red arrow), and pelvis (blue arrow). (Adapted from (12).)
The mechanism of uptake of 18F-NaF specifically within bone is similar to that of 99mTc-MDP. 18F ions exchange with hydroxyl ions (OH−) on the surface of hydroxyapatite of bone to form fluoroapatite. Uptake of 18F-NaF reflects bone remodeling. Increased uptake occurs through processes that increase bone exposure by increasing the number of binding sites (i.e., osteoblastic or lytic processes) or the blood flow. The rate-limiting step is blood flow (11).
COMPARISON WITH 99MTC-MDP, 99MTC-MDP SPECT, AND 18F-NAF PET/CT
Conventional bone scintigraphy using 99mTc-MDP has reasonable sensitivity but suffers from reduced specificity. The addition of SPECT significantly increases the accuracy of metastatic bone detection, and accuracy is further increased with the use of 18F-NaF PET/CT, as Table 1 illustrates (12).
Comparison of 99mTc-MDP, 99mTc-MDP SPECT, and 18F-NaF PET (44 High-Risk Prostate Cancer Patients (12))
In addition, the reduced specificity of 18F-NaF PET (62%) compared with 99mTc-MDP SPECT is because of the increased sensitivity of PET in detecting bone lesions. Although these are more likely to be benign, their detection can lead to false-positive results and reduced specificity, without the benefit of conventional CT.
Several other studies (13–16) showed improved accuracy in bone lesion detection, as well as a high negative predictive value, for 18F-NaF PET/CT compared with 99mTc-MDP SPECT (13) or planar 99mTc-MDP (15,16). Some of these studies are summarized in Table 2.
Other Studies Showing Improved Accuracy of Bone Lesion Detection Using 18F-NaF PET/CT Over Planar Bone Scintigraphy
The high negative predictive value of 18F-NaF PET/CT thus rules out metastatic spread to the bony skeleton with a high degree of confidence. This is important in such cases as high-risk prostate cancer patients with rising prostate-specific antigen and adverse clinical features.
Determination that there is no skeletal spread renders radiotherapy or radical prostatectomy with a curative approach feasible in these patients, who might otherwise have been managed with a more conservative or palliative approach.
PROCEDURE AND PATIENT PREPARATION
As described by Segall et al. (9) and the 2015 Guidelines of the European Association of Nuclear Medicine (8), patients are first to be provided with an information leaflet before the test, and then a member of the PET/CT team is to explain the procedure to them on their arrival in the department. 18F-NaF radiotracer (370 MBq) is injected into the patient intravenously, and there is usually a 1-h wait before the scan, although this can be shortened to 30–45 min if necessary. Any metal objects on the patient are removed to prevent attenuation artifacts. There is no requirement for fasting or avoidance of medications beforehand, and the patient can talk before the procedure.
The patient should be well hydrated to enhance 18F-NaF renal excretion (17), which also reduces radiation exposure and helps to optimize the target-to-background ratio. Patients void their bladders immediately before the PET/CT scan.
Pregnant patients should not undergo this examination unless the potential benefit outweighs the risk from radiation exposure to the mother and fetus.
Arm position during scanning depends on the indications for the study. The arms may be by the sides when the whole body is imaged or elevated when only the axial skeleton is imaged.
A low-dose CT scan is obtained first from the skull vertex to the mid thighs (<30 s) for attenuation correction and for anatomic localization. The usual CT settings sufficient for attenuation correction and localization are a tube current of 30 mA, voltage of 120 kVp, rotation of 0.5 s, and pitch of 1 (8).
PET imaging is then performed from the vertex of the skull to the mid thighs (∼20-min duration). PET images may be acquired in 2- or 3-dimensional mode. Three-dimensional mode is usually recommended for whole-body acquisition because the higher counting rates compensate for the shorter acquisition times required for imaging a larger area. Acquisition time per bed position can vary but is usually 1–2 min in 3-dimensional mode.
Images can be acquired on either a 128 × 128 matrix or a 256 × 256 matrix and are reconstructed with a 3-dimensional ordered-subset expectation maximization time-of-flight algorithm, ideally with iterative reconstruction.
Coregistered fused PET/CT images are then sent to the workstation for further interpretation. Maximum-intensity projections should also be generated to help facilitate lesion detection.
DOSIMETRY
After an injection of 370 MBq of 18F-NaF, the total effective dose of 18F-NaF PET is 8.9 mSv (18) compared with a total effective dose of 4.2 mSv for 99mTc-MDP SPECT. These values vary according to the injected dose. The radiation exposure associated with the CT component of the PET/CT and SPECT/CT studies is highly variable and ranges from less than 1 mSv for CT attenuation correction up to 8 mSv for a diagnostic CT scan. A typical value is 3.2 mSv (16), and consequently the total effective dose of a 18F-NaF PET/CT study is 12.1 mSv (8.9 + 3.2 mSv) compared with 7.4 mSv (4.2 + 3.2 mSv) for a 99mTc-MDP bone SPECT/CT study.
The total effective dose administered needs to be considered when scanning is repeated to monitor progress, especially because cancer patients in general may be undergoing multiple CT, fluoroscopy, and plain radiography scans, potentially further increasing the radiation dose that the patient receives.
ADVANTAGES OF 18F-NAF PET/CT OVER 99MTC-MDP BONE SCINTIGRAPHY
18F-NaF PET/CT has many advantages over 99mTc-MDP planar bone scintigraphy and 99mTc-MDP SPECT/CT (11,19).
18F-NaF PET tracer emits higher-energy photons; hence, there is better penetration of tissues after administration to the patient, with less scatter and more γ-rays able to reach the scanner detector. Attenuation correction corrects for photons having to travel through dense objects to reach the scanner, and this is provided in all PET/CT scans by means of the CT component. Full-body CT greatly increases spatial resolution and sensitivity and consequently also image quality.
The injection-to-scan time is greatly reduced from 3–4 h to 30–60 min, significantly reducing the overall examination time for patients and increasing throughput, or the number of patients who can be scanned in one session (e.g., scanning 6–7 patients with 18F-NaF PET/CT during the morning session, compared with 3–4 patients with 99mTc-MDP).
In view of the faster uptake and clearance of 18F-NaF, there is twice as much uptake in the bony skeleton, which also leads to better-quality imaging than with 99mTc-MDP.
The low-dose CT scan reduces the need for plain radiographs or diagnostic CT or MRI scans to exclude metastatic disease in equivocal cases. By not requiring patients to wait for extra scans, this reduces their anxiety. A reduced need for additional scans also helps radiologists make swifter and more definitive management decisions in multidisciplinary cancer meetings, which could significantly affect patient management.
A weakness of 18F-NaF PET/CT is that there are more false-positive results because there is more of a tendency to pick up benign pathology (e.g., degenerative joints) instead of just malignant. There are occasional false-negative scans, seen particularly if there is a solitary small lytic metastasis in the bone marrow with little associated osteoblastic activity. There is an increased total effective radiation dose to the patients, and interpretation of the scans requires more time because their greater sensitivity picks up more findings and the CT portion must be viewed in detail.
CLINICAL EXAMPLES
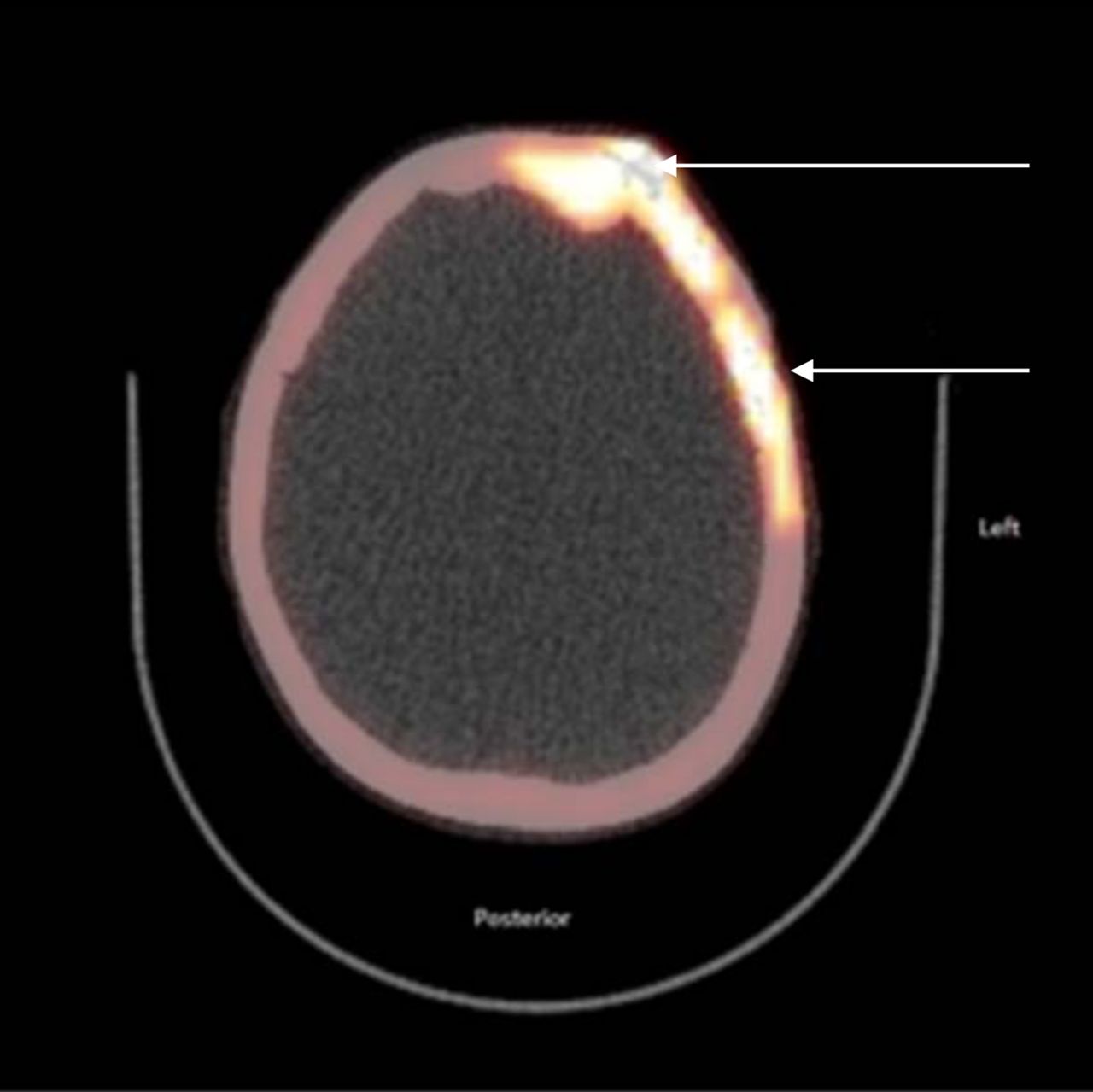
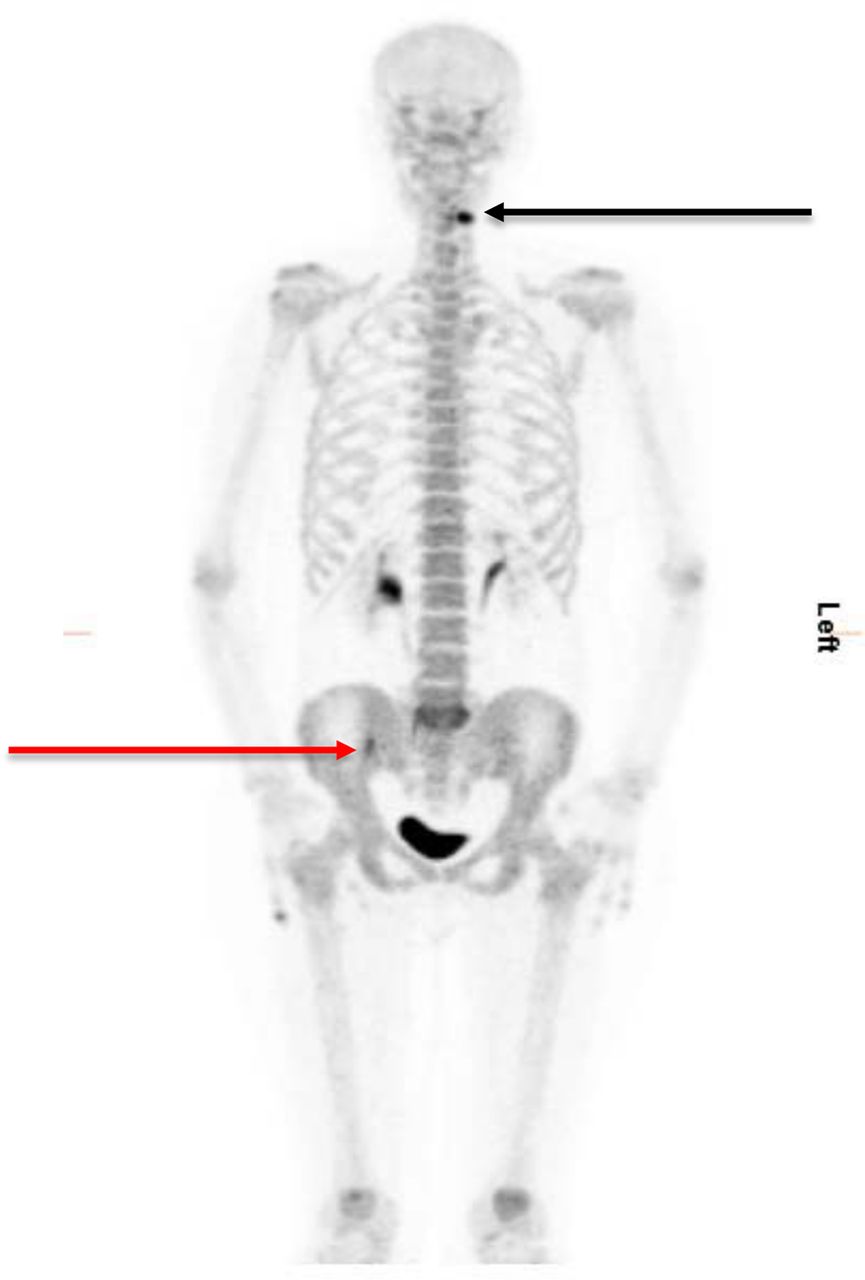
An example of a true-positive 18F-NaF PET/CT bone scan is shown in Figures 4 and 5. This patient has primary breast cancer with bone metastases at several sites, including the skull, ribcage, right pedicle of the T12 vertebra, right hemipelvis, and right inferior pubic ramus. The prior bone scintigraphy study using 99mTc-phosphate failed to show the full extent of these bone metastases.
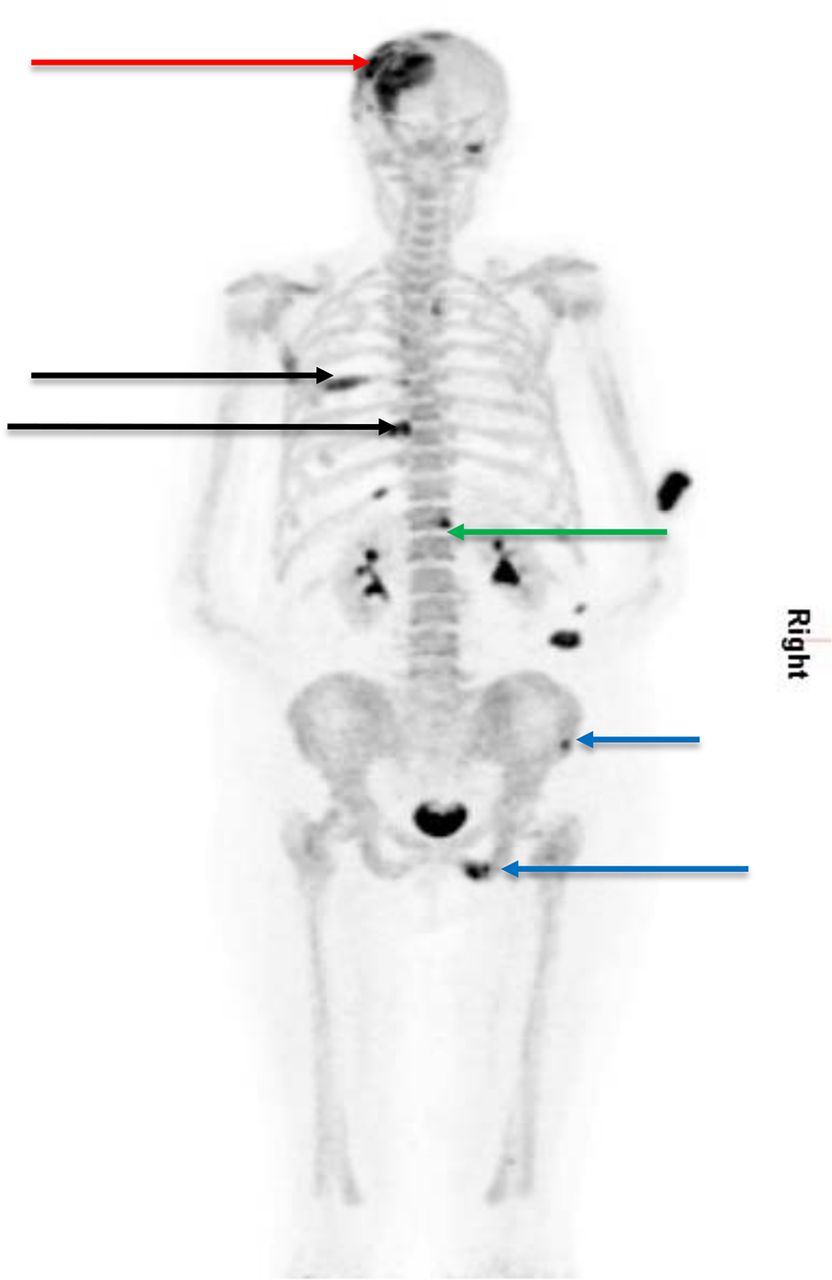
Maximum-intensity-projection 18F-NaF PET/CT bone scan (posterior view) shows bone metastases in left frontoparietal skull near vertex (red arrow), left posterior ribs (black arrows), right pedicle of T12 (green arrow), and right hemipelvis (blue arrows) that were not seen clearly on a previous planar bone scan. (Courtesy of Department of Nuclear Medicine, Royal Liverpool Hospital, Liverpool, U.K., 2016.)
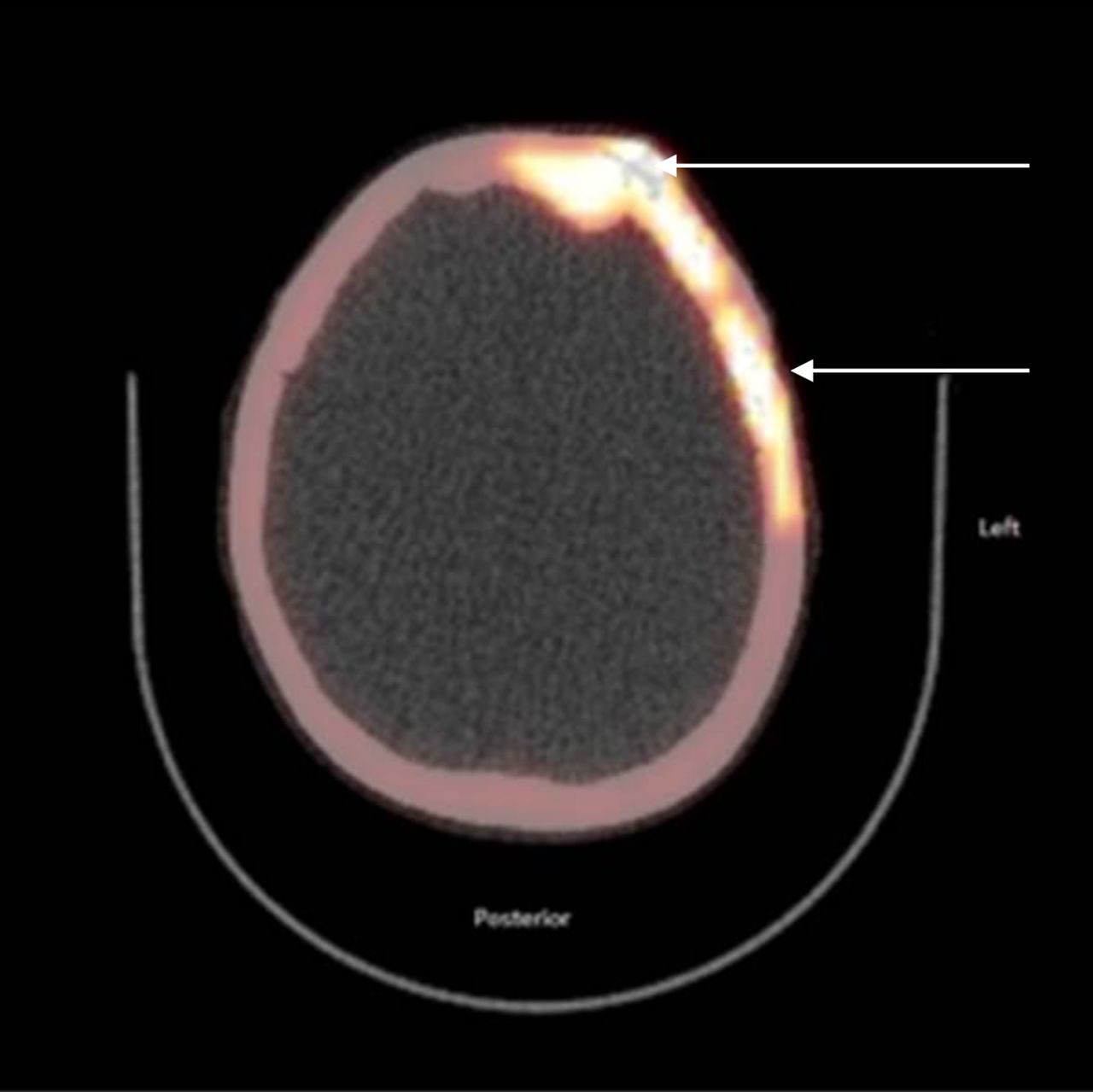
Axial fused 18F-NaF PET/CT bone scan of same patient as in Figure 4 shows left frontoparietal skull metastasis for which the CT component clearly reveals bony involvement (arrows). (Courtesy of Department of Nuclear Medicine, Royal Liverpool Hospital, Liverpool, U.K., 2015.)
Figures 6 and 7 show an example of a false-positive 18F-NaF PET/CT study in which the low-dose CT portion demonstrated benign pathology. This patient also had primary breast cancer, with a lesion in the right sacroiliac joint being identified on 18F-NaF PET/CT as a potential metastasis. On further diagnostic CT and MR scanning, this lesion was found to be a benign sclerotic fibroosseous lesion.

False-positive maximum-intensity-projection 18F-NaF PET/CT scan shows lesions in left upper cervical region (black arrow) and right iliac bone region close to right sacroiliac joint (red arrow). (Courtesy of Department of Nuclear Medicine, Royal Liverpool Hospital, Liverpool, U.K., 2015.)

Axial fused 18F-NaF PET/CT bone scan shows degenerative change in upper left cervical facet joint (arrow), corresponding to lesion seen in this area on previous maximum-intensity-projection image. (Courtesy of Department of Nuclear Medicine, Royal Liverpool Hospital, Liverpool, U.K., 2015.)
CONCLUSION
This article has described the history and main use of 18F-NaF in detecting bone metastases, primarily from breast cancer but also from prostate cancer. 18F-NaF PET/CT is more accurate than traditional planar bone scintigraphy or SPECT/CT, produces images of superior quality, and allows for a greater throughput of patients. The low-dose CT portion is good at excluding benign disease, and the greater accuracy reduces the number of anxious waiting periods for patients who would otherwise require extra testing (e.g., plain film radiography or diagnostic CT or MR scanning). The limitations of 18F-NaF must also be kept in mind, including a small number of false-positive results and an increase in radiation dose.
The main challenges in putting 18F-NaF imaging into more widespread use are its high cost and its worldwide lack of reimbursement, as well as referring clinicians’ lack of awareness of the procedure. It is hoped that these challenges will be overcome in the coming years by increased availability to hospitals and increased acceptability by clinicians.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Sep. 15, 2016.
CE credit: For CE credit, you can access the test for this article, as well as additional JNMT CE tests, online at https://www.snmmilearningcenter.org. Complete the test online no later than December 2019. Your online test will be scored immediately. You may make 3 attempts to pass the test and must answer 80% of the questions correctly to receive 1.0 CEH (Continuing Education Hour) credit. SNMMI members will have their CEH credit added to their VOICE transcript automatically; nonmembers will be able to print out a CE certificate upon successfully completing the test. The online test is free to SNMMI members; nonmembers must pay $15.00 by credit card when logging onto the website to take the test.
REFERENCES
- Received for publication May 22, 2016.
- Accepted for publication August 15, 2016.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Assessment of Bone Lesions with 18F-FDG PET Compared with 99mTc Bone Scintigraphy Leads to Clinically Relevant Differences in Metastatic Breast Cancer Management
- A Half-Century of Nuclear Medicine
- 18F-Sodium Fluoride PET: History, Technical Feasibility, Mechanism of Action, Normal Biodistribution, and Diagnostic Performance in Bone Metastasis Detection Compared with Other Imaging Modalities