


Abstract
18F-FDG is a well-established tracer for evaluating myocardial viability, as is 99mTc-tetrofosmin (TET) for evaluating myocardial perfusion. Dual-isotope single-acquisition (DISA) studies using a 99mTc perfusion agent and 18F-FDG have been performed to evaluate myocardial viability. The purpose of this investigation was to determine whether there is a difference in the results of gated SPECT DISA, compared with gated SPECT DIDA (dual-isotope dual-acquisition) studies using 99mTc-TET/18F-FDG and a high-energy collimated dual-head SPECT system.
Methods: We prospectively studied 13 patients with depressed left ventricular function using both acquisition protocols. Summed rest scores were calculated for both 99mTc and 18F-FDG studies using a 12-segment model and a 5-grade severity score. Images were evaluated by a single reader who did not know whether the images were acquired separately or simultaneously.
Results: The concordance of DISA and DIDA protocols for 99mTc-TET when allowing no difference in the SRS was 57%, or 89 of 156 segments. The concordance of DISA and DIDA protocols for 18F-FDG was 86%, or 134 of 156 segments. The concordance of segments determined to be viable versus nonviable was 92%, or 143 of 156 segments. Ejection fraction measurements obtained by gated 99mTc-TET studies correlated strongly with those obtained by gated 18F-FDG studies.
Conclusion: A high concordance for 18F-FDG studies was shown between gated DISA and gated DIDA. A lower concordance was shown between gated DISA and gated DIDA studies using 99mTc-TET, most likely because of downscatter from 18F into the 99mTc window. An excellent concordance was demonstrated between the 2 techniques for viability assessment. The gated 99mTc-TET/18F-FDG DISA protocol can be both a reliable and an efficient way to evaluate myocardial function, perfusion, and viability.
The most commonly used single-photon tracer for the evaluation of myocardial viability is 201Tl. However, several investigators have reported that SPECT using 18F-FDG, when compared with other commonly used tracers for determining myocardial viability, identifies additional viable tissue (1–3). These findings have made 18F-FDG the imaging gold standard for assessment of myocardial viability. The widespread use of 18F-FDG has been limited in the past by several factors but primarily by tracer availability and the high cost of dedicated PET scanners. Recent advances in technology have allowed the imaging of positron-emitting radionuclides, such as 18F, on scintillation cameras using ultra-high-energy parallel-hole collimators. For cardiac applications, the camera-collimator combination has acceptable spatial resolution and sensitivity for 99mTc and 18F single-acquisition SPECT imaging studies (4). The available data show that 18F-FDG SPECT provides comparable information to 18F-FDG PET concerning myocardial viability in patients with chronic coronary artery disease and depressed left ventricular function (5). For these viability studies, it is important to compare the 18F-FDG distribution to the distribution of myocardial perfusion. The ability to perform perfusion and viability imaging simultaneously would be economically and logistically attractive. As noted by Sandler et al. (6), several important technical issues may interfere with the widespread application of this technology. The purpose of this study was to compare dual-isotope single-acquisition (DISA) studies with dual-isotope dual-acquisition (DIDA) studies and to evaluate the potential advantages and disadvantages of each.
MATERIALS AND METHODS
We prospectively studied 13 consecutive patients with depressed left ventricular function (ejection fraction < 45%) who were referred for myocardial viability assessment. All patients signed a consent form before the study. For each patient, images were acquired using DISA and DIDA protocols.
First, resting 99mTc-tetrofosmin (TET) studies were performed with intravenous injection of 1,110 MBq of the tracer. Thirty minutes after the injection, gated SPECT images were obtained for 30 s per frame. Blood glucose levels were monitored. A baseline between 110 and 140 mg/dL was desired before the 18F-FDG administration. Depending on the patient’s blood glucose level, 1–5 units of regular human insulin injection, U.S. Pharmacopeia, were administered intravenously. If necessary, 25–50 g of oral glucose were administered orally before insulin administration. The 18F-FDG studies were performed with intravenous administration of 370–555 MBq of the tracer and an uptake period of 30–45 min. The 18F-FDG gated SPECT images were acquired at 40 s per frame, concluding the DIDA protocol. Immediately after the 18F-FDG acquisition, a final acquisition was performed at 40 s per frame. For this DISA protocol, both 99mTc-TET gated SPECT and 18F-FDG gated SPECT were acquired with a single acquisition and photopeaks set at both 140 and 511 keV using a 20% energy window. Images were acquired during a 90° rotation (3° per stop) using a 2-headed scintillation camera with ultra-high-energy parallel-hole collimators. The imaging heads were oriented at 90° and contained 16-mm (⅝ in.) NaI (thallium) crystals (Varicam; Elscint, Haifa, Israel). A matrix size of 64 × 64 × 8 was used. Images were gated for 8 frames per cardiac cycle with 100% beat acceptance. A Butterworth filter with a cutoff of 0.35 cycles per pixel and a power of 5.0 was applied to the 99mTc-TET data. A Metz filter with a cutoff of 0.36 and a power of 3 was applied to the 18F-FDG data. Images were reconstructed with filtered backprojection, and no attenuation correction was applied. After reconstruction, the short-axis images underwent preprocessing for quantification of gated left ventricular ejection fraction using software that had been previously validated (7).
A single reader who did not know whether the 99mTc-TET and 18F-FDG images had been acquired by a DISA or a DIDA protocol interpreted the studies. A summed rest score (SRS) was calculated using a 12-segment model, with 0 = normal, 1 = mildly abnormal, 2 = moderately abnormal, and 3 = severely abnormal for each segment. A total of 156 segments were analyzed for concordance between DISA and DIDA studies for the severity and extent of abnormalities and viability assessment.
RESULTS
The concordance of the DISA and DIDA protocols for 99mTc-TET studies, in terms of severity when allowing no difference in the SRS between the 2 acquisition protocols, was 57%, or 89 of 156 segments. This low concordance relates to the large number of segments graded more severely abnormal by the separate acquisition protocol versus the single-acquisition studies (Table 1). When allowing for a difference ≥ 1 in the SRS, the concordance was 76%, or 119 concordant segments of 156 segments. The concordance of DISA and DIDA protocols for 18F-FDG when allowing for no difference in the SRS was 86%, or 134 concordant segments of 156 segments. When allowing for a difference of 1 or >1 in the SRS, the concordance was 96%, or 149 of 156 segments (Table 2).
Comparison Between DISA and DIDA 99mTc Studies
Comparison Between DISA and DIDA 18F-FDG Studies
The concordance of segments determined to be viable was 92%, or 143 of 156 segments.
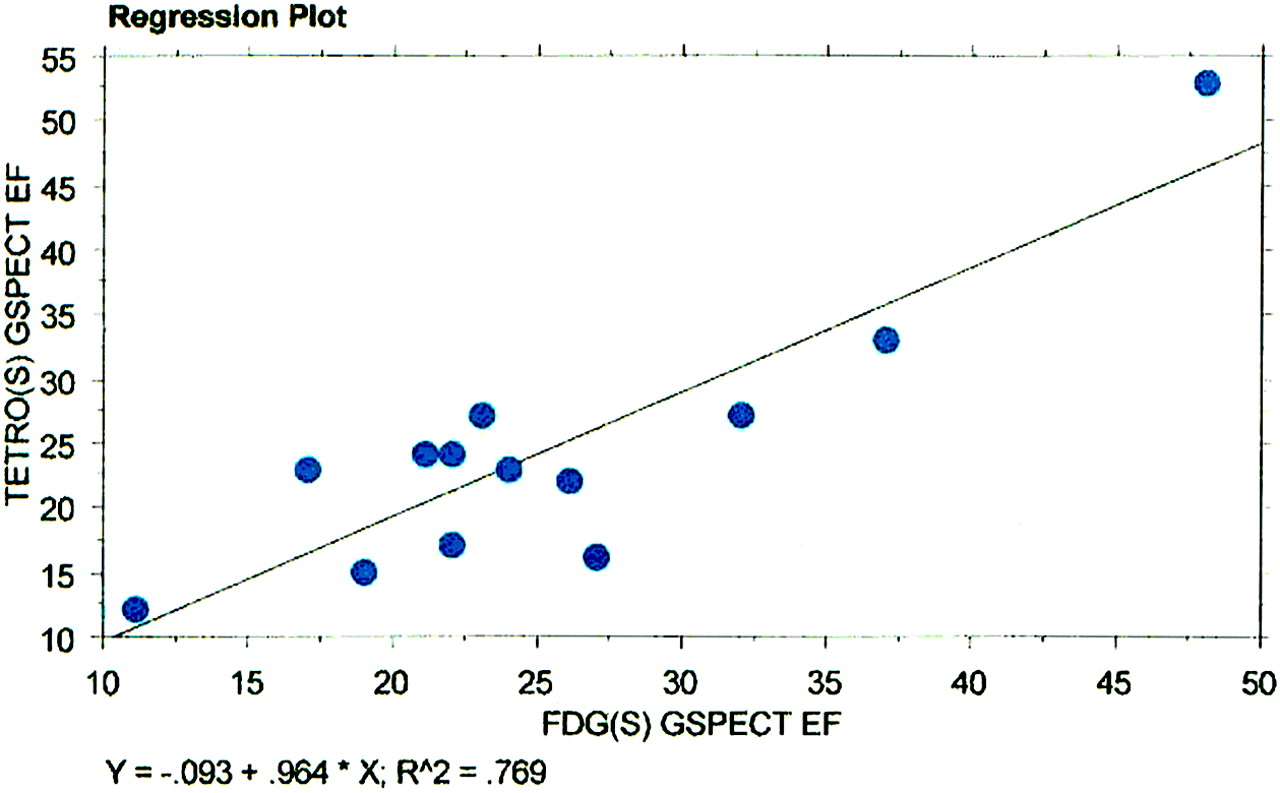
A linear regression analysis demonstrated a significant correlation between 99mTc-TET and 18F-FDG for left ventricular ejection fraction measurements by gated SPECT using the DISA protocol (r2 = 0.769) (Fig. 1). Likewise, there was a highly significant correlation between 99mTc-TET and 18F-FDG for left ventricular ejection fraction measurements by gated SPECT using the DIDA protocol (r2 = 0.738) (Fig. 2).

Linear regression plot demonstrates strong correlation between 99mTc-TET gated SPECT ejection fraction using single-acquisition protocol (TETRO[S] GSPECT EF) and 18F-FDG gated SPECT ejection fraction using single-acquisition protocol (FDG[S] GSPECT EF).
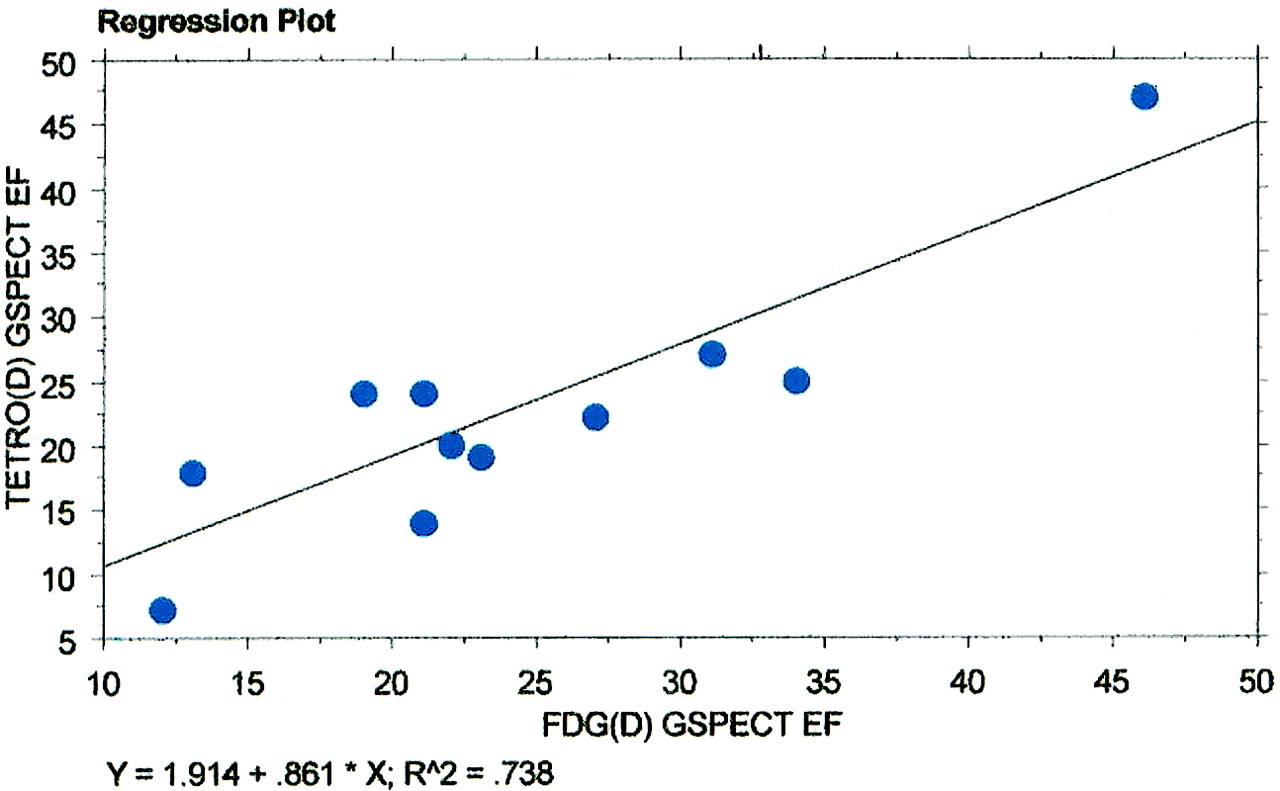
Linear regression plot demonstrates strong correlation between 99mTc-TET gated SPECT ejection fraction using dual-acquisition protocol (TETRO[D] GSPECT EF) and 18F-FDG gated SPECT ejection fraction using dual-acquisition protocol (FDG[D] GSPECT EF).
DISCUSSION
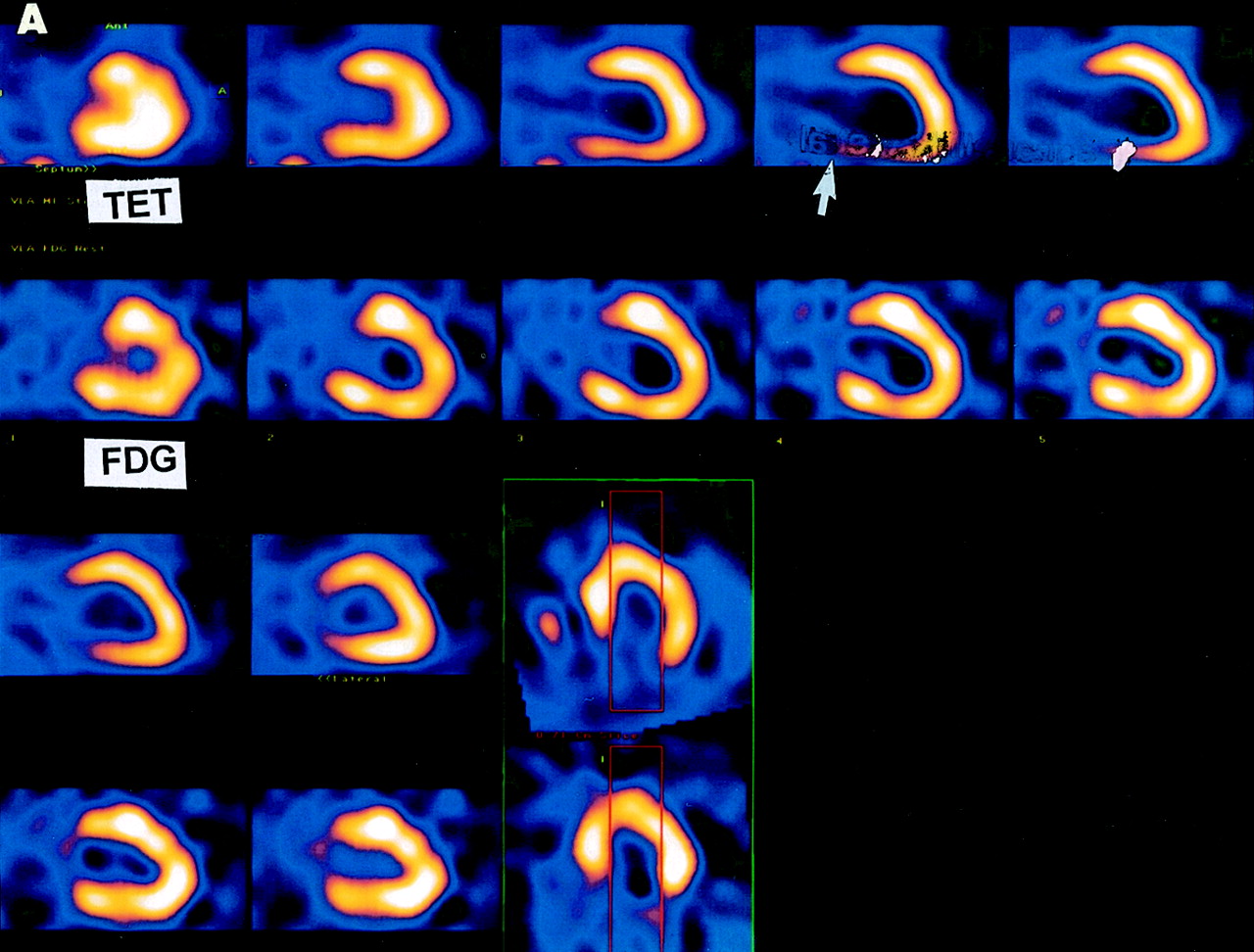
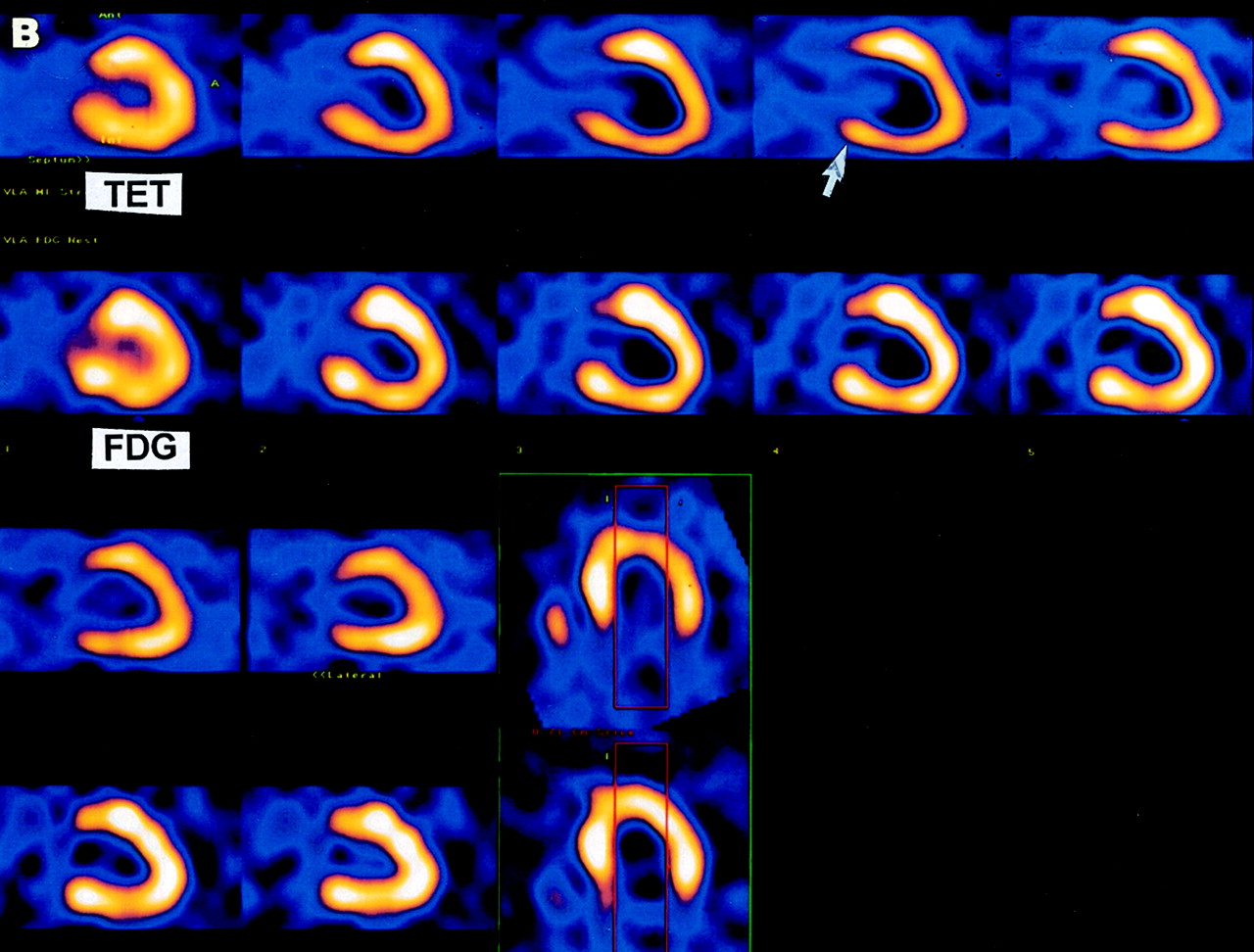
SRS for the 18F-FDG images was similar for the DISA and DIDA protocols. An overall good clinical concordance was shown between gated DISA and gated DIDA studies using 18F-FDG. No significant difference was found between gated 99mTc-TET and 18F-FDG measurements of left ventricular ejection fraction using either imaging protocol. The acceptable, although lower, concordance between the 99mTc-TET DISA and 99mTc-TET DIDA severity segment scores is believed to be a result of downscatter from the 18F annihilation radiation into the 99mTc energy window. Downscatter into the 99mTc window results in a “filling in” of defects in 99mTc-TET images, making the defects appear less severe (Figs. 3A and 3B). Other studies have acknowledged this potential problem and attempted to correct the 99mTc perfusion images for scatter, with limited success (8).


Vertical long-axis slices from 99mTc-TET (first row) and 18F-FDG (second row) studies of same patient using dual-acquisition protocol (A) and single-acquisition protocol (B). Inferior wall perfusion defect (arrow) but viable myocardium is seen on dual-acquisition 18F-FDG study, but perfusion abnormalities (arrow) are underestimated on single-acquisition 99mTc-TET study, likely related to downscatter from 18F 511-keV photons.
CONCLUSION
The SRS of the 99mTc-TET segments acquired with DISA were lower than the SRS of the segments acquired with DIDA. Despite a strong clinical correlation between the 18F-FDG DISA and 18F-FDG DIDA studies, a limited clinical concordance exists between 99mTc-TET DIDA and 99mTc-TET DISA studies. Therefore, our study strongly suggests that using a separate acquisition protocol will likely avoid underestimating perfusion defects that would be important in determining the ischemic-versus-nonischemic nature of a cardiomyopathic process. Such an underestimation would have a tremendous impact on how these patients would be treated clinically (medically vs. surgically).
Footnotes
For correspondence or reprints contact: Salvador Borges-Neto, MD, Duke University Medical Center, Durham, NC 27710.
E-mail: borge001@mc.duke.edu.





{kind=link}
{kind=link}
{kind=link}
{kind=link}