


Abstract
Histiocytic sarcoma (HS) is a rare malignancy with morphologic and immunophenotypic features indicating histiocytic differentiation. We present a case of HS with multisystem involvement, including an obstructing mass in the pancreatic head. 18F-FDG PET/CT is a valuable tool in staging this rare entity and in assessing the response to therapy. Knowing the diverse metastatic pattern of HS will help avoid imaging pitfalls on clinical 18F-FDG PET/CT scans.
Histiocytic sarcoma (HS) is a rare neoplasm of myeloid-derived macrophages. The exact etiology is unclear. It occurs predominantly in adults and is associated with poor survival (1). HS may involve lymph nodes and many organs and is hypermetabolic on 18F-FDG PET/CT. Diagnosis of HS relies on demonstration of histopathologic evidence of histiocytic differentiation, that is, CD68 and CD163, and exclusion of other malignancies, including large B-cell lymphoma, T/NK-cell lymphoma, and other histiocytic and dendritic neoplasms.
CASE REPORT
A 51-y-old woman presented with progressively worsening back pain. Thoracic spine MRI demonstrated a large mass centered at the T7 level and bilaterally infiltrating the T7 and T8 neural foramen, as well as adjacent ribs. The patient underwent T6–T8 decompression and tumor debulking to relieve back pain. Histopathologic evaluation of the intraspinal, extradural mass lesion demonstrated large anaplastic cells, mitotic activity, and admixed lymphocytes and eosinophils. Immunohistochemical stains showed the large tumor cells to be positive for CD4, CD10, CD45, CD68, and CD163 and negative for markers of a plasma cell neoplasm (CD138 immunoglobulin light-chain–negative), Hodgkin lymphoma (CD30 and CD15), Langerhans cell sarcoma (CD1a), and dendritic cell sarcoma (CD21 and CD35). A diagnosis of HS was established.
Shortly after surgery, the patient presented with acute pain in the right upper quadrant and around the stomach, which worsened after meals, as well as jaundice and pruritus. Contrast-enhanced CT showed an ill-defined mass in the pancreatic head, with dilation of the bile duct and the main pancreatic duct. On 18F-FDG PET/CT, there were multiple hypermetabolic lesions, including the mass in the pancreatic head (Fig. 1). The patient underwent 3 cycles of chemotherapy under the CHOP regimen (cyclophosphamide, doxorubicin, vincristine, and prednisolone) and demonstrated a favorable response to therapy.
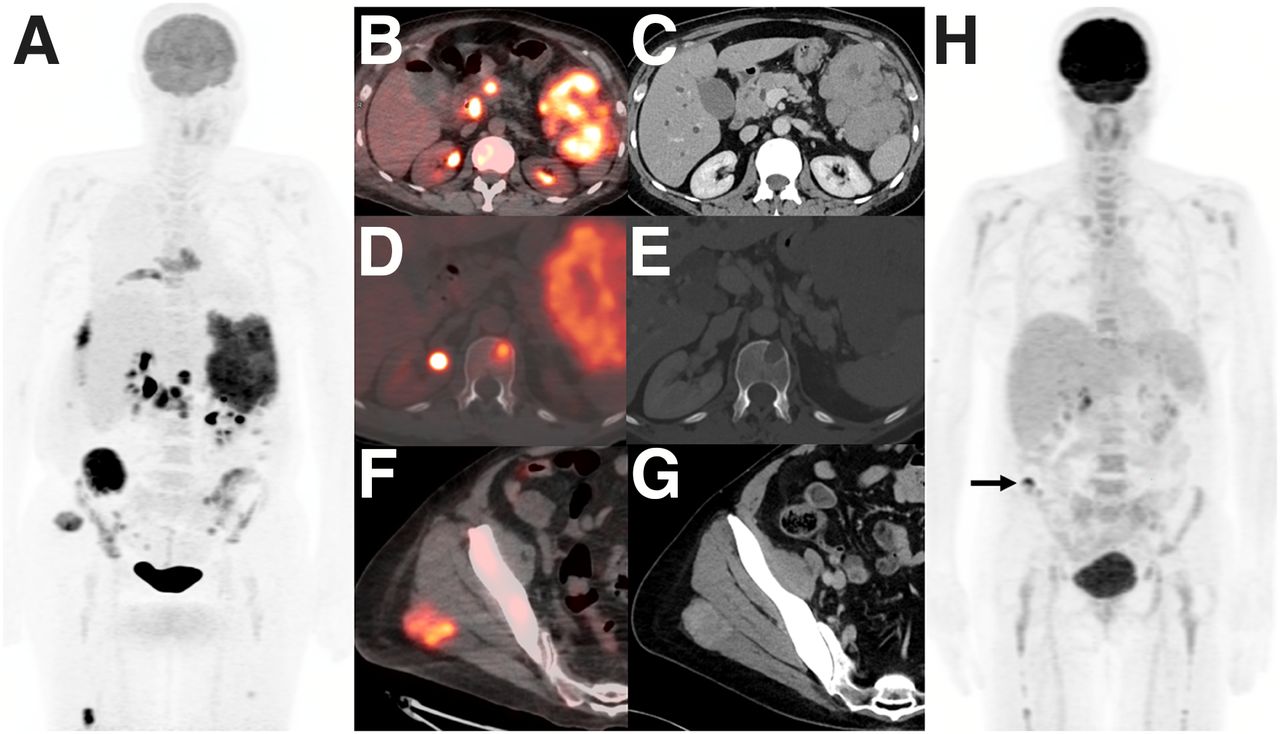
(A–G) On staging 18F-FDG PET/CT maximum-intensity projection (A), PET/CT fusion, and corresponding contrast-enhanced diagnostic CT images, there are multiple hypermetabolic metastases, including obstructive mass in pancreatic head and large mass lesion in left upper quadrant (B and C), lytic lesion in T12 vertebral body (D and E), and lesion in right gluteus maximus muscle (F and G). (H) After 3 cycles of chemotherapy, follow-up 18F-FDG PET/CT showed near-complete response and small, residual tracer-avid focus in right iliac wing (arrow).
DISCUSSION
HS is a rare histiocyte disorder with a slight male predominance (2). Since HS may involve multiple systems, its clinical manifestation varies and may present as multifocal hypermetabolic extranodal disease on 18F-FDG PET/CT (2–4). Pancreatic involvement in HS is extremely rare and may mimic other pancreatic malignancies. Ultimate diagnosis of HS relies on histopathologic evidence of histiocytic differentiation within involved tissue and exclusion of other malignancies, including large B-cell lymphoma and other histiocytic and dendritic neoplasms (5). There is no standard treatment for HS, and the CHOP regimen might be acceptable for multifocal disease. Although HS might exhibit a favorable response to chemotherapy, the long-term survival rate is poor (1). 18F-FDG PET/CT may allow us to delineate the extent of HS, guide biopsy, and assess treatment response.
CONCLUSION
It is important to be familiar with the widespread multisystem pattern of HS. 18F-FDG PET/CT is a valuable tool in staging and surveillance of this rare entity.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online July 30, 2021.
REFERENCES
- Received for publication March 5, 2021.
- Revision received April 15, 2021.





{kind=link}