


Abstract
Recommended 177Lu-DOTATATE treatment regimens involve prophylaxis with antiemetics to counteract the emetogenic properties of the nephroprotective amino acid solution infusion. We describe a 58-y-old woman treated with 177Lu-DOTATATE for metastatic small-bowel carcinoid, who was allergic to many classes of antiemetics. Therefore, she was treated with 177Lu-DOTATATE without antiemetic prophylaxis. She tolerated the compounded amino acid infusion of lysine and arginine, followed by 177Lu-DOTATATE, without significant nausea or any vomiting. We hypothesize that aggressive antiemetic prophylaxis may not be necessary if a 177Lu-DOTATATE patient receives compounded lysine/arginine amino acid solutions. The omission would decrease overall health-care costs and limit possible medication side effects.
DOTATATE with 177Lu (LUTATHERA; Advanced Accelerator Applications SA) is a peptide receptor radionuclide therapy used in gastroenteropancreatic neuroendocrine tumors. The regimen includes pretreatment with positively charged amino acids (AA) to prevent possible nephrotoxicity from 177Lu-DOTATATE retention. Nausea and vomiting are unfortunate side effects of the AA solution (1). Historically, commercial AA solutions resulted in significant nausea; however, new data suggest that compounded l-arginine and l-lysine AA solutions are significantly less emetogenic (2). Because of historic severe nausea and vomiting with commercial AA solutions, aggressive pretreatment with antiemetics is recommended (3). We present a case of a patient allergic to many antiemetic drugs, who successfully underwent 177Lu-DOTATATE therapy without the use of antiemetics.
CASE REPORT
The typical prophylactic antiemetic at our institution for 177Lu-DOTATATE patients is a combination of netupitant and palonosetron (Akynzeo; Helsinn Healthcare SA). We administer this drug 30 min before the AA infusion, followed by 177Lu-DOTATATE infusion 30 min later. For the AA renal-protective solution, we use a compounded solution of lysine and arginine, rather than the commercial AA solutions.
A 58-y-old woman presented to our clinic for her first 177Lu-DOTATATE cycle for metastatic small-bowel carcinoid that was progressive despite chronic long-acting octreotide therapy (Fig. 1). She had undergone resection of a low-grade ileal carcinoid tumor in 2005, followed by long-acting octreotide therapy. During consultation for the first treatment dose, the patient reported severe allergies to many classes of antiemetics, including the antiserotonergic class that we typically give to patients. After a discussion with the patient on the risks of not administering antiemetics, we decided to proceed with standard AA and 177Lu-DOTATATE (7.3 GBq) infusion without antiemetic prophylaxis. The 177Lu-DOTATATE infusion was performed using the standard technique outlined by the manufacturer. The patient denied experiencing any significant nausea or vomiting at any time during her infusion or at any time (checked at approximately 2-h intervals) during her overnight hospital admission. We imaged the patient the next morning per the standard protocol and allowed her to return home (Fig. 2). She denied experiencing nausea the next morning as well.
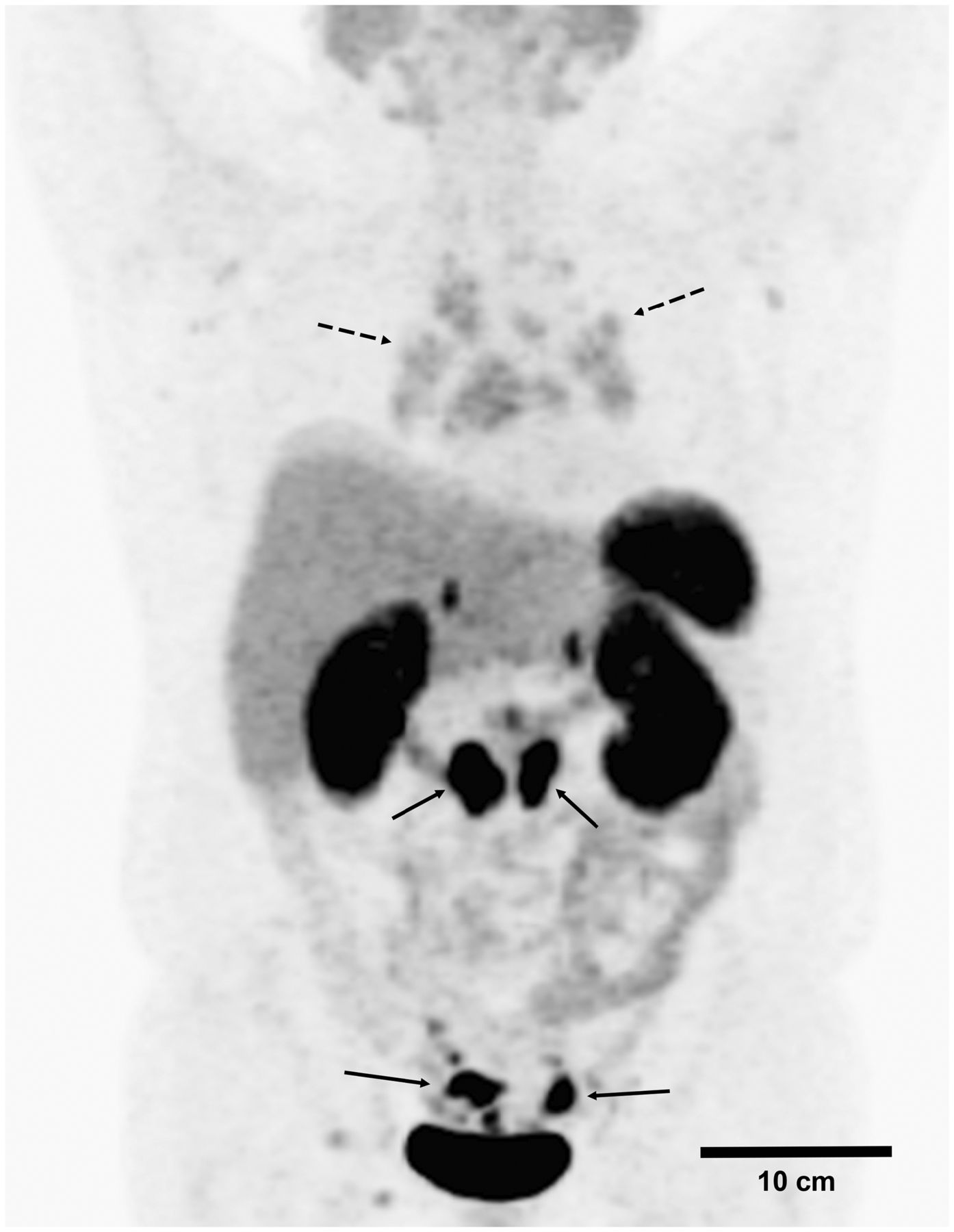
68Ga-DOTATATE PET/CT maximum-intensity projection demonstrating multiple radiotracer-avid abdominopelvic lymph nodes (solid arrows). Incidental mediastinal and hilar nodal uptake (dashed arrows) were felt to be due to underlying inflammatory condition, such as sarcoidosis.
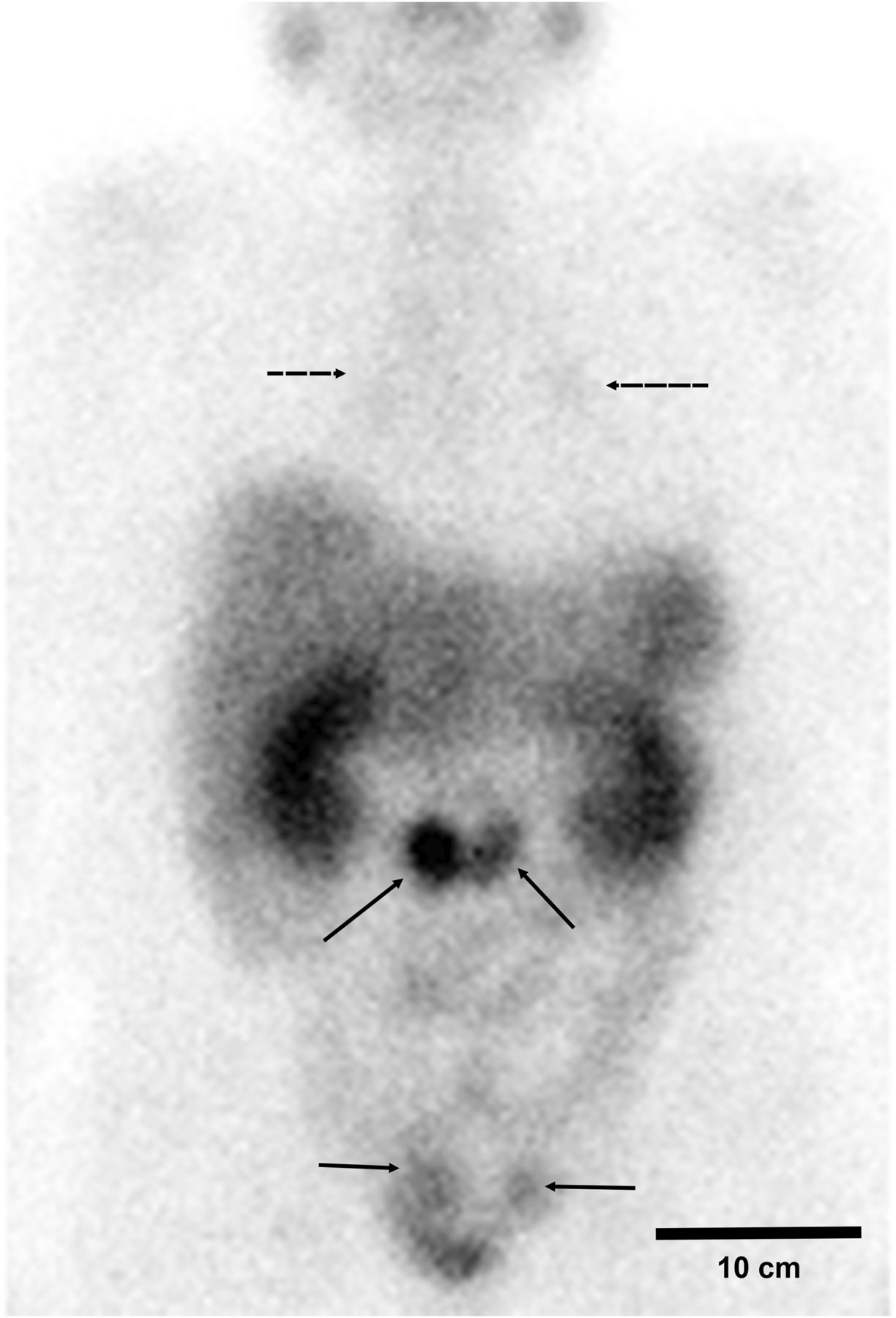
177Lu-DOTATATE (7.3 GBq) posttreatment anterior planar γ-image demonstrating pattern of uptake similar to that seen on prior 68Ga-DOTATATE PET/CT (Fig. 1), with abdominopelvic (solid arrows) and incidental mediastinal and hilar (dashed arrows) nodal uptake again noted.
DISCUSSION
Although omitting the antiemetic placed our patient at a higher risk for developing symptoms of nausea and vomiting, the compounded AA solution of lysine and arginine likely lowered the likelihood of symptoms (2). She was monitored closely but did not develop any significant nausea or vomiting symptoms at any time during her clinical course.
The recommended 177Lu-DOTATATE treatment regimen includes aggressive and potentially expensive antiemetic prophylaxis. The cash-paying cost (i.e., insurance costs of medications often differ from out-right cash costs from the manufacturer) of a single dose of the combination antiemetic Akynzeo is $683. Another possible problem with these antiemetics are side effects, including headache and fatigue.
CONCLUSION
Our patient with metastatic small-bowel carcinoid underwent 177Lu-DOTATATE therapy successfully despite the fact that, because of allergies, she did not receive antiemetics. We hypothesize that aggressive and potentially expensive antiemetic prophylaxis may not be necessary when infusing patients with a compounded AA solution of lysine and arginine. Further research into this matter is important to improve patient care and to reduce treatment costs.
DISCLOSURE
The views expressed here are those of the authors and do not reflect the official policy or position of Brooke Army Medical Center, the U.S. Army Medical Department, the U.S. Army Office of the Surgeon General, the Department of the Army, the Department of the Air Force, the Department of Defense, the Defense Health Agency, or the U.S. Government. No potential conflict of interest relevant to this article was reported.
Footnotes
Published online July 30, 2021.
- Received for publication January 23, 2021.
- Revision received April 13, 2021.





{kind=link}
{kind=link}