


Abstract
We present serial 18F-FDG PET/CT findings in a case of grade 3 pulmonary lymphomatoid granulomatosis positive for the Epstein–Barr virus. The patient experienced a transient complete response to R-CHOP chemotherapy and subsequent multisystem recurrence, predominately involving the subcutaneous region of the torso on 18F-FDG PET/CT. Biopsy of the most hypermetabolic subcutaneous lesion demonstrated grade 1 cutaneous lymphomatoid granulomatosis negative for the Epstein–Barr virus. This report highlights the role of 18F-FDG PET/CT in characterizing and monitoring disease progression and regression, as well as the limitations of 18F-FDG PET/CT in accurate grading of multisystem recurrence, given the diversity of clinical and histopathologic features of lymphomatoid granulomatosis.
Lymphomatoid granulomatosis is a rare T-cell rich, Epstein–Barr virus associated B-cell lymphoproliferative disorder, predominately involving the lung (1). Accurate grading information on this abnormality is essential in determining clinical management and prognosis. 18F-FDG PET/CT plays an important role in staging lymphomatoid granulomatosis, in monitoring therapeutic response, and in guiding biopsy (2).
CASE REPORT
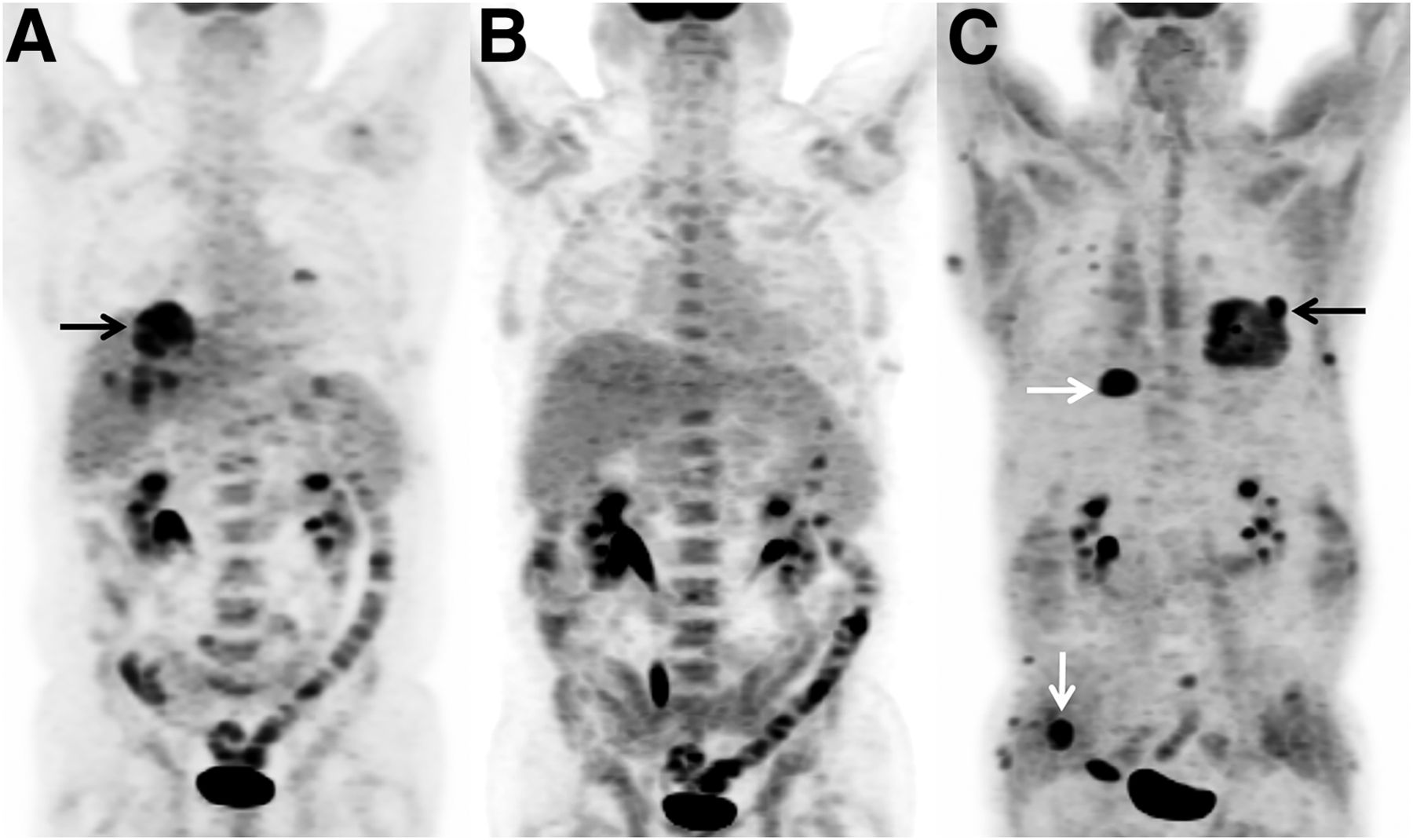
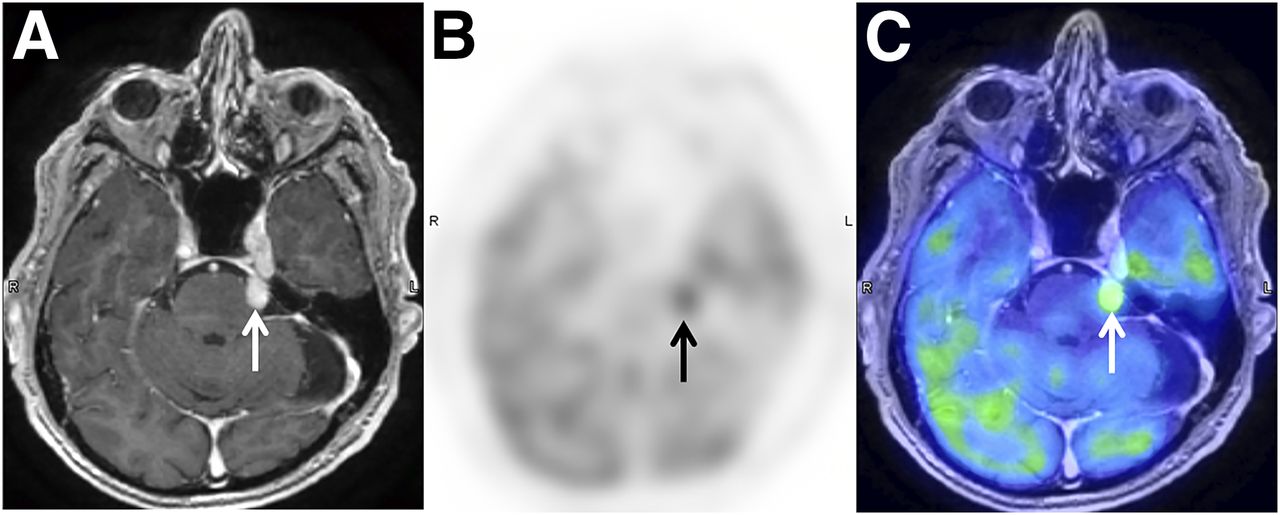
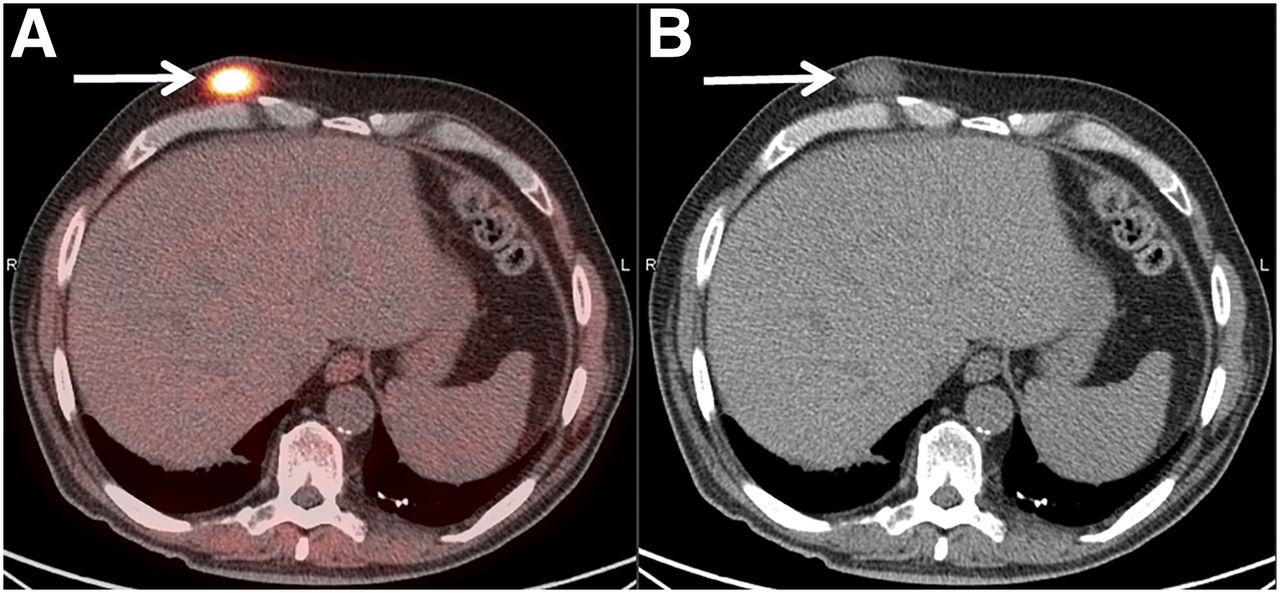
A 65-year-old man presented with multiple pulmonary nodules and underwent left lower lobe wedge resection. Histopathologic examination confirmed lymphomatoid granulomatosis of grade 3 on the World Health Organization classification, with atypical large B cells positive for Epstein–Barr virus. A staging 18F-FDG PET/CT scan showed multiple hypermetabolic nodules in both lungs (Fig. 1A). The patient received 6 cycles of rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) chemotherapy. Posttherapeutic 18F-FDG PET/CT showed resolution of all lung lesions, indicating a complete response to therapy (Fig. 1B). Seven months later, the patient presented with left ear pain and multiple subcutaneous nodules. A restaging 18F-FDG PET/CT scan demonstrated numerous hypermetabolic subcutaneous nodules in the torso and a hypermetabolic nodule in the left lung (Fig. 1C). Brain MRI showed an enhancing left-trigeminal-nerve lesion, which was also 18F-FDG avid (Figs. 2A–2C) and was presumed to represent involvement of the lymphomatoid granulomatosis in the central nervous system. Excisional biopsy of the most 18F-FDG avid subcutaneous nodule in the right anterior chest (Figs. 3A and 3B) demonstrated grade 1 lymphomatoid granulomatosis negative for the Epstein–Barr virus. The patient declined lung biopsy and additional chemotherapy. Palliative radiation therapy was delivered for symptomatic trigeminal neuralgia.

(A) Staging 18F-FDG PET/CT showed multiple hypermetabolic lung lesions (arrow). (B) After 6 cycles of R-CHOP therapy, all lesions resolved. (C) Seven months later, restaging 18F-FDG PET/CT showed multiple subcutaneous hypermetabolic lesions (white arrows) and a left lung hypermetabolic nodule (black arrow).

Contrast-enhanced brain MRI showed enhancing lesion (arrows) involving left trigeminal nerve (A), which was 18F-FDG avid (SUVmax, 6.3) on restaging 18F-FDG PET (B) and PET/MRI (C).

Restaging 18F-FDG PET/CT showed 18F-FDG avid subcutaneous nodule (arrows) with SUVmax of 10.3 on right anterior chest wall. Excisional biopsy confirmed grade 1 cutaneous lymphomatoid granulomatosis.
DISCUSSION
Lymphomatoid granulomatosis predominantly affects the lungs (>90%), followed by the skin (25%–50%), the kidneys (32%–40%), and the central nervous system (20%–30%) (1). The clinical behavior of lymphomatoid granulomatosis is highly variable, with approximately 12% of cases progressing to malignant lymphoma. Chemotherapy regimens for diffuse large B-cell lymphoma, such as R-CHOP, have shown promise for high-mortality grade 3 pulmonary lymphomatoid granulomatosis (3).
Histopathologic diagnosis of lymphomatoid granulomatosis relies on the cytologic atypia and density of clonal B cells positive for Epstein–Barr virus from the lung specimen (1). Of the few reported cases of concomitant pulmonary–cutaneous lymphomatoid granulomatosis, up to half showed absence of the Epstein–Barr virus, indicating discordant grading between the skin lesions and the lung lesions (4,5). In the current case, therefore, grading based on histopathologic examination of the cutaneous specimen was not reliable in predicting the clinical course or in guiding management.
CONCLUSION
18F-FDG PET/CT is a useful imaging tool in the surveillance of lymphomatoid granulomatosis but lacks accuracy in grading lymphomatoid granulomatosis, given the variability of Epstein–Barr virus positivity and the diversity of clinical features in cutaneous lesions. Histopathologic examination of lung lesion specimens is the reliable grading method in relapsed multisystem lymphomatoid granulomatosis.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jun. 8, 2018.
REFERENCES
- Received for publication April 2, 2018.
- Accepted for publication May 31, 2018.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.