


Abstract
The present prospective study evaluated the diagnostic value of a standardized analysis of 123I-N-ω-(fluoropropyl)-2β-carbomethoxy-3β-(4-iodophenyl)tropane (FP-CIT) SPECT studies acquired on a triple-head γ-camera for patients with clinically uncertain movement disorders having tremor as the most striking feature. Methods: 123I-FP-CIT studies were performed on 52 consecutive patients (27 male and 25 female; mean age, 49.2 y; range, 17–80 y) who had a clinical diagnosis of Parkinson's disease (PD) (n = 21), hypokinetic rigid syndrome (n = 19), dystonia (n = 8), or essential tremor (n = 4). In all patients, the final diagnosis was based on a thorough clinical examination, the family history, and a 2-y follow-up. Two independent technologists analyzed 123I-FP-CIT studies using a standardized quantitative method applying both fixed regions of interest (ROIs) and manually drawn ROIs. The mean values from both methods were compared using the Student t test, and the intra- and intertechnologist variabilities were tested. Results: In patients with PD, all ratios were significantly lower (P < 0.001) than those in patients with other movement disorders. No significant differences were found between the other groups tested. The manual method resulted in significantly lower values than did the standardized method (P < 0.001) and, for the putamen, showed significant differences between technologists. The standardized method showed no significant differences between technologists. The intra- and intertechnologist variabilities for this method were 0.14 ± 0.13 (confidence value, 2.4%) and 0.19 ± 0.18 (confidence value, 3.1%), respectively, whereas the intraclass correlation coefficients were 0.99 for 1 technologist and 0.98 for the 2 independent technologists. Conclusion: Our data confirm that 123I-FP-CIT SPECT has value in the differentiation of PD from other movement disorders. Acquisition using a triple-head γ-camera and subsequent standardized analysis using fixed ROIs result in good intra- and intertechnologist agreement and can easily be applied in clinical practice.
Parkinson's disease (PD) is a well-known and well-described disorder that involves movement, cognition, and emotion (1,2). Because degeneration of dopamine-containing cells is found in many different movement disorders, including PD, diagnosis of PD may be difficult. Especially in the early phase of PD, the diagnoses most commonly mistaken for it are progressive supranuclear palsy, multiple-system atrophy, essential tremor, vascular parkinsonism, and even Alzheimer's disease (3–6). Juvenile-onset dystonia that improves after treatment with levodopa may occur both in dopa-responsive dystonia (DRD) and in juvenile parkinsonism, clinically similar conditions with different prognoses and managements. In all cases, a close clinical examination, the family history, and follow-up are required to establish the diagnosis, but in some patients a proper diagnosis still cannot be made. In such cases, postmortem evaluation of the dopaminergic degeneration in the striatum is the only way to confirm the clinical suspicion.
The use of dopamine transporter imaging with 123I-N-ω-(fluoropropyl)-2β-carbomethoxy-3β-(4-iodophenyl)tropane (FP-CIT) for differentiating PD from essential tremor has been studied extensively over the past 10 y (7–11). This radiolabeled tracer has the advantage of having faster kinetics than do other cocaine analogs, providing the opportunity for imaging studies to be performed 70–240 min after injection. Results obtained with 123I-FP-CIT have been reliable and reproducible in showing a reduction of presynaptic tracer uptake. Furthermore, the uptake has been found to correlate with the duration and severity of PD. In most of these studies, however, brain-dedicated SPECT systems were used (12). These systems consist of 12 individual crystals, each equipped with a focusing collimator. Data on the reproducibility of nondedicated SPECT systems are scarce.
In the present prospective study, we investigated the value of 123I-FP-CIT in patients with a clinically uncertain diagnosis of a movement disorder. The studied patients had PD, essential tremor, hypokinetic rigid syndrome, or dystonia, with tremor as the most striking feature. In a subgroup of patients who underwent 123I-FP-CIT studies in clinical practice, we evaluated a standardized method of quantitative analysis using fixed regions of interest (ROIs) and compared the results with those obtained using manually drawn ROIs.
MATERIALS AND METHODS
123I-FP-CIT studies were performed on 52 consecutive patients (27 male and 25 female; mean age, 49.2 y; range, 17–80 y) with movement disorders who had a clinical diagnosis of PD (n = 21), hypokinetic rigid syndrome (n = 19), dystonia (n = 8), or essential tremor (n = 4). In all patients, the diagnosis was based on a thorough clinical examination, the family history, and follow-up. To assess the clinical diagnosis, we followed these patients for 2 y after the imaging study. All subjects received potassium iodide orally to block thyroid uptake of radioactive iodide.
Imaging Procedure
Data acquisition began 3 h after the patient had received an intravenous injection of 185 MBq of 123I-FP-CIT. A triple-head γ-camera (GCA9300/hg; Toshiba) equipped with high-resolution fanbeam collimators was used. Data were acquired for 60 s per projection in a 256 × 256 matrix applying a step-and-shoot method (120 projections). Before the acquisition, the orbitomeatal line was registered with a laser beam.
After the acquisition had finished, the fanbeam projections were converted to parallel projections. This conversion included reduction of the matrix to 128 × 128, resulting in 90 parallel projections. The conversion also involved filtering of the data by a Butterworth low-pass filter (order, 8; cutoff frequency, 0.30 cycles per pixel) to preserve the total counts in the study. After the fanbeam-to-parallel conversion, tomographic reconstruction using an ordered-subset expectation maximization algorithm began, applying 2 iterations, 10 subsets, and Butterworth prefiltering (order, 8; cutoff frequency, 0.15 cycles per pixel). The tomographic reconstruction delivered 40−50 transaxial slices of 1-pixel (∼2-mm) thickness. Each of these slices was 2 pixels (∼4 mm) thick, with an overlap of 1 pixel.
Image Analysis
Image analysis included semiautomatic selection of the slice to be analyzed and positioning of the ROI around the striatum. The program first calculated the total activity within a square ROI in the center of each slice. The slice with the highest activity within this square ROI was assumed to include the striatum. This slice was viewed on a screen, and a technologist positioned around the striatum an ROI (obtained from an anatomic atlas) that could not be changed in shape, size, or rotation. The program then determined the slice with the highest activity within this fixed ROI and used that central slice and the 2 adjacent slices to obtain the uptake of 123I-FP-CIT in the caudate nucleus and putamen. Use of overlapping slices enabled accurate selection of the slices of interest, by proceeding at steps of only 1 pixel through the reconstructed volume. After selection of the slices, the technologist could adapt the position of the ROI in each slice separately.
When all ROIs had been positioned correctly, the uptake was calculated for each selected slice in the left and right caudate nucleus and the left and right putamen. Next, the results for the corresponding ROIs were combined to determine the uptake in the left and right caudate nucleus and the left and right putamen separately. In addition, these counts were corrected using recovery coefficients obtained in a head-to-head comparison of the triple-head camera and a Strichman camera, which was used on an Alderson phantom to provide a reference database. For each study, the deviation from the mean value was calculated. The mean deviation and its SD were then calculated over all studies. The whole procedure was performed once by 2 independent technologists and twice by 1 technologist to assess the intra- and intertechnologist variabilities and to calculate the intraclass correlation coefficient. This value was defined as a measure of the consistency or agreement between values within cases. In addition to this semiautomatic procedure, a generally comparable manual method was tested. However, instead of positioning the fixed ROIs, 2 experienced technologists manually drew ROIs around the putamen and caudate nucleus and around the occipital cortex. The ROIs were mirrored to the opposite side, and the ratios obtained with this method were corrected using the same recovery coefficients as were used for the semiautomatic method. Finally, the results for technologists 1 and 2 were compared, and the results for the manual and semiautomatic methods were compared.
Recovery Coefficients and Normal Uptake Ratios
To assess the results obtained clinically with the triple-head γ-camera, we performed a phantom study using an Alderson phantom—an anthropomorphic basal ganglia phantom commercially available from Radiology Support Devices Inc. This phantom consists of symmetric chambers simulating each caudate nucleus (4.8 mL) and each putamen (6.0 mL) and a large chamber simulating the remaining brain (1,290 mL), all shaped according to the anatomy of the normal human brain. The chambers are surrounded by an artificial skull and soft tissue, with attenuation coefficients equivalent to those of human tissue. For an accurate head-to-head comparison of the different camera and collimator combinations, 6 activity concentrations of 123I were used, resulting in different specific ratios between the striatum and background regions. The activities ranged from markedly decreased radiotracer binding to high normal results. All solutions were prepared in identical vials before the phantom SPECT acquisition. The acquisition parameters were the same as those described in “Imaging Procedure.” All activity concentrations were measured 4 times so that mean uptake ratios could be calculated. The ratios acquired with the triple-head camera were corrected using true specific ratios acquired with a dedicated Strichman camera. These reference data were provided by the Department of Nuclear Medicine of the Academic Medical Center in Amsterdam. The acquisition parameters for these reference data and the results for healthy volunteers have been described previously (9,13). Finally, to assess the clinical value of the ratios measured in the current study, the reference uptake ratios were used: In patients less than 40 y old, the normal uptake ratios are 8.2 (SD ± 2.4) and 9.2 (SD ± 3.7) for the caudate nucleus and putamen, respectively; in patients more than 40 y old, the values are 7.8 (SD ± 3.5) and 8.3 (SD ± 3.7), respectively.
RESULTS
During the 2-y follow-up, the initial clinical diagnosis was not changed: 21 patients with PD and 31 patients with other movement disorders. In none of the patients were significant differences found between the left and right caudate nucleus or the left and right putamen. In patients with PD, all ratios were significantly lower (P < 0.001) than those in patients with other movement disorders. No significant differences were found between the other groups tested (Table 1).
Uptake Ratios on 123I-FP-CIT Studies Based on Standardized Analysis Method
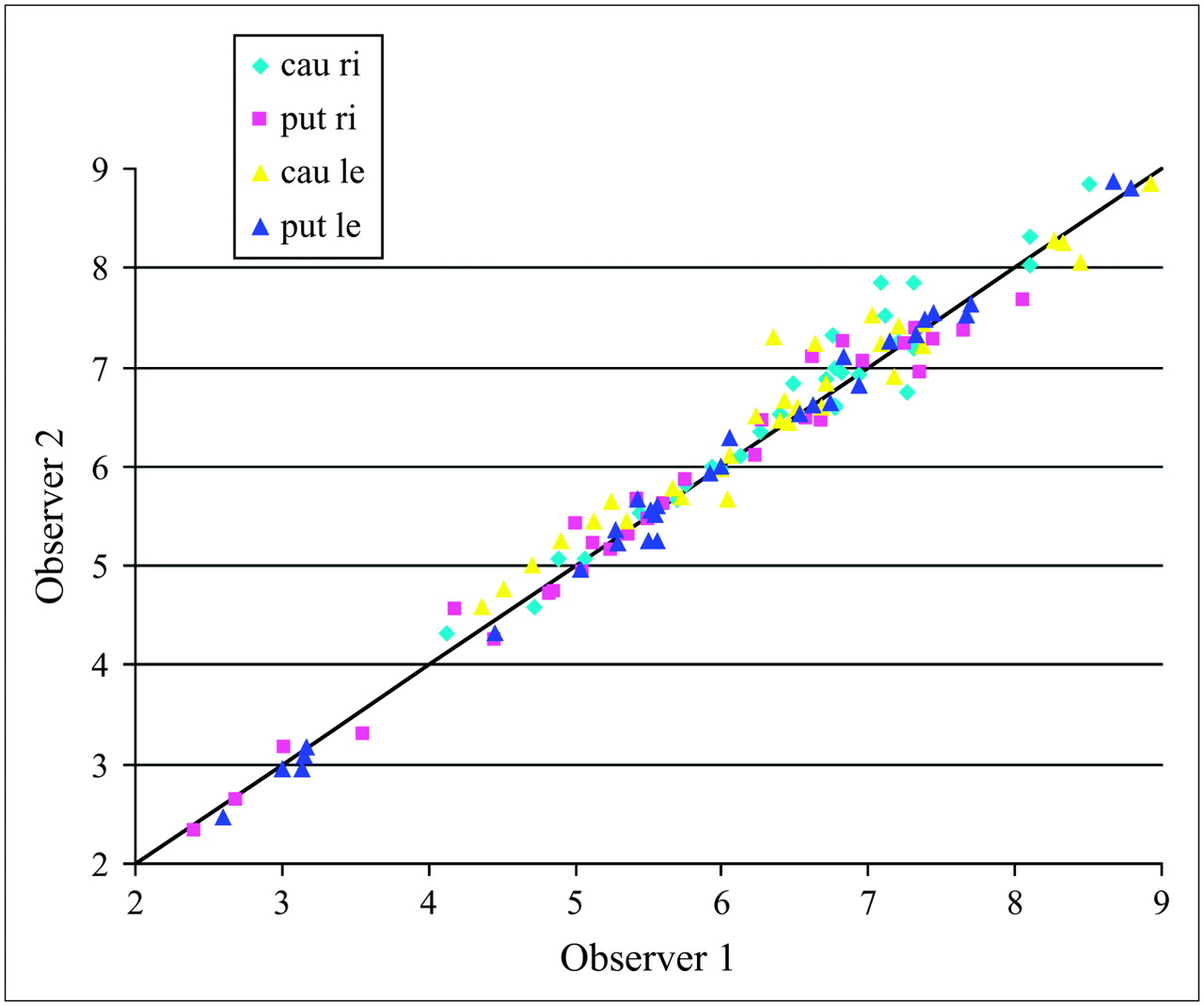
Overall, the manual method resulted in significantly lower uptake values for both the putamen and the caudate nucleus than did the standardized method using fixed ROIs. Furthermore, for the manual method, the mean uptake ratios for the putamen differed significantly between the 2 technologists (P = 0.002 and 0.014 for the right and left putamen, respectively). The values for the caudate nucleus were not significantly different (P = 0.892 and 0.703 for the right and left caudate nucleus, respectively). The results with the standardized method correlated well between the different technologists (Fig. 1). All mean uptake ratios, irrespective of the site, were comparable (Table 2), and the intra- and intertechnologist variabilities were 0.14 ± 0.13 and 0.19 ± 0.18, respectively. The intraclass correlation coefficients were 0.99 for 1 technologist and 0.98 for the 2 independent technologists. In Figure 2, the absolute difference between technologists 1 and 2 is plotted against the mean ratio for both and confirms the good reproducibility of the method. The absolute difference between the methods was less than 10% of the mean. In this respect, no correlation was seen between the mean ratio and the difference. In none of the patients studied with the semiautomatic method did the difference between the technologists result in a different classification. However, as shown in Table 2, we found significant differences between the manual method and the semiautomatic method on the one hand and between technologist 1 and technologist 1 for the manual method on the other hand. The most significant differences in ratios between technologists 1 and 2 for the manual method were in the left and right putamen. That finding is important because the putamen represents the site of early-onset PD. As can be seen in Table 2, false-positive results can be obtained for uptake ratios, which are significantly lower than the normalized values.
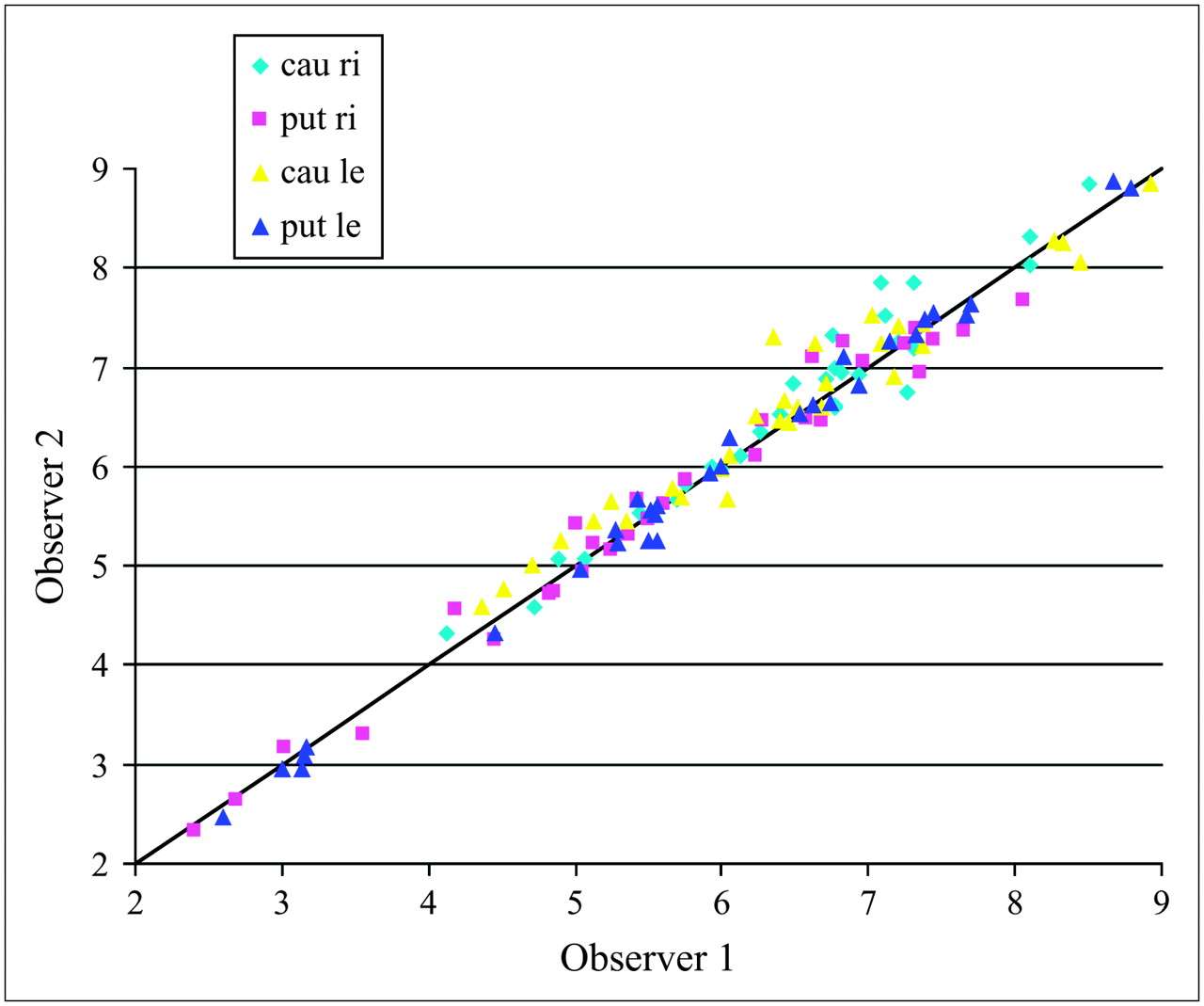
Correlation between results obtained from 123I-FP-CIT studies by 2 technologists (observers 1 and 2). Intra- and intertechnologist variabilities were 0.14 ± 0.13 (confidence value, 2.4%) and 0.19 ± 0.18 (confidence value, 3.1%), respectively. Cau le = left caudate nucleus; cau ri = right caudate nucleus; put le = left putamen; put ri = right putamen.
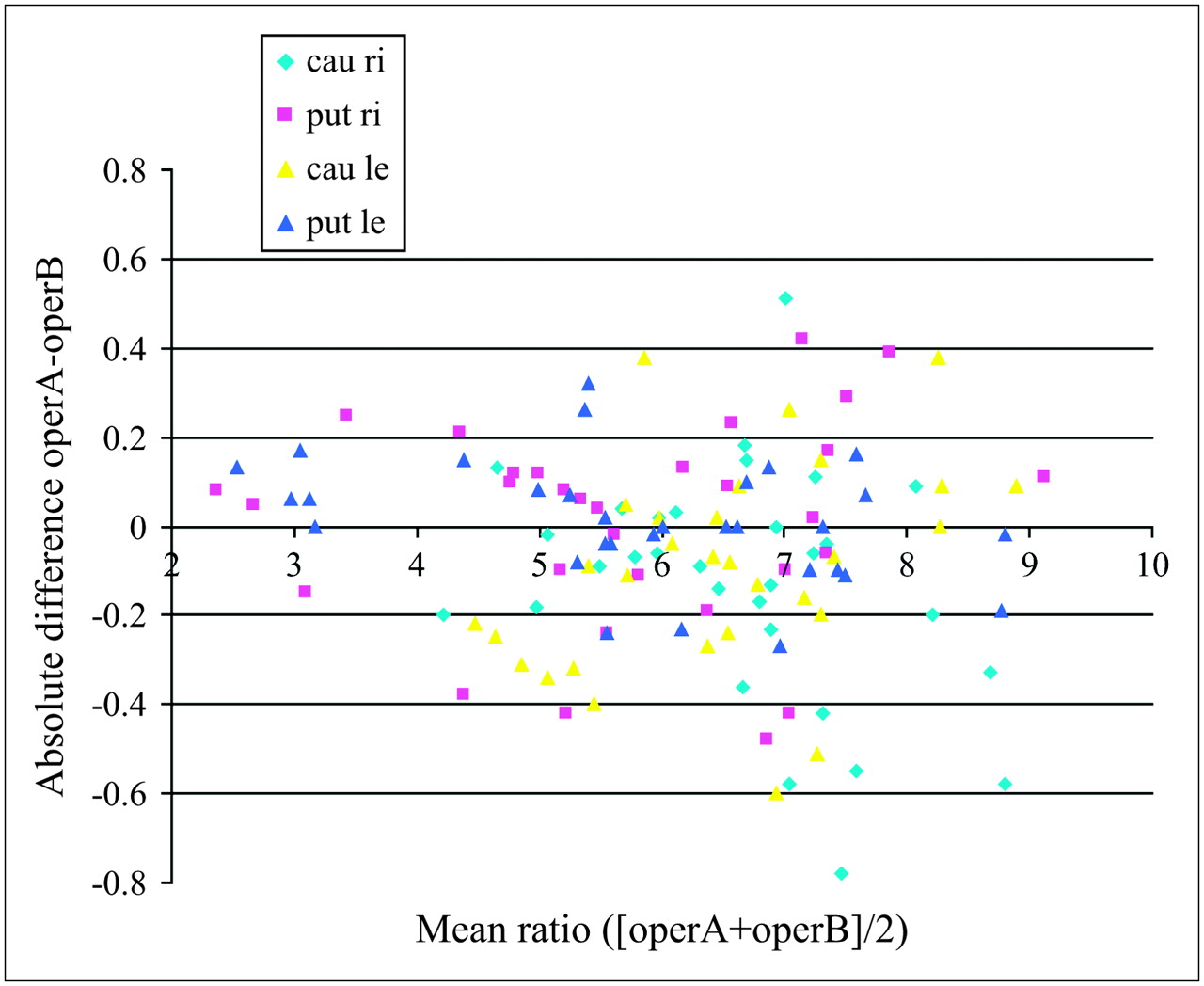
Absolute difference between 2 technologists plotted against mean ratio of both, confirming good reproducibility of method used in current study. Intraclass correlation coefficients, defined as measure of consistency or agreement of values within cases, of 1 technologist was equal to 0.99. This value for 2 independent technologists was equal to 0.98. Cau le = left caudate nucleus; cau ri = right caudate nucleus; operA = technologist 1; operB = technologist 2; put le = left putamen; put ri = right putamen.
Difference Between Mean Values Obtained with Fixed ROIs and Manually Drawn ROIs in Analysis of 123I-FP-CIT Studies
Figure 3 shows an example of a patient with essential tremor and normal uptake values, an example of a patient with diminished uptake in the caudate nucleus suggesting early-onset PD, and an example of a patient with diminished uptake in the whole striatum, corresponding to PD.

Uptake values as obtained using automatic semiquantitative method of analysis. (A) Normal uptake in putamen and caudate nucleus of patient with essential tremor. (B) Patient with diminished uptake in caudate nucleus, suggesting early-onset PD; 2-y follow-up confirmed hypothesis. (C) Patient with diminished uptake in whole striatum, corresponding to PD.
DISCUSSION
In the present study, we evaluated the use of a standardized analysis program that applies fixed ROIs in the assessment of different movement disorders. Because of the fixed shape and size of the ROIs, the technologist has the option only of translating the ROIs, resulting in good intra- and intertechnologist variability. Most important, this method showed clinical value in differentiating between PD and other movement disorders with similar features. Although a manual method of drawing and selecting ROIs is commonly used in clinical practice, the present study showed that, in comparison with the semiautomatic method, the manual method will result in significantly different outcomes between technologists. Moreover, the manual method may result in false-positive results in the diagnosis of early-onset PD. In general, when compared with the semiautomatic method, the manual method underestimated uptake values in the left and right putamen.
PD is a distinct clinical and neuropathologic disease characterized by bradykinesia, resting tremor, rigidity, and postural reflex impairment. Degeneration of pigmented cells, most prominently in the substantia nigra pars compacta, with associated Lewy bodies, is the chief pathologic feature of this disease. Symptoms become apparent when about 70%–80% of striatal dopamine neurons and about 50% of nigral dopamine neurons are lost (14,15). In the early stage, this disease may be difficult to differentiate from essential tremor (6), a common but complex neurologic movement disorder that usually affects the hands. Most people with essential tremor have both a postural and a kinetic tremor, whereas patients with PD have a resting tremor that decreases when the extremity is used. Dystonia is a neurologic movement disorder characterized by involuntary muscle contractions that force certain parts of the body into abnormal, painful movements or postures (4,16–18). Dystonia may affect any part of the body, including the arms and legs, trunk, neck, eyelids, face, and vocal cords. It is the most common movement disorder after PD and essential tremor (19). Symptoms may appear minor, such as cramps after exercise, or may present later in life in a form that more closely resembles PD. Moreover, lower-limb dystonia that improves with levodopa treatment is also a common feature in juvenile parkinsonism and results from depletion of nigrostriatal dopaminergic neurons (20). Finally, hypokinesia and rigidity are frequent symptoms of PD but also of multiple-system atrophy and progressive supranuclear palsy (2,5). These entities are well defined and correlate with a loss of dopamine transporters, D2 receptors, or both. However, these symptoms may also be related to Alzheimer's disease, dementia with Lewy bodies, Steele-Richardson-Olszewski syndrome, l-dopa–responsive infantile rigid parkinsonism due to tyrosine hydroxylase deficiency, or other conditions (21–23). From this fact, one can conclude that in certain cases PD may be difficult to differentiate from essential tremor, hypokinetic rigid syndrome, and dystonia—symptoms or syndromes that closely resemble the initial stage of PD. The present study evaluated the results of follow-up dopamine transporter imaging performed to evaluate the initially presumed diagnosis. In all patients with PD, the scans revealed significantly decreased uptake. Patients diagnosed with essential tremor, DRD, or hypokinetic rigid syndrome had normal scan findings, which excluded degeneration of the presynaptic dopaminergic system.
Over the past 12 y, data have become available on the value of 123I-FP-CIT SPECT in the early diagnosis of PD (10,24–32). One of these studies clearly described the clinical benefit of imaging dopamine transporters in differentiating patients with presynaptic parkinsonism from those with other forms of parkinsonism. In that study, by Booij et al., 33 inconclusive cases were evaluated (33). A follow-up of 3 y was used to confirm the scintigraphic data. True-positive and -negative rates of 100% and 92%, respectively, were observed. One of the most important findings was that all patients with essential tremor had normal scan results. In other words, 123I-FP-CIT can be used to differentiate between PD and essential tremor. Our present results, showing a significant decrease in uptake in PD, agree with the data in the literature. Other reports from the study group of Booij et al. have pointed to a possible effect of age and sex on transporter imaging in healthy volunteers but not in PD patients (8,9,11). The investigators described a significant age-dependent decline of approximately 4% per decade in binding ratios. These results were used to set the normal values applied in the present study.
Two case reports have described the use of 123I-FP-CIT to differentiate between DRD and PD in patients with dystonia. O'Sullivan et al. described a 17-y-old patient with a clinically atypical case of DRD highly suggestive of juvenile PD (16). Normal uptake was seen on the SPECT study, and the family history and several years of follow-up finally confirmed the diagnosis of DRD. Katzenschlager et al. described a patient with exercise-induced dystonia (34). Despite a thorough neurologic and orthopedic examination, a clear diagnosis could not be made. 123I-FP-CIT SPECT revealed a bilateral, asymmetric reduction of striatal tracer uptake. During follow-up, mild stiffness and resting tremor developed, and criteria consistent with PD were finally fulfilled. Other studies have shown that patients with dementia with Lewy bodies also had significantly decreased uptake in the striatum. Dementia with Lewy bodies is one of the main differential diagnoses of Alzheimer's disease (30,35). A definitive diagnosis can be made only by histopathologic examination of the brain. Like PD, however, dementia with Lewy bodies shows a loss of nigrostriatal dopaminergic neurons, ranging from 40% to 70%, on postmortem studies.
CONCLUSION
Our data confirm the value of 123I-FP-CIT SPECT in the differentiation of PD from other movement disorders that may mimic PD. Normal uptake in patients with essential tremor, hypokinetic rigid syndrome, or DRD—entities that may resemble early-stage PD—can be used to exclude PD. The combination of a standard γ-camera and a standardized analysis, as used in the present study, results in good intra- and intertechnologist agreement. The analysis based on fixed ROIs and standard methods of reconstruction can easily be applied in clinical practice; does not have the absolute prerequisite of a dedicated camera system; and, compared with the manual method of analysis, increases diagnostic accuracy and minimizes interpretation errors. Because manually drawn ROIs may result in lower uptake values and false-positive results, we strongly recommend the standardized method for the assessment of movement disorders.
Acknowledgments
We thank the Department of Nuclear Medicine of the Academic Medical Center, Amsterdam, The Netherlands, for providing their 123I-FP-CIT reference data.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication February 20, 2006.
- Accepted for publication November 28, 2006.





{kind=link}
{kind=link}
{kind=link}