


Visual Abstract

Abstract
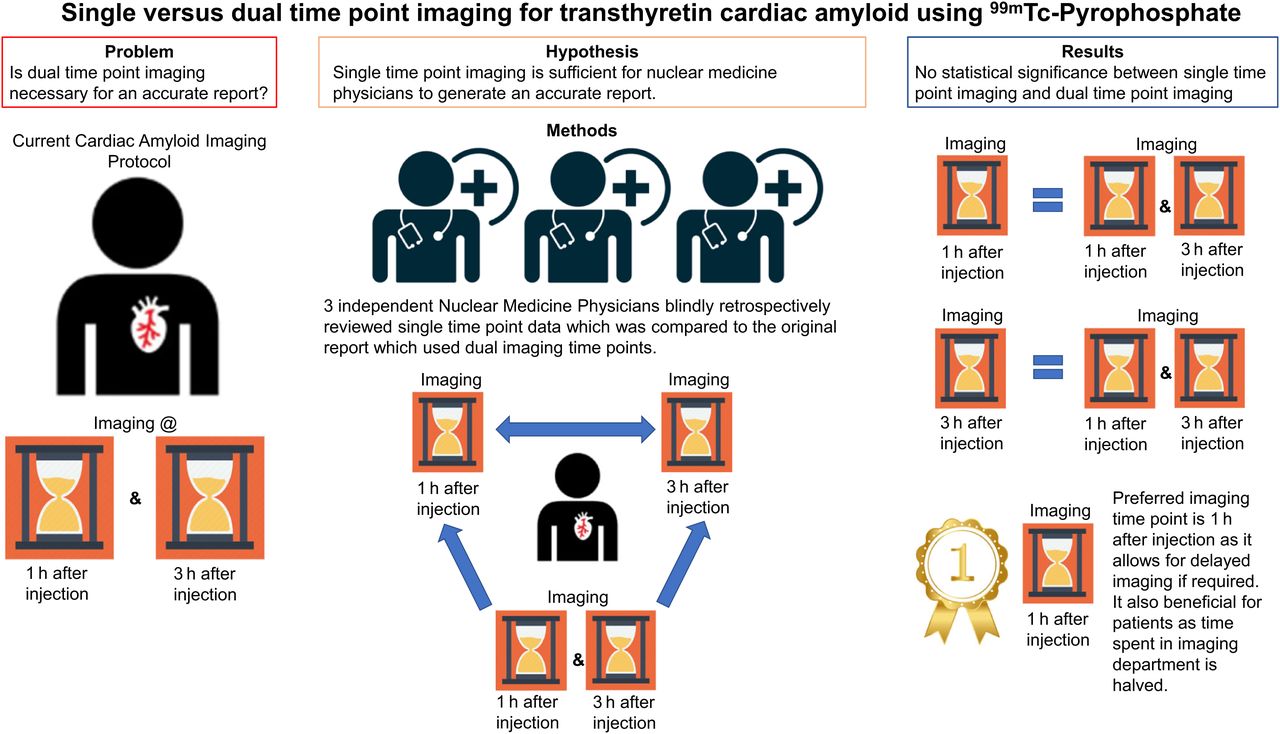
Nuclear medicine scintigraphy using 99mTc-pyrophosphate has proven valuable in the diagnosis of cardiac transthyretin amyloidosis in recent years. However, there is still confusion over the optimal imaging time points. The American Society of Nuclear Cardiology has recommended different imaging time points over the last decade. We aimed to determine whether single- or dual-time-point imaging is required for reporting purposes and which time point would be the most appropriate if a single time point was to be considered. Methods: Cardiac amyloid scans using 99mTc-pyrophosphate acquired from 2017 to 2023 were retrieved from our Picture Archiving and Communications System. Scans with static views and SPECT/CT images of the chest for both imaging time points, at 1 h (early) and 3 h (delayed) after injection, were included. Each study was independently read by 3 nuclear medicine physicians. Original clinical reports using both imaging time points were used as a reference to calculate the accuracy of a single time point. Results: In total, 70 patients were included in this study. Reports of cardiac amyloid studies using any single-time-point imaging were highly sensitive, accurate, and specific. There was agreement among all readers. Of the 140 datasets reported by each reader, 4 scans were classified as equivocal, requiring more imaging for confident reporting. Conclusion: Single-time-point imaging showed an accuracy comparable to the dual-time-point imaging in diagnosing cardiac transthyretin amyloidosis. This was further validated by agreement among the 3 readers. Early time-point imaging is preferred, and additional delayed imaging can be acquired when the early result is equivocal.
Footnotes
Published online Apr. 22, 2025.
This article requires a subscription to view the full text. If you have a subscription you may use the login form below to view the article. Access to this article can also be purchased.
SNMMI members
Login to the site using your SNMMI member credentials
Individuals
Login as an individual user
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.