


Abstract
We performed a 68Ga-DOTATOC PET/CT scan on a 25-mo-old female patient who presented with opsoclonus myoclonus ataxia syndrome and had negative initial anatomic imaging. The scan showed a somatostatin receptor-overexpressing cervical tumor in favor of a cervical neuroendocrine tumor, with subsequent histopathologic findings of ganglioneuroblastoma.
Neuroblastic tumors have been found to develop anywhere along the sympathetic nervous chain and are divided into 3 histologic categories—ganglioneuroma, ganglioneuroblastoma, and neuroblastoma—ranging from mature to immature tumors (1). The median age at diagnosis is 17 mo (2,3). Ganglioneuroblastomas account for 20% of neuroblastic tumors (4). Ganglioneuroblastomas arising from the neck are exceptionally rare (5).
Opsoclonus myoclonus ataxia syndrome (OMAS) is a rare neuroinflammatory disorder with multiple etiologies, and the neural-crest paraneoplastic etiology is the most common (6).
It was found that 68Ga-DOTA-peptide PET/CT is the imaging modality of choice for well-differentiated neuroendocrine tumors because of its ability to locate the primary lesion and identify the extent of disease (7).
In the literature, we found a limited number of cervical ganglioneuroblastoma cases (only 16 cases) (5). We were unable to locate any case in which 68Ga-DOTA-peptide PET/CT screening was used to diagnose cervical ganglioneuroblastoma. The objective of this case report is to demonstrate the value of 68Ga-DOTATOC PET/CT in the diagnosis of cervical ganglioneuroblastoma while screening for clinically suspected neuroblastic tumors in a child who presented with OMAS. Institutional review board approval was waived for this case.
CASE REPORT
The pediatric unit referred a 25-mo-old girl with OMAS for a 68Ga-DOTATOC PET/CT scan to screen for a potential neuroblastic tumor. The patient first underwent a contrast-enhanced torso CT scan, which was reported to be unremarkable.
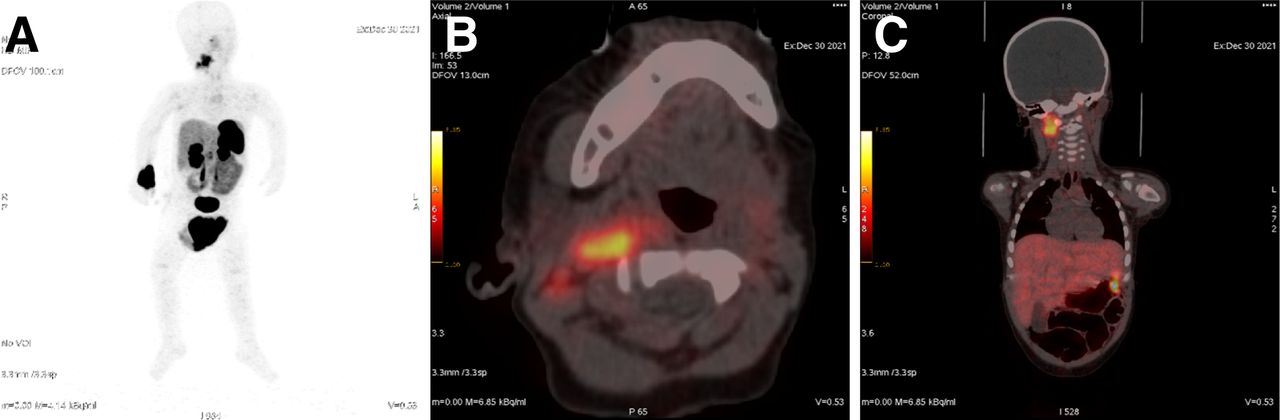
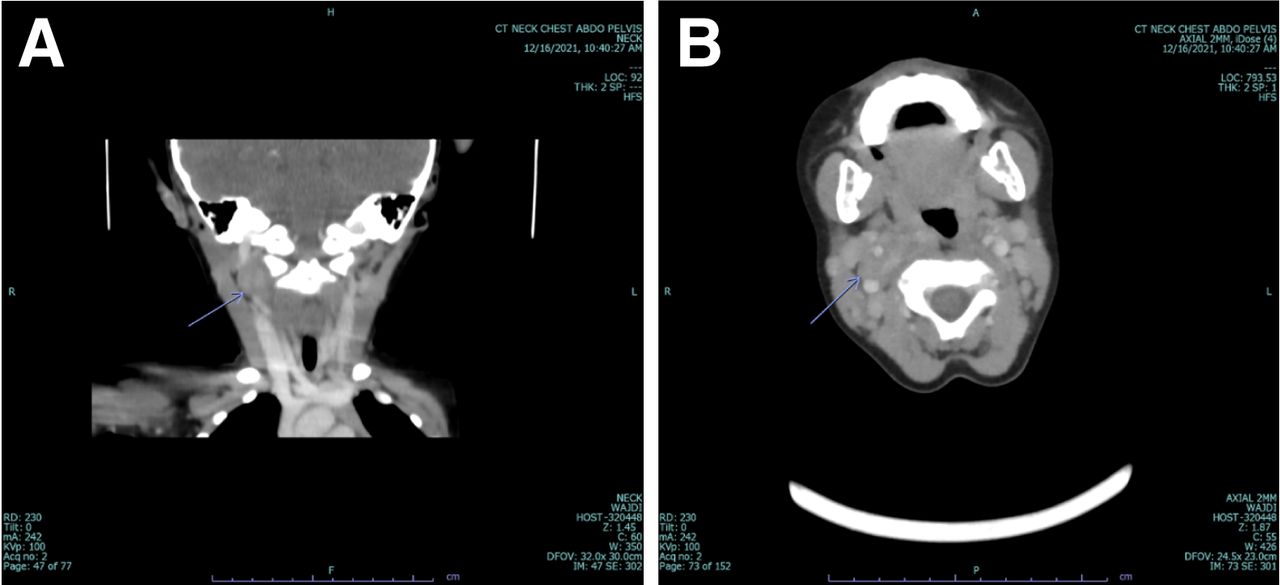
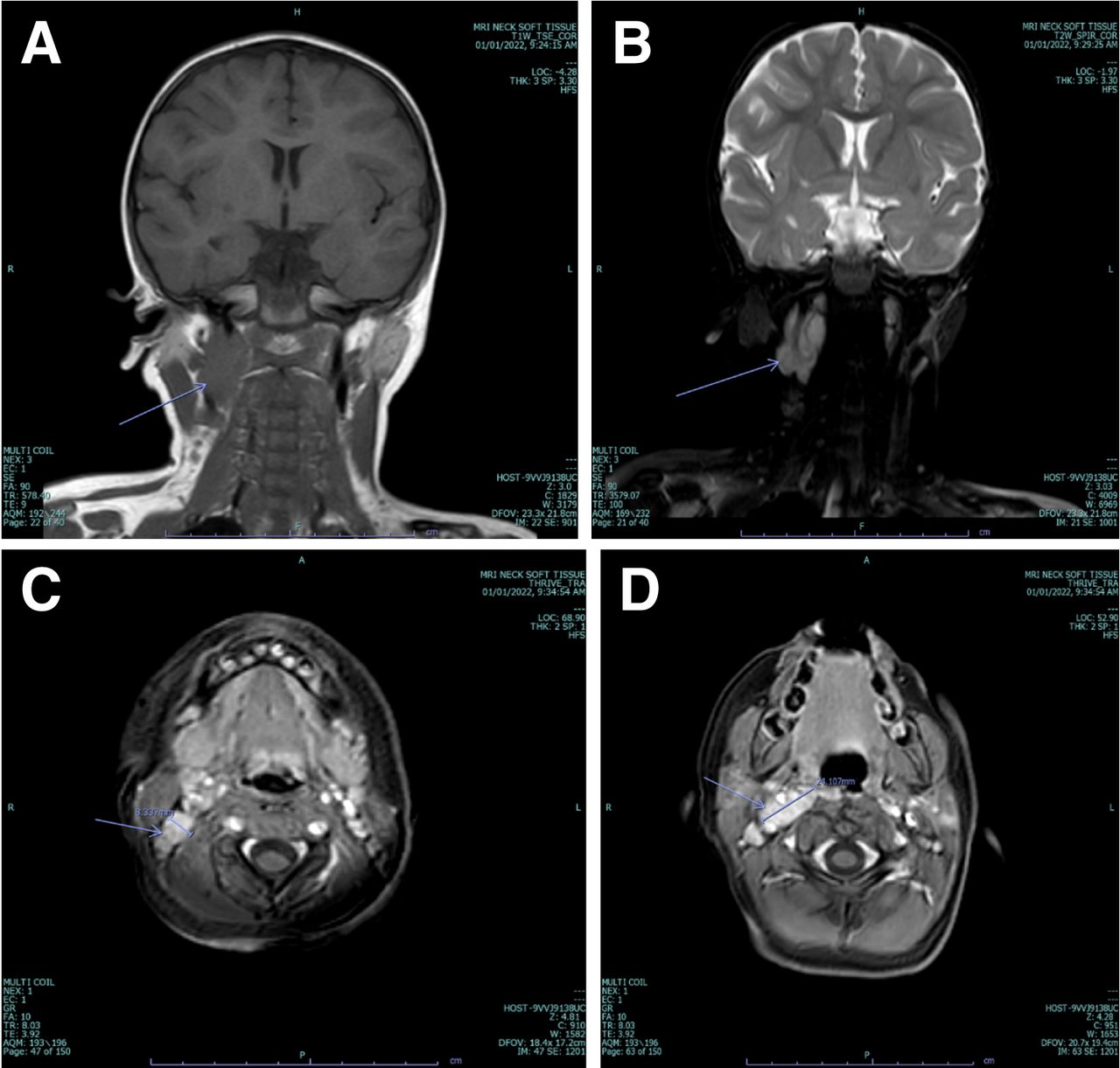
A 68Ga-DOTATOC PET/CT scan was performed afterward, revealing a tracer-avid soft-tissue mass in the right upper cervical region that was compatible with a somatostatin receptor-overexpressing tumor, in favor of a cervical neuroendocrine tumor. In addition, the scan revealed a tracer-avid enlarged right upper cervical lymph node suggestive of metastatic lymphadenopathy (Fig. 1). The scan was negative for tracer-avid distant metastases. A second look at the previously performed CT scan confirmed that there was a slightly enhanced soft-tissue mass in the right jugulodigastric region (Fig. 2). Neck MRI showed a well-defined heterogeneous soft-tissue mass measuring 1 × 2.1 × 2.7 cm that had high T2 and low T1 signal intensities and was enhanced on the postcontrast T1 sequence. The mass extended from the skull base to the level of the C2 vertebra, with an extension into the right retropharyngeal space and partial encasement of the right internal carotid artery (Fig. 3). Also, the neck MRI revealed pathologic upper cervical lymph nodes.

68Ga-DOTATOC PET/CT images (PET maximum-intensity projection, A; axial view, B; coronal view, C) showing tracer-avid right upper cervical mass.

Contrast-enhanced CT images (coronal view, A; axial view, B) showing slightly enhanced soft-tissue mass in jugulodigastric region (arrow).

Neck MRI showing right upper cervical mass (arrows) that is low signal on T1 sequence (coronal view, A), high signal on T2 sequence (coronal view, B), and enhanced on postcontrast T1 sequence (axial views, C and D).
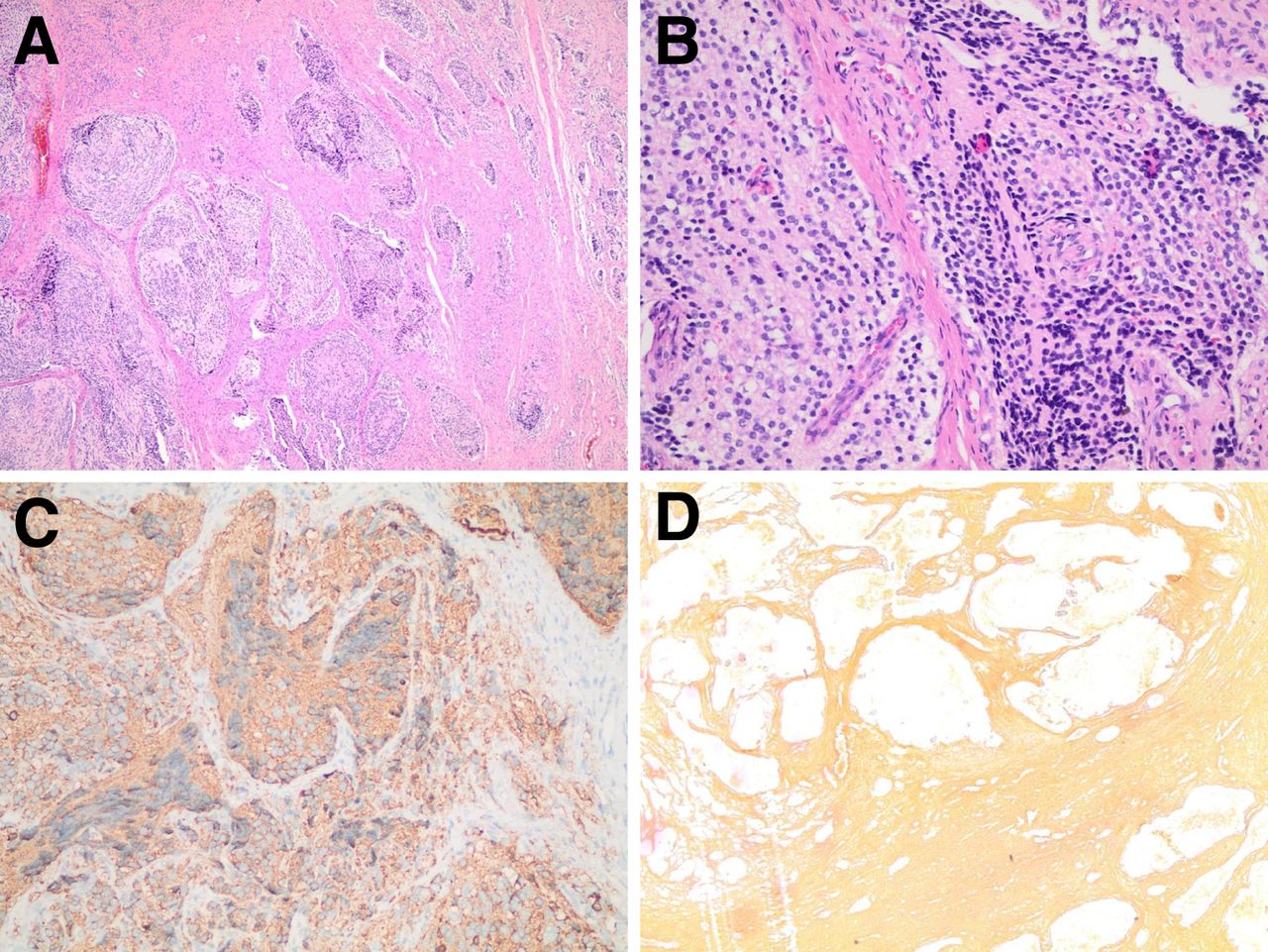
Partial surgical resection was performed. Histopathology showed a nodular subtype of ganglioneuroblastoma (Fig. 4).

(A and B) Histopathology showing nodules composed of stroma-poor islands of primitive cells with fibrillary neuropil matrix. (C) Synaptophysin staining in tumor cells. (D) Reticulin stain highlights nested pattern.
DISCUSSION
Our patient presented with OMAS, which is an immune-mediated condition that may be paraneoplastic in the context of neuroblastoma. Peripheral neuroblastic tumors are found in 50% of children with OMAS. The most common tumor type is neuroblastoma (73%), followed by ganglioneuroblastoma (22%) and ganglioneuroma (4%) (8). Approximately 5% of peripheral neuroblastic tumors occur in the cervical region (5).
To our knowledge, this is the first case of cervical ganglioneuroblastoma that presented as paraneoplastic OMAS and was diagnosed by a 68Ga-DOTATOC PET/CT scan.
Our case demonstrates the great value of 68Ga-DOTA-peptide PET/CT scanning in screening for clinically suspected neuroblastic tumors in children, as these tumors commonly overexpress somatostatin receptors (7). Tracers currently in clinical use are 68Ga-DOTATOC, 68Ga-DOTATATE, and 68Ga-DOTANOC with high sensitivity (93%–96%) and high specificity (85%–100%) (9).
Our case is added to the 16 cases of cervical ganglioneuroblastoma reported in the literature. None of these 16 was diagnosed by 68Ga-DOTA-peptide PET/CT scanning.
CONCLUSION
We reported a rare case of cervical ganglioneuroblastoma manifested clinically as OMAS and diagnosed by a 68Ga-DOTATOC PET/CT scan of a 25-mo-old child.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Aug. 16, 2023.
REFERENCES
- Received for publication April 5, 2023.
- Revision received July 6, 2023.





{kind=link}
{kind=link}
{kind=link}
{kind=link}