


Abstract
Paragangliomas associated with mutations of the SDHD gene can occasionally result in distant metastasis. Diagnosis can be difficult, and nuclear imaging is used to evaluate the case further. Not all tumors are alike; nuclear avidity may differ. We present a case in which metastatic paraganglioma caused by mutations of the SDHD gene was negative on 123I-metaiodobenzylguanidine scintigraphy and positive on 111In-labeled octreotide scintigraphy. This situation presents an opportunity for a novel therapeutic approach toward metastatic paraganglioma using targeted peptide receptor radionuclide therapy.
In the evaluation of patients with metastatic paraganglioma, nuclear imaging is useful for identifying metastatic sites and determining therapeutic options. 123I-metaiodobenzylguanidine (123I-MIBG) scintigraphy is the initial recommended nuclear imaging test, but its sensitivity in metastatic paraganglioma is only 56%–83% (1). If 123I-MIBG scintigraphy has negative results, additional nuclear imaging such as with 111In-octreotide scintigraphy and 68Ga-DOTATATE PET can be valuable, both of which have been shown to detect metastatic disease better than 123I-MIBG scintigraphy (2,3). Alternative imaging can also be done with 18F-FDG PET and 18F-FDOPA PET (1), as well as with 68Ga-DOTATATE PET, which was recently approved by the U.S. Food and Drug Administration for use in suspected metastatic neuroendocrine tumors. 111In-octreotide positivity indicates the presence of somatostatin receptor subtypes 2 and 5 and the potential effectiveness of therapy with octreotide. The emergence of peptide receptor radionuclide therapy (PRRT) offered a new treatment option for 111In-octreotide-avid metastatic paraganglioma. PRRT uses radiolabeled somatostatin analogs that specifically target somatostatin receptors on the tumor (4,5). The two β-emitting radionuclides used for radiolabeled therapy are 90Y and 177Lu (4,5). The response to 90Y has been reported to be between 4% and 33% (5). Complete and partial remission with 177Lu has been reported to be 2% and 28%, respectively (5). Quality of life is improved in up to 70% of cases, with minimal toxicity (4,5).
CASE REPORT
A 52-y-old woman with a known SDHD mutation was diagnosed and treated for bilateral dopamine-secreting cervical paragangliomas in 1996 and did well until 2013. She developed recurrent bilateral neck masses and was treated with repeated surgical excision of the left-side tumor and radiation therapy of the right-side tumor, given that the latter was unresectable (Fig. 1A). In 2014, she developed hypertension, flushing, and tachycardia. Biochemical evaluation revealed a serum dopamine level of 280 (reference level, <20 pg/mL). Neck imaging revealed stable lesions, but on chest CT she was found to have a ninth thoracic vertebral lesion (Fig. 2A). After α-blockade, she underwent vertebral biopsy, which revealed metastatic paraganglioma. She was treated with radiation therapy to the thoracic spine. Her dopamine levels remained elevated and she underwent 123I-MIBG imaging (Fig. 3A), with negative results. 111In-octreotide imaging, however, showed increased uptake in the right cervical tumor and the ninth thoracic vertebral body (Figs. 1–3).
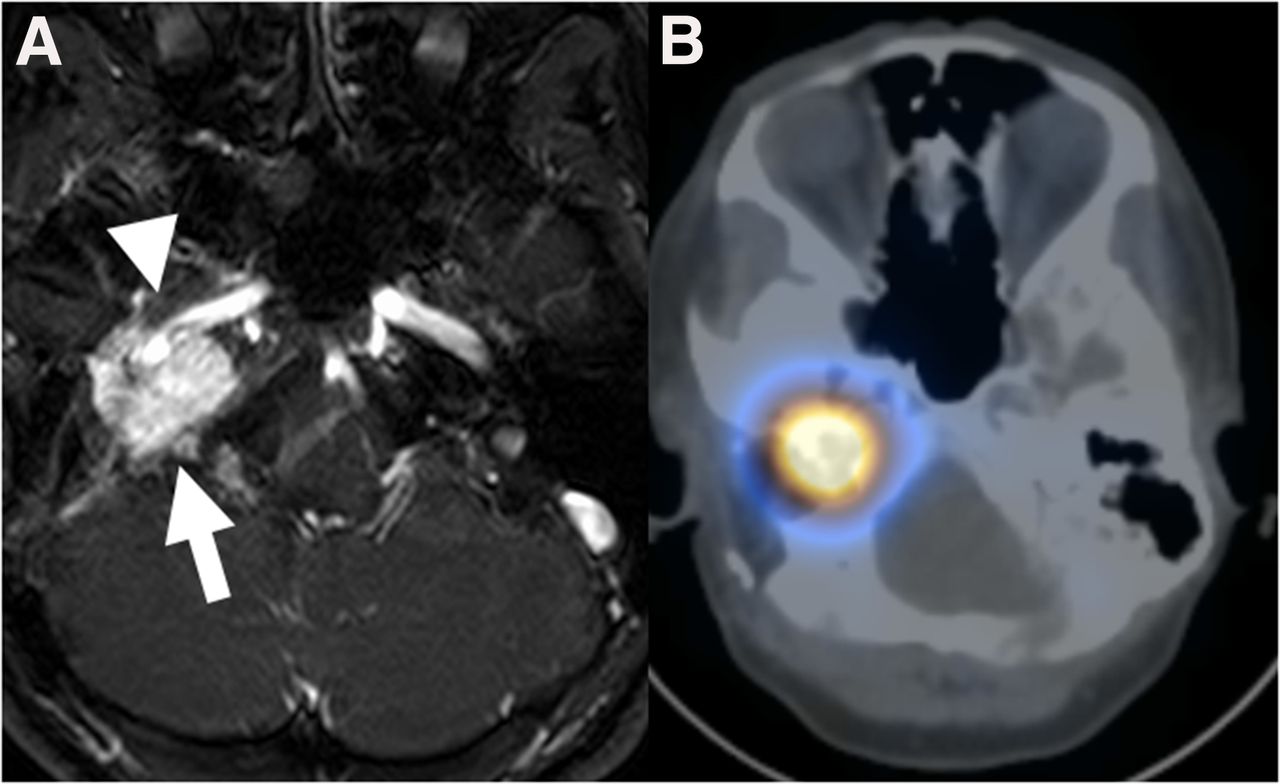
(A) Axial MR image of avidly enhancing recurrent nonresectable mass of right skull base at level of jugular bulb (arrow), partially encasing right internal carotid artery (arrowhead). (B) Corresponding axial SPECT/CT 111In-octreotide image showing intense avidity in mass.

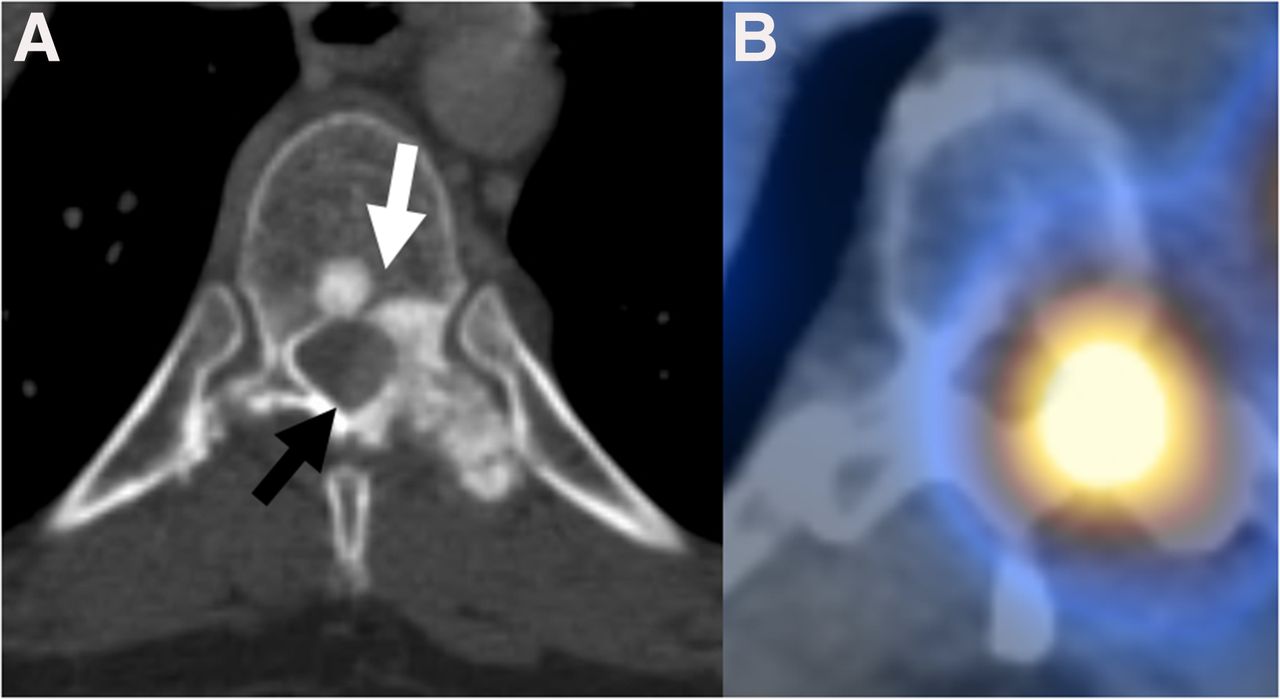
(A) CT scan of T9 vertebra showing predominantly sclerotic bone metastasis involving vertebral body, left pedicle, and left transverse process (white arrow) and solid enhancing epidural soft tissue (black arrow). (B) Corresponding axial SPECT/CT 111In-octreotide image showing intense avidity in bone metastasis.
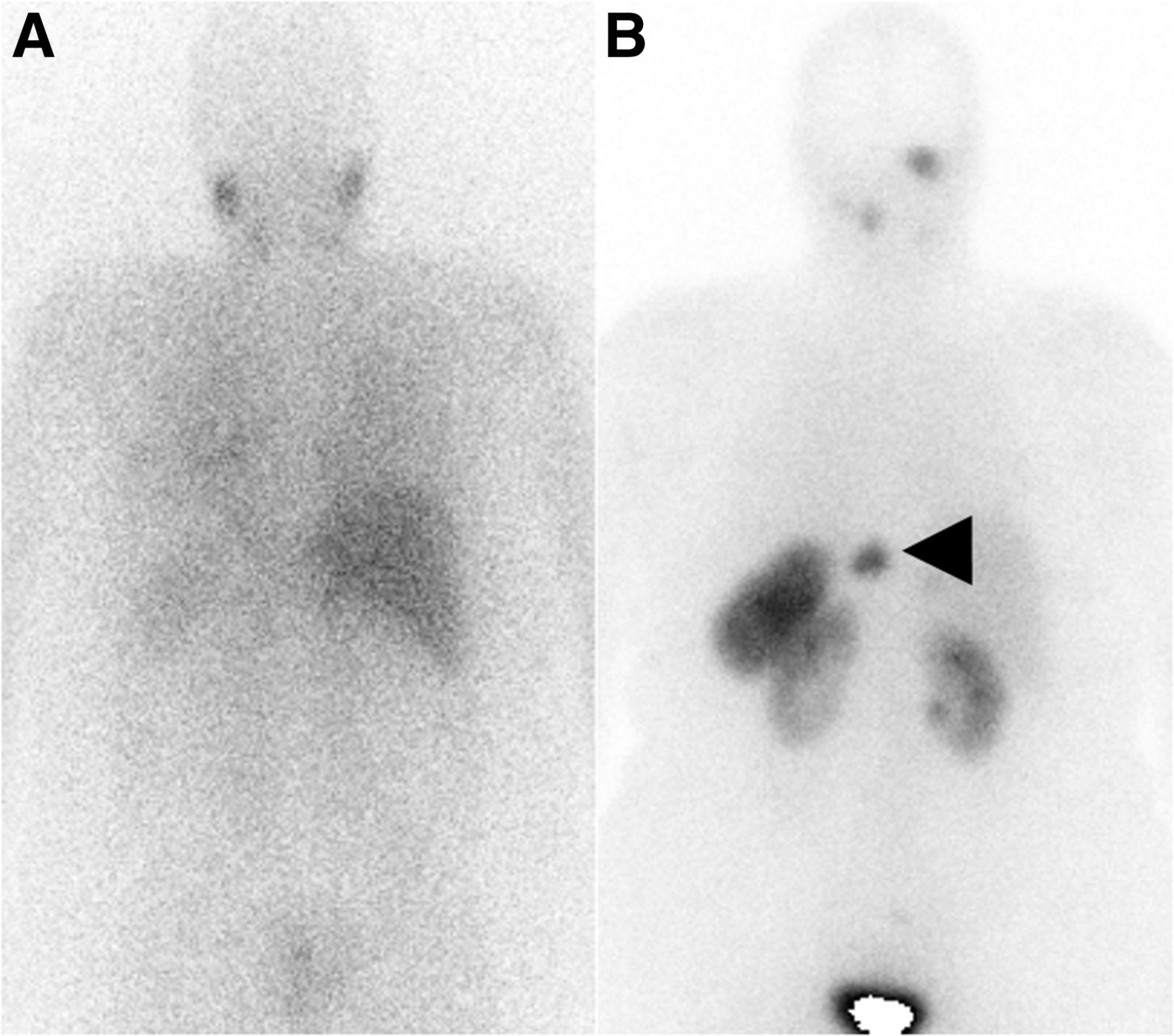
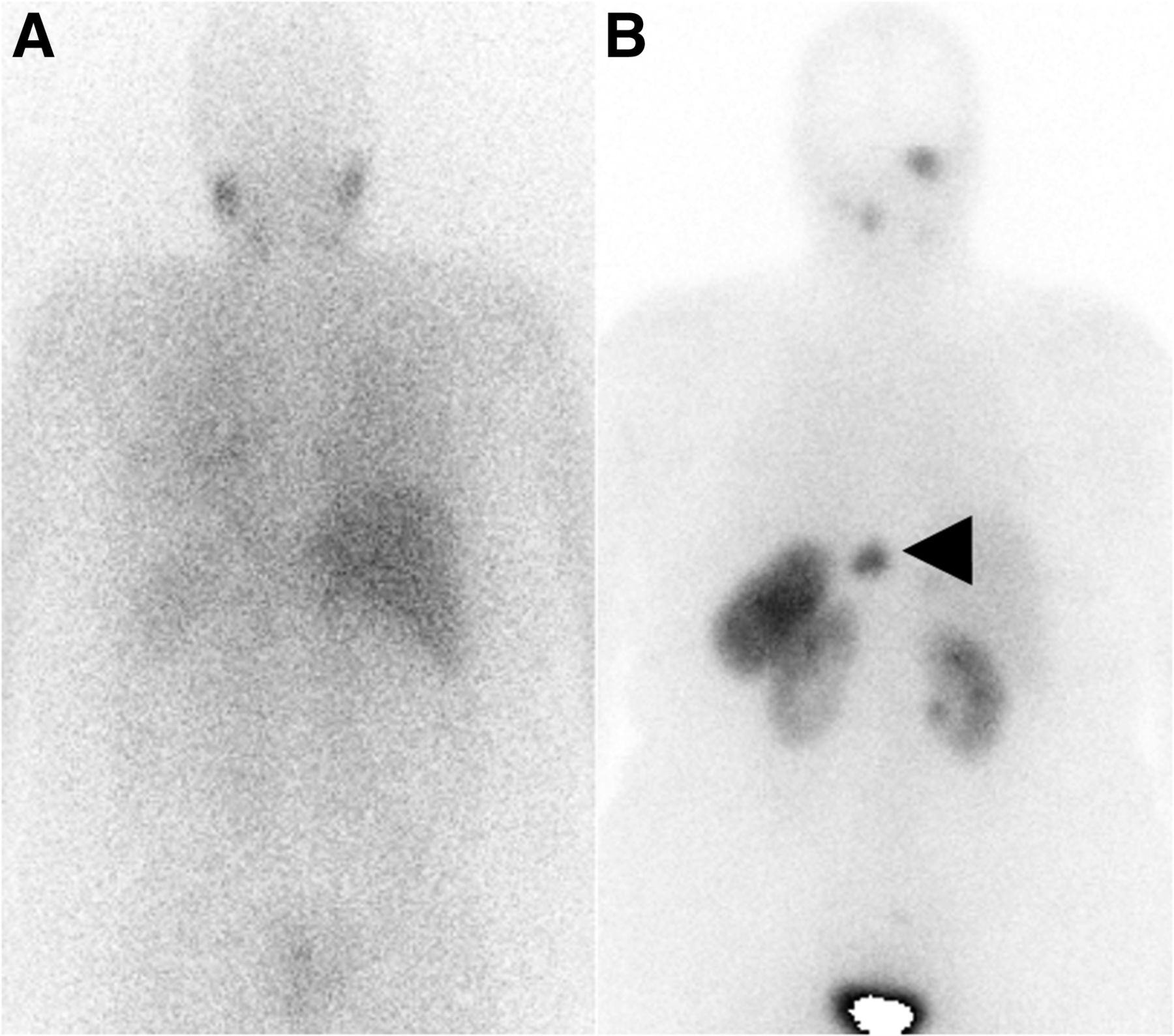
(A) Whole-body posterior 123I-MIBG γ-camera image showing normal uptake in salivary glands in neck and no uptake in known metastases. (B) Whole-body posterior 111In-octreotide γ-camera image showing focal intense uptake within disease sites in neck and in T9 metastasis (arrowhead).
DISCUSSION
This case highlights the importance of nuclear imaging in diagnosing metastatic paraganglioma. If initial 123I-MIBG scintigraphy studies are negative, then 111In-octreotide scintigraphy can potentially aid in localizing the metastatic paraganglioma and can also have therapeutic implications. Additional nuclear imaging such as with 18F-FDG PET, 18F-FDOPA PET, and 68Ga-DOTATATE PET can also be useful (1–3). In this case, it allowed us to treat the patient with 111In-octreotide subcutaneously and to refer her for a clinical trial of the use of PRRT.
CONCLUSION
Diagnosis of metastatic paraganglioma is difficult and may require more than one nuclear medicine imaging modality. Although 123I-MIBG scintigraphy is the initial test recommended to evaluate for metastatic paraganglioma, not all tumors are 123I-MIBG–positive, and alternate imaging such as with 111In-octreotide scintigraphy, 18F-FDG PET, 18F-FDOPA PET, and 68Ga-DOTATATE PET may be indicated. Receptor positivity can help dictate the radiolabeled therapy options.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Oct. 27, 2016.
REFERENCES
- Received for publication July 19, 2016.
- Accepted for publication September 19, 2016.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.