


Abstract
This report describes a case of extensive diffuse bone marrow involvement with bilateral breast metastases from duodenal neuroendocrine tumor giving rise to a superscan-like appearance on somatostatin receptor–targeted 99mTc-hydrazinonicotinamide-TOC scintigraphy. The metastatic lesions demonstrated partial concordance with 18F-FDG PET/CT findings, signifying varying tumor biology and heterogeneity among metastatic lesions in the same individual, as illustrated with a dual-tracer approach. There was a dramatic symptomatic and biochemical response and better health-related quality of life with a single fraction of peptide receptor radionuclide therapy with 177Lu-DOTATATE, and radiologically there was stable disease at that point.
We present an unusual case of atypical metastatic disease from gastroenteropancreatic neuroendocrine tumor (NET) in bone marrow and breast, diagnosed using 99mTc-hydrazinonicotinamide (HYNIC)-TOC scintigraphy. Varying biology and heterogeneity among metastatic lesions in the same individual was demonstrated by a dual-tracer approach. Substantial symptomatic improvement with better health-related quality of life was documented with a single fraction of peptide receptor radionuclide therapy (PRRT) with 177Lu-DOTA-octreotate.
CASE REPORT
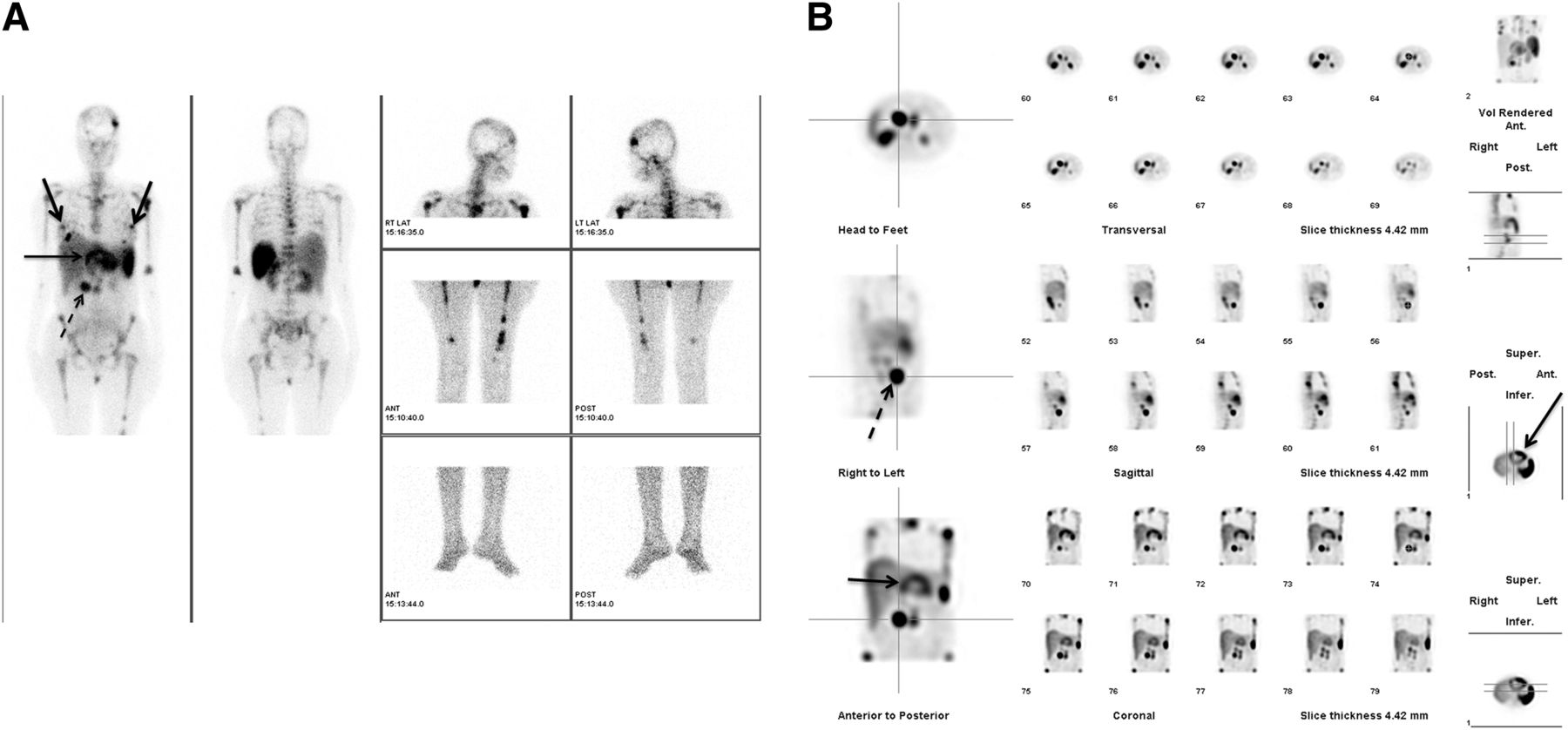
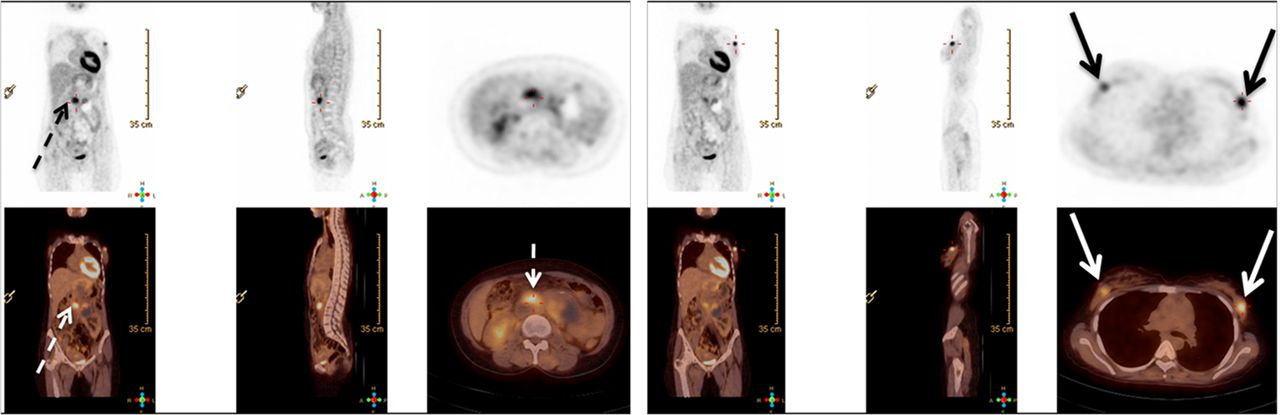
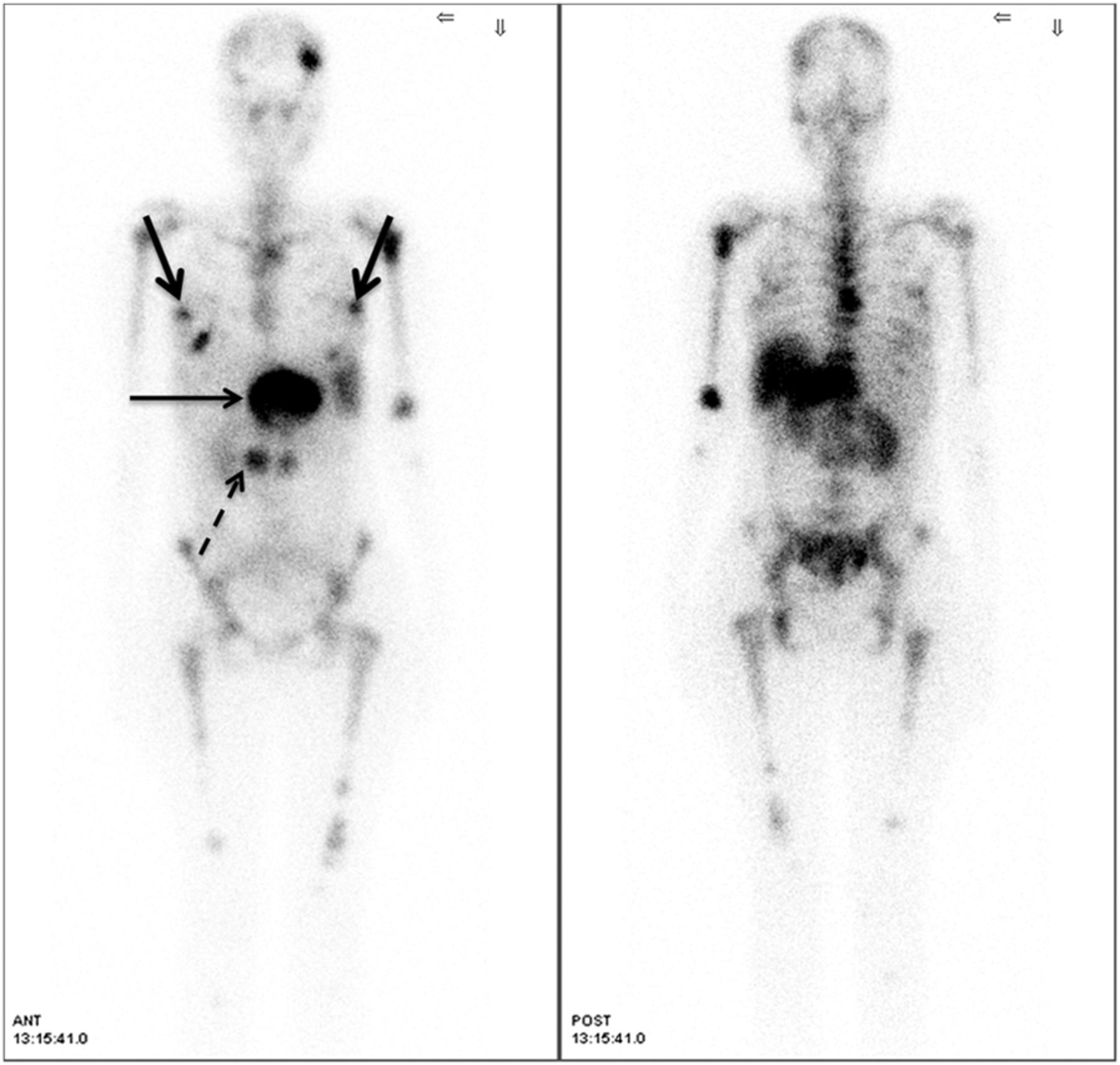
A 35-y-old woman diagnosed with duodenal NET (MiB-1 labeling index, 20%) with liver metastasis (involving the left lobe), and a history of radiofrequency ablation of the liver metastasis and external radiotherapy 6 mo previously, had progressively worsening symptoms of dyspnea on mild exertion, along with skeletal pain and weight loss. She was referred to determine her eligibility for PRRT. A 99mTc-HYNIC-TOC planar study (Fig. 1A) and SPECT study (Fig. 1B) demonstrated tracer uptake in the liver lesion, with a large area of photopenia (suggesting necrosis) at the residual primary in the duodenum. In addition, diffuse bone marrow involvement (over the axial and appendicular skeleton, with interspersed focal areas of uptake, particularly in the left parietal bone) and bilateral breast metastases were observed. Both had been unknown before scintigraphy. Comparative 18F-FDG PET/CT showed partial concordance, demonstrating relatively intense uptake in the duodenal primary tumor and bilateral metastatic breast nodules, with low-grade uptake in the liver lesion and absence of uptake in the bone marrow (Fig. 2). To summarize, the 99mTc-HYNIC-TOC study demonstrated the duodenal primary tumor and 4 metastatic lesions (liver, both breasts, and bone marrow); 18F-FDG PET was positive for the primary tumor, breast disease, and only low grade uptake in the liver; and previous CT was positive only for the liver lesion, with the other metastatic lesions being unknown previous to the functional imaging.
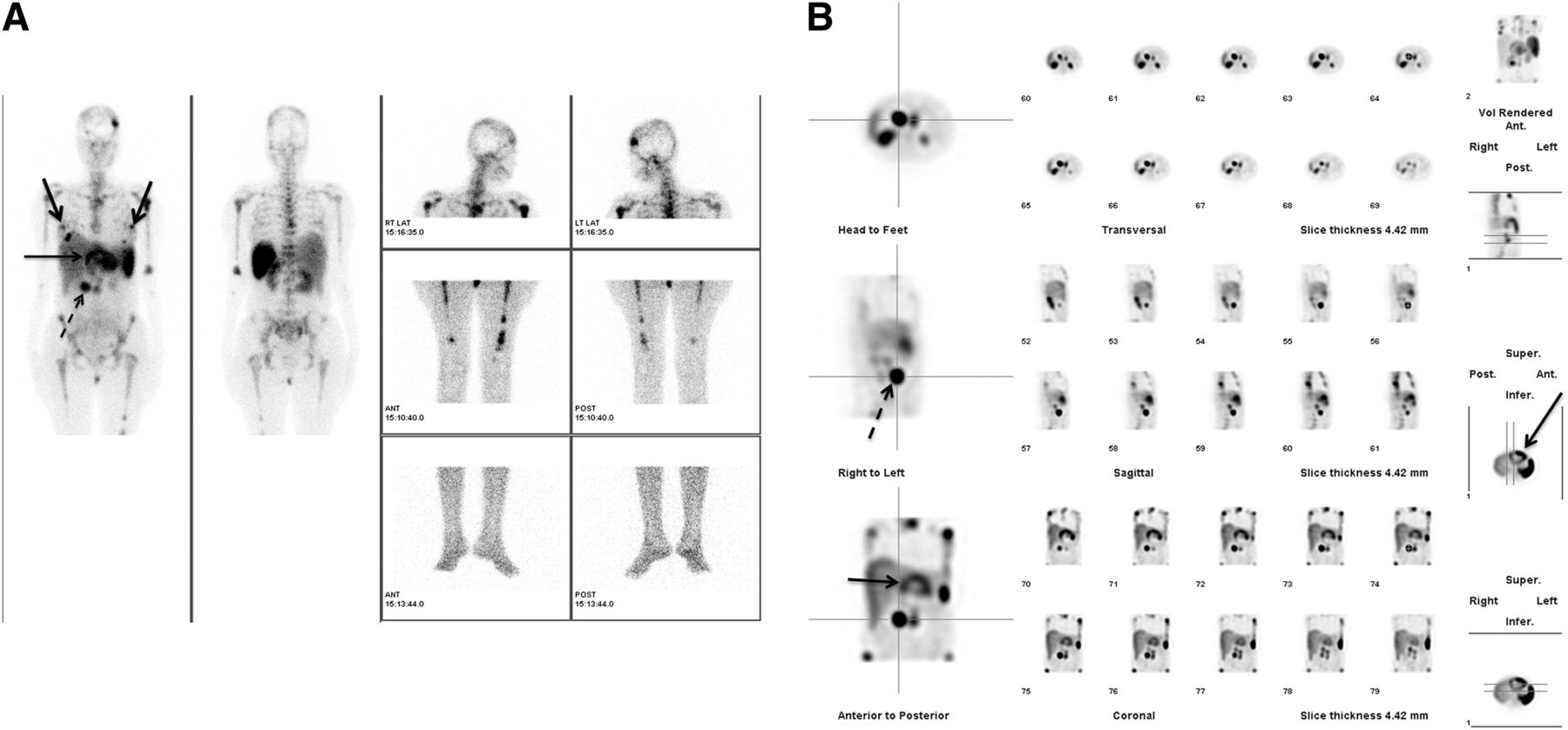
99mTc-HYNIC-TOC planar (A) and SPECT (B) images demonstrating tracer uptake in residual primary tumor in duodenum (dotted arrow) and liver lesion (thin solid arrow) with fairly large area of photopenia suggesting necrosis. Diffuse uptake over axial and appendicular skeleton (with interspersed areas of focal uptake, particularly in left parietal bone) and intense bilateral uptake in breast nodules (thick solid arrows) indicate metastases from NET.
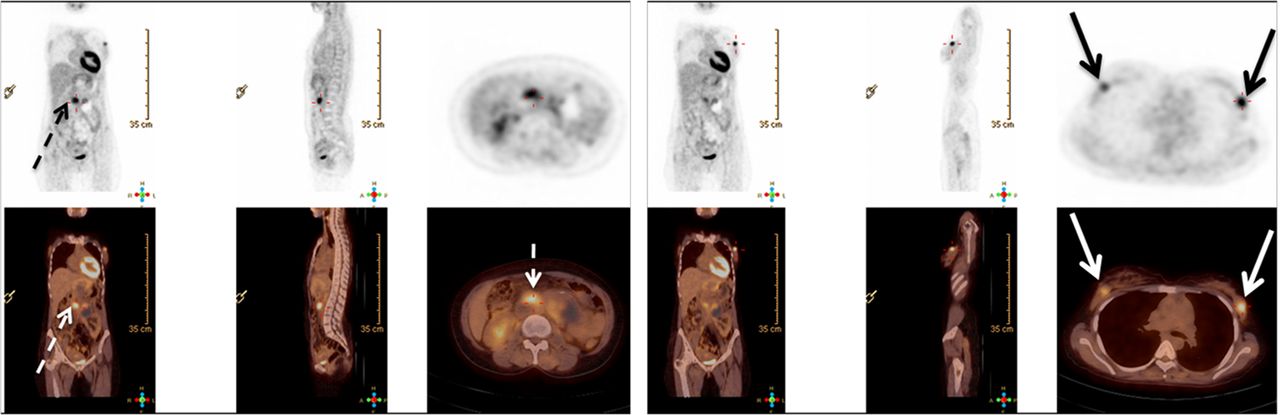
18F-FDG PET/CT demonstrating relatively intense uptake in duodenal primary tumor (dotted arrow), intense uptake bilaterally in metastatic breast nodules (solid arrows), low-grade 18F-FDG uptake in liver lesion, and no uptake in bone marrow.
The patient was treated with 7,104 MBq (192 mCi) of 177Lu-DOTATATE, and the posttherapy scan (Fig. 3) demonstrated an uptake pattern similar to that observed on the diagnostic 99mTc-HYNIC-TOC scintigraphy. At the 3-mo posttherapy assessment, symptoms were substantially improved, health-related quality of life was better, and disease was radiologically stable. The serum chromogranin A level decreased from 1,135 to 786.70 ng/mL; 99mTc-HYNIC-TOC scintigraphy demonstrated stable disease. The patient was prepared for a second cycle of PRRT.
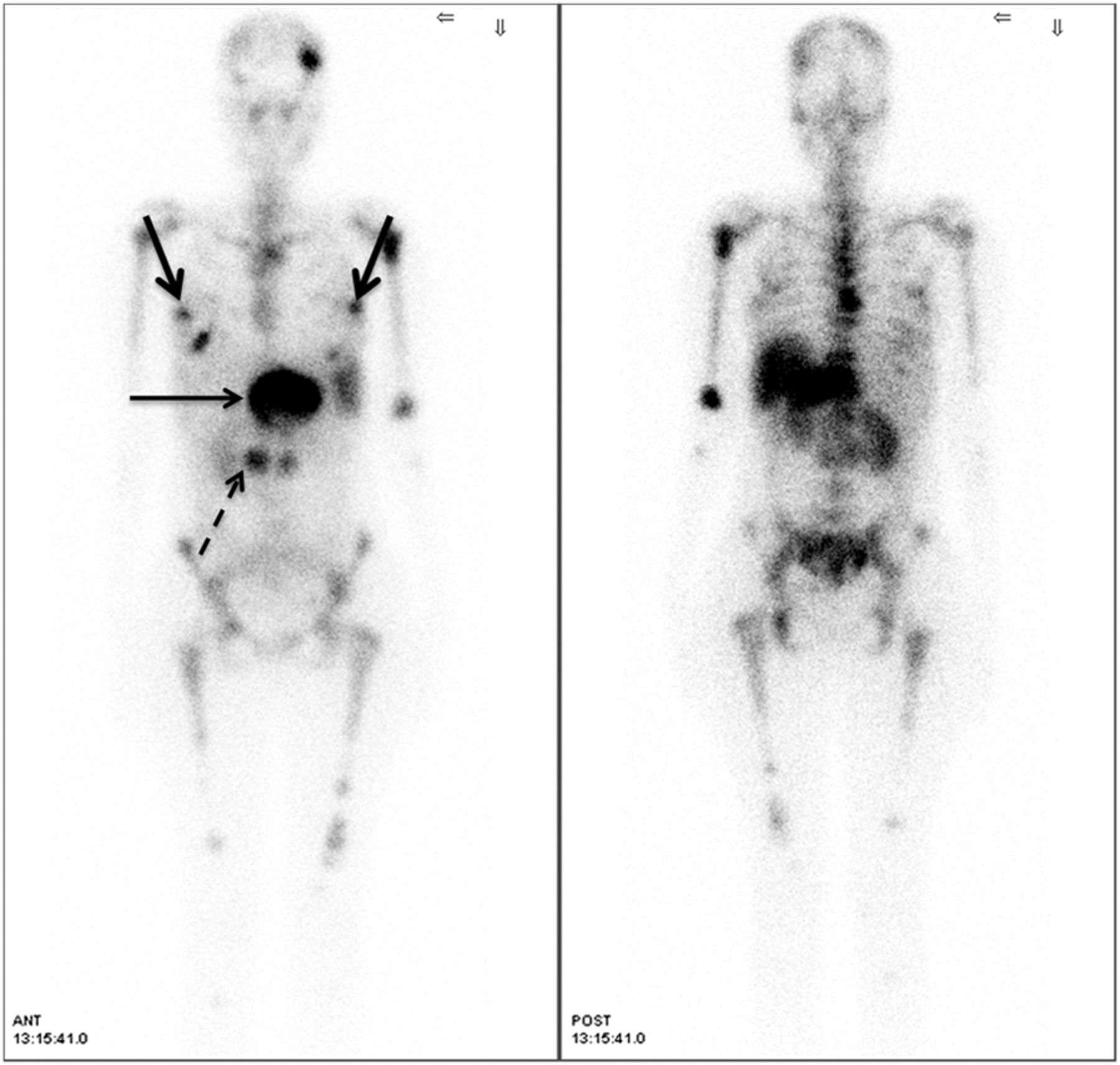
Scan after 177Lu-DOTATATE therapy showing uptake pattern similar to that on pretreatment diagnostic 99mTc-HYNIC-TOC scintigraphy.
DISCUSSION
In recent years, PRRT has evolved as an effective therapeutic option for metastatic NET. Somatostatin receptor–targeted imaging (with 99mTc-HYNIC-TOC, 111In-octreotide scintigraphy, or 68Ga-DOTANOC/TATE PET/CT) is integral for evaluating whether metastatic NET patients are eligible for PRRT. 18F-FDG PET/CT in NET can been regarded to be of more value for prognosis than for diagnostic staging (1–3) and can be positive, negative, or (interestingly) mixed positive/negative (as observed in this patient), thus depicting heterogeneity among different metastatic lesions in the same individual. The prognosis for NET with the dual-tracer approach is a subject of current research, and it is expected that the lesions with somatostatin receptor positivity and 18F-FDG negativity will demonstrate the most favorable behavior, followed by those that are both somatostatin receptor–positive and 18F-FDG–positive, whereas the least favorable prognosis will be for those who are somatostatin receptor–negative and 18F-FDG–positive. However, this expectation needs further validation in prospective trials. A dramatic symptomatic response is one of the gratifying experiences with PRRT in this setting.
CONCLUSION
An atypical metastatic pattern and differing tumor biology among the various lesions within the same individual was demonstrated in this report. Irrespective of the behavior, a dramatic symptomatic response and better quality of life were documented with PRRT with 177Lu-DOTA-octreotate.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Sep. 4, 2014.
- Received for publication February 18, 2014.
- Accepted for publication April 14, 2014.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.