


Abstract
68Ga-prostate-specific membrane antigen (PSMA) ligands are novel PET radiotracers for prostate cancer. These radiotracers also localize in the normal renal cortex to a high degree and can demonstrate parenchymal defects. We recently started a prospective research study to compare 68Ga-PSMA-11 PET/CT with 99mTc-dimercaptosuccinic acid (DMSA) scan in adults with pyelonephritis. Here, we present a side-by-side comparison of renal cortical PSMA PET/CT and DMSA images of an adult patient with chronic recurring pyelonephritis. Methods: Our prospective study was approved by the Ethical Committees. DMSA images (multiple planar and SPECT) were obtained 3 h after intravenous injection of 111 MBq (3 mCi) of 99mTc-DMSA. On a separate day, we obtained PET/CT images of the kidneys 60 min after intravenous injection of 74 MBq (2 mCi) of 68Ga-PSMA-11 after the patient provided written informed consent. Results: The patient was a 46-y-old woman with history of chronic recurring pyelonephritis. Both DMSA scan and PSMA PET/CT demonstrated slight cortical thinning with mildly reduced uptake in the upper pole of the right kidney, with no significant cortical defects. There was an excellent distribution of activity in the renal cortex and better image resolution with PSMA PET than with DMSA scan. Non–attenuation-corrected PSMA PET images also showed the same findings, with reasonable image quality. Conclusion: In our first case, 68Ga-PSMA-11 PET imaging provided promising results in an adult patient with pyelonephritis. The results of our prospective study on a larger number of adult patients will provide a more accurate comparison of 68Ga-PSMA-11 PET to 99mTc-DMSA scanning in pyelonephritis.
Scanning with 99mT-dimercaptosuccinic acid (99mTc-DMSA) is widely used to demonstrate renal parenchymal changes in pyelonephritis, particularly in detecting renal sequelae (scar formation) at least 4–6 mo after acute infection (1–3). 99mTc-DMSA scanning is more commonly used in children than in adults. It is the current gold standard in detecting renal scarring but has certain limitations such as a relatively long waiting time after radiotracer injection; a long acquisition time, which is inconvenient for the patients; and the limited spatial resolution of γ-cameras. In addition, there has been a shortage of 99mTc-DMSA in certain countries, such as the United States, over the last few years (4).
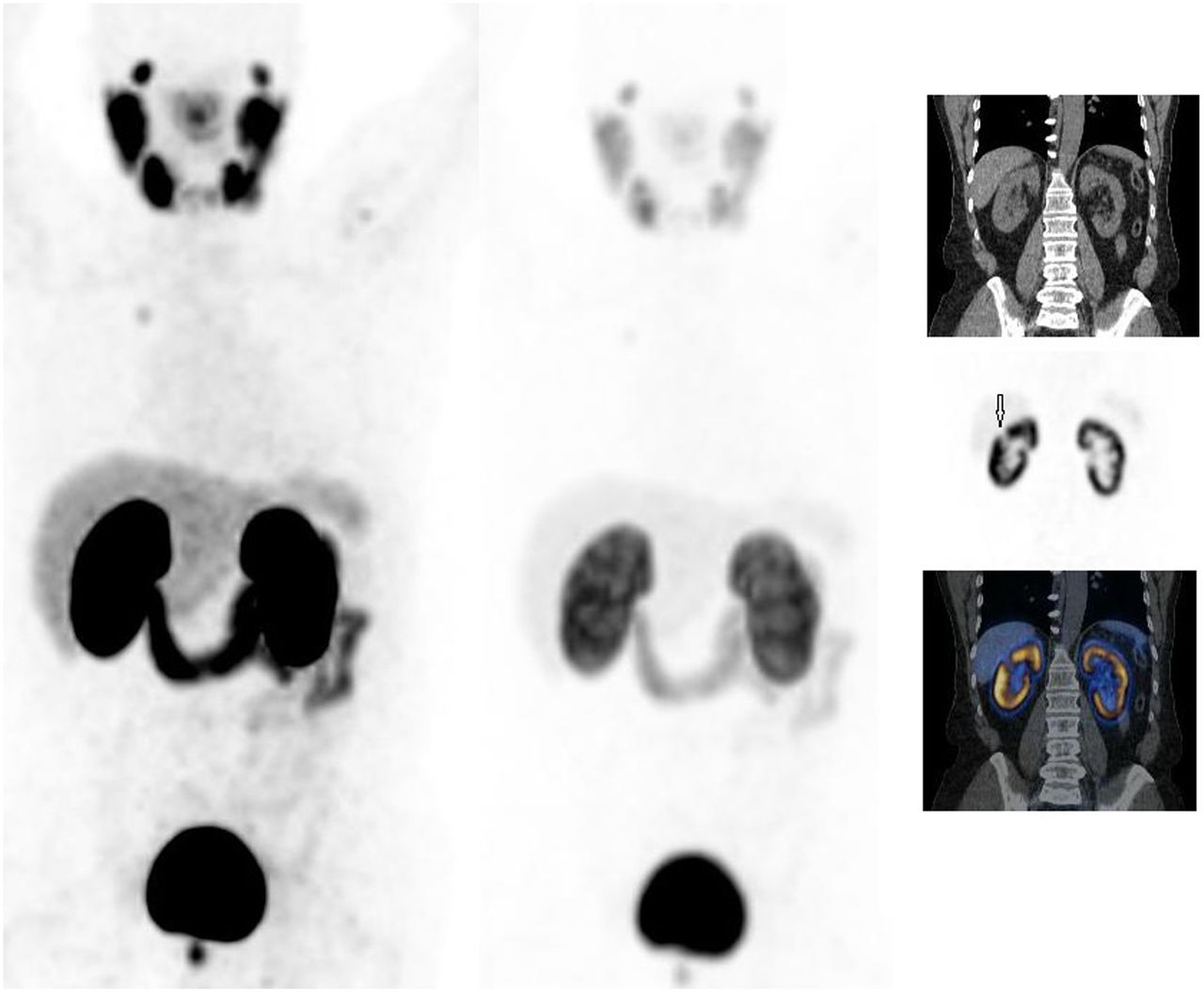
68Ga-labeled prostate-specific membrane antigen (68Ga-PSMA) ligands or inhibitors are novel PET radiotracers to image prostate cancer and its metastases (5–7). The physiologic biodistribution of 68Ga-PSMA ligands demonstrates uptake in various normal tissues, being highest in the kidneys and salivary glands (Fig.1). PSMA is a type II transmembrane protein with enzymatic activity (glutamate carboxypeptidase II) that is reported mainly in prostate tissue and is overexpressed in prostate cancer and in some extraprostatic normal tissues, including the kidneys and various other malignancies (8–10). In immunohistochemical analysis, detectable PSMA levels were identified in a subset of proximal renal tubules (8). PSMA expression was available in the brush borders and apical cytoplasm of a subset of proximal tubules (11). 68Ga-PSMA ligands bind to PSMA and internalized. They also inhibit enzymatic activity of PSMA.

In patient with prostate cancer, 68Ga-PSMA-11 maximum-intensity-projection PET images (in high-intensity setting [left] and low-intensity setting [middle]) and selected coronal CT image (top right), PET image (middle right), and PET/CT fusion image (bottom right) 2 h (image could not be obtained at 1 h due to unexpected delay) after intravenous injection of 129.5 MBq (3.5 mCi) of 68Ga-PSMA-11 demonstrate physiologic high renal uptake and excellent distribution of activity in renal cortex. Approximately 1-cm cyst (arrow) is cause of cortical defect in upper pole of right kidney.
Assessing the kidneys in low-intensity settings on 68Ga-PSMA PET images shows a high degree uptake of the radiotracer in the renal parenchyma and high-resolution images of the renal cortex (Fig.1) (12–14). In some of our patients with prostate cancer, 68Ga-PSMA PET also demonstrated renal parenchymal defects caused by various sizes of simple renal cysts—a finding that encouraged us to conduct a prospective study to compare 68Ga-PSMA PET with 99mTc-DMSA scanning in adults with pyelonephritis (12–14). Because of the coronavirus disease 2019 pandemic, our study is currently on hold, but we wanted to present the 68Ga-PSMA PET and 99mTc-DMSA images of our first case.
MATERIALS AND METHODS
Our prospective study was approved by the Ethical Committee of the Health Sciences Center at Kuwait University and by the Kuwait Ministry of Health. The study was conducted at Mubarak Al-Kabeer Hospital in Kuwait.
The patient provided written informed consent before the study. We obtained 68Ga-PSMA PET/CT and 99mTc-DMSA images from a 46-y-old woman with a 10-y history of chronic recurring pyelonephritis. In the previous 2 mo, the patient had an acute episode of pyelonephritis (with urine cultures positive for Escherichia coli) and was treated with 2 wk of antibiotics, which ended a few days before this study.
The 68Ga-PSMA ligand (PSMA-11) was radiolabeled at another institute (Radiopharmacy Unit at Kuwait Cancer Control Center) using a 68Ge/68Ga generator and a manual synthesis module (Isotope Technologies). 68Ga-PSMA ligands are investigational PET radiotracers and as of now have not been approved by the U.S. Food and Drug Administration or the European Medicines Agency. This was an off-label use of 68Ga-PSMA ligands for renal imaging.
99mTc-DMSA images were obtained 3 h after intravenous injection of 111 MBq (3 mCi) of 99mTc-DMSA using a Symbia S SPECT scanner (Siemens Healthineers) equipped with a high-resolution parallel-hole collimator. Multiple planar images were obtained in the anterior, posterior, right posterior oblique, and left posterior oblique projections (10 min each, 20% window centered at 140 keV, 256 × 256 matrix, and zoom of 1.3). After planar imaging, SPECT images of the kidneys were obtained (20-s acquisition per view, 60 views, 360° rotation, 128 × 128 matrix, no zoom, and 20% window centered at 140 keV). Images were reconstructed using a standard iterative algorithm and reformatted into transaxial, coronal, and sagittal views.
Three days after the 99mTc-DMSA scan, 68Ga-PSMA PET/CT images of the kidneys were obtained on a Philips Gemini time-of-flight PET/CT camera (Philips Medical Systems) 60 min after intravenous injection of 74 MBq (2 mCi) of 68Ga-PSMA ligand. We used a low activity to reduce the radiation dose to the patient and also because we had a limited amount of radiotracer. Before the PET image acquisition, a low-dose, unenhanced CT scan of the kidney region was obtained for attenuation correction, anatomic localization, and gross anatomic correlation purposes. The CT parameters included 30 mAs, 120 kV, pitch of 0.829, 0.5-s rotation time, 64 × 0.625 collimation, and 5-mm slice thickness. The PET acquisition time was 7 min/bed position for 2 bed positions. Because a low dose of activity was administered, the image acquisition time was longer than usual. The PET images were attenuation-corrected (AC) on the basis of the CT data, reconstructed using a standard iterative algorithm, and reformatted into transaxial, coronal, and sagittal views. Maximum-intensity-projection images were also generated. Because of intense activity in the kidneys, the PET images were reviewed in low intensity to better assess renal cortical uptake and distribution. Both AC and non-AC PET images, as well as PET/CT fusion and low-dose CT images, were evaluated to assess the anatomic location, size, and morphology of the kidneys; the uptake and distribution of radiotracer in the renal parenchyma; and the presence of any parenchymal defects or other abnormalities.
RESULTS
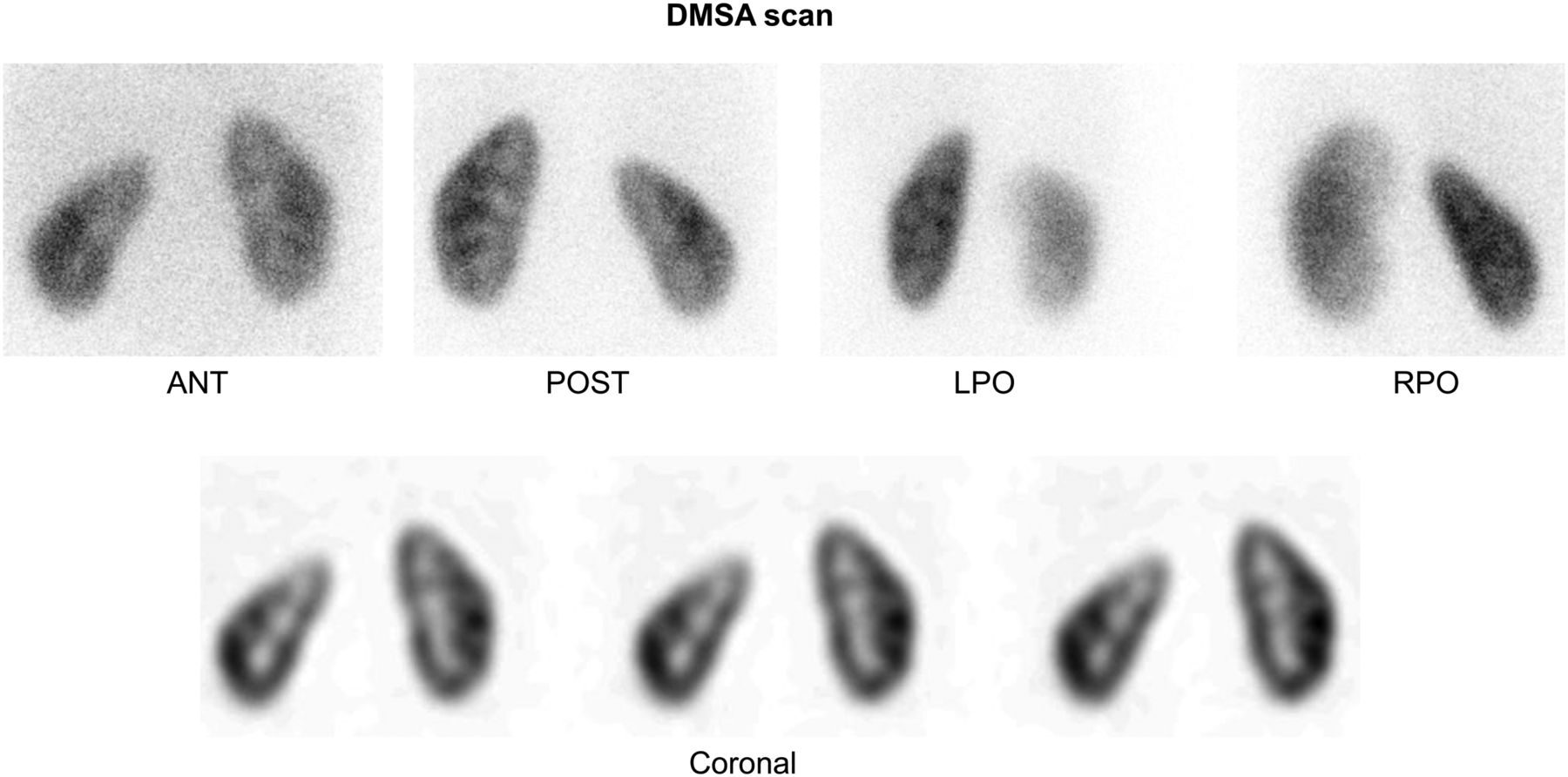
99mTc-DMSA images showed slight cortical thinning with mildly reduced uptake in the upper pole of the right kidney, with no significant cortical defects (Fig. 2).
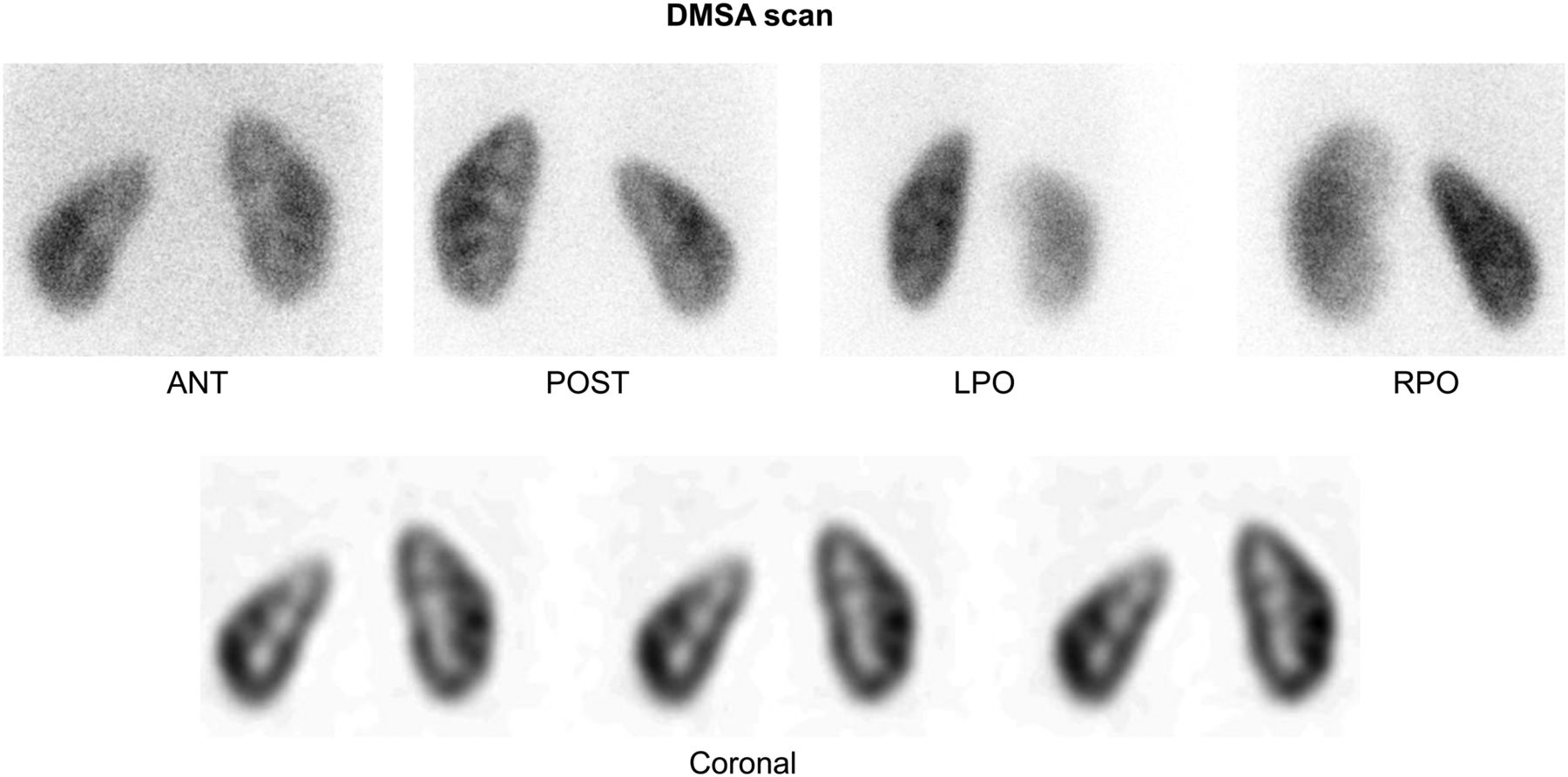
99mTc-DMSA multiple planar and selected coronal SPECT images demonstrate slight cortical thinning and mildly reduced activity in upper pole of right kidney, without significant cortical defect. ANT = anterior; POST = posterior; LPO = left posterior oblique; RPO = right posterior oblique.
68Ga-PSMA PET/CT images also showed slight cortical thinning and mildly reduced uptake in the upper pole of the right kidney, with no significant cortical defects (Fig. 3). Overall, there was an excellent distribution of activity in the renal cortices, with more prominent uptake in the renal columns on 68Ga-PSMA images. Image resolution was better with 68Ga-PSMA than with 99mTc-DMSA.
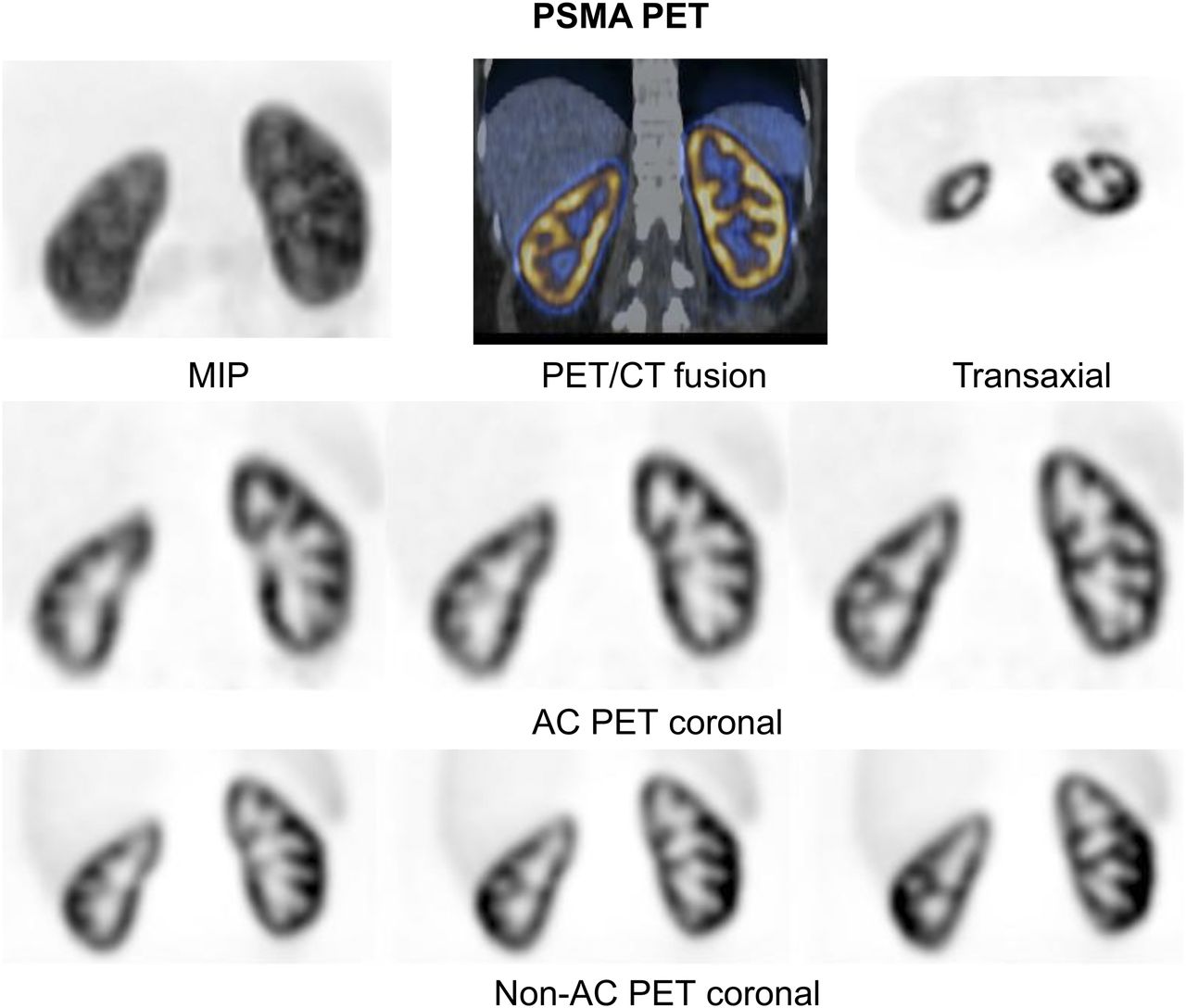
68Ga-PSMA-11 maximum-intensity-projection (MIP), PET, selected coronal PET/CT, fusion, transaxial and coronal AC PET, and coronal non-AC PET images with injected activity of 74 MBq (2 mCi) show slight cortical thinning and mildly reduced uptake in upper pole of right kidney, without significant defect. Images of renal cortex are of higher resolution with 68Ga-PSMA PET than with 99mTc-DMSA, as shown in Figure 2. Non-AC PET also provides good-quality images of kidneys.
Non-AC 68Ga-PSMA PET images showed the same findings, with reasonable image quality (Fig. 3).
Low-dose CT images did not show any simple cysts or calculi, which can cause parenchymal defects.
DISCUSSION
Side-by-side comparison of renal 68Ga-PSMA PET and 99mTc-DMSA images in our first case demonstrated that 68Ga-PSMA ligand is a promising radiotracer for renal cortical imaging. 68Ga-PSMA PET has certain advantages over 99mTc-DMSA scanning. The waiting period after radiotracer injection, and the image acquisition time, are less with 68Ga-PSMA PET than with 99mTc-DMSA scanning. Images are obtained approximately 3 h after 99mTc-DMSA injection and 1 h after 68Ga-PSMA ligand injection. The image acquisition time was approximately 14 min with 68Ga-PSMA PET/CT, as compared with 45 min (20 min for planar imaging, 25 min for SPECT) with 99mTc-DMSA scanning in our case. The 68Ga-PSMA PET image acquisition time was 7 min per bed position because a low dose of radiotracer was administered. The image acquisition time can be further reduced to 3–4 min with the administration of a higher activity. The longer acquisition time with 99mTc-DMSA scanning can cause patient discomfort and patient motion, which result in image artifacts and may require the acquisition of additional images and sedation in pediatric patients. 68Ga has a shorter half-life (approximately 68 min) than 99mTc (6 h). The absorbed kidney doses of 68Ga-PSMA-11 and 99mTc-DMSA in adults are 0.24 and 0.18 mGy/MBq, respectively (15,16), and the effective adult doses are 0.022 and 0.0088 mSv/MBq, respectively (15,16). An injected activity of 111 MBq (3 mCi) for 99mTc-DMSA and 74 MBq (2 mCi) for 68Ga-PSMA-11 yields an estimated effective dose of 0.98 and 1.63 mSv, respectively. Therefore, in adults, 68Ga-PSMA-11 results in a 66% higher exposure from the effective dose. if 74 MBq (2 mCi) is used. However, the amount of 68Ga-PSMA-11 activity may be further reduced with a longer acquisition time (e.g., 37 MBq [1 mCi] and a 10-min acquisition). There is an additional radiation dose from CT in PET/CT, but the CT has a low dose and covers only the kidney region. However, as the non-AC PET also provides good-quality images of the renal parenchyma, the low-dose CT can be omitted. PET scanners offer higher spatial resolution than γ-cameras and can detect smaller defects (17). In our case, image resolution was better with 68Ga-PSMA PET (PET/CT and non-AC PET) than with 99mTc-DMSA scanning (planar and SPECT). SPECT/CT is expected to provide higher-resolution images than SPECT, but because we wanted to reduce the radiation dose to our patient, we did not perform SPECT/CT. However, PET/CT is known to provide higher-resolution images than SPECT/CT. On the other hand, new SPECT systems with cadmium-zinc-telluride detectors have better resolution than conventional scanners with sodium iodide detectors.
The main limitations of 68Ga-PSMA PET imaging are a higher cost, and less global availability. The cost of 99mTc-DMSA scanning and 68Ga-PSMA PET varies among institutes and countries. At our institute, the cost of 99mTc-DMSA scanning and 68Ga-PSMA PET is approximately $292 and $454, respectively. However, there is currently a shortage of 99mTc-DMSA in certain countries. 99mTc-DMSA was added to the drug-shortages list of the U.S. Food and Drug Administration in 2014 and was commercially unavailable thereafter (4). New radiotracers for renal cortical imaging are needed as an alternative to 99mTc-DMSA or to replace it. In our early images, 68Ga-PSMA PET appears to have the potential to be an alternative to 99mTc-DMSA scanning. 68Ga-alizarin red S was also studied in animals and humans as a renal cortical PET radiotracer in the 1980s (18). 68Ga-PSMA PET provided results comparable to 99mTc-DMSA scanning in our adult patient, but we do not know its biodistribution and radiation dose in children. Further work, such as learning the mechanism of uptake and the physiologic meaning of uptake, determining the optimal injected activity, and investigating the dosimetry, is also required before its use as a renal cortical tracer can be supported.
CONCLUSION
In our first case, 68Ga-PSMA PET provided promising results in an adult with pyelonephritis. The results of our prospective study on a larger number of adult patients will provide a more accurate comparison of 68Ga-PSMA PET to 99mTc-DMSA scanning in pyelonephritis.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Sep. 4, 2020.
REFERENCES
- Received for publication May 4, 2020.
- Accepted for publication July 30, 2020.





{kind=link}
{kind=link}
{kind=link}