


Abstract
18F-FDG uptake in enlarged lymph nodes is always suspicious, especially in cancer patients. We report a case of hypermetabolic internal mammary lymphadenopathy in a breast cancer patient who was previously treated with bilateral mastectomy and implants. The abnormal nodal uptake turned out to be due to foreign body–induced inflammation, as confirmed histopathologically. Vigilant PET interpretation is required in breast cancer patients who have evidence of breast implant rupture.
Breast cancer patients are often followed up with 18F-FDG PET/CT to detect local recurrence and metastasis. Any focus of abnormally increased radiotracer uptake should not be overlooked, because the activity may be due to malignancy instead of to benign conditions that cause high cellular metabolism. Silicone-induced lymphadenopathy is an uncommon late complication after breast implant surgery.
CASE REPORT
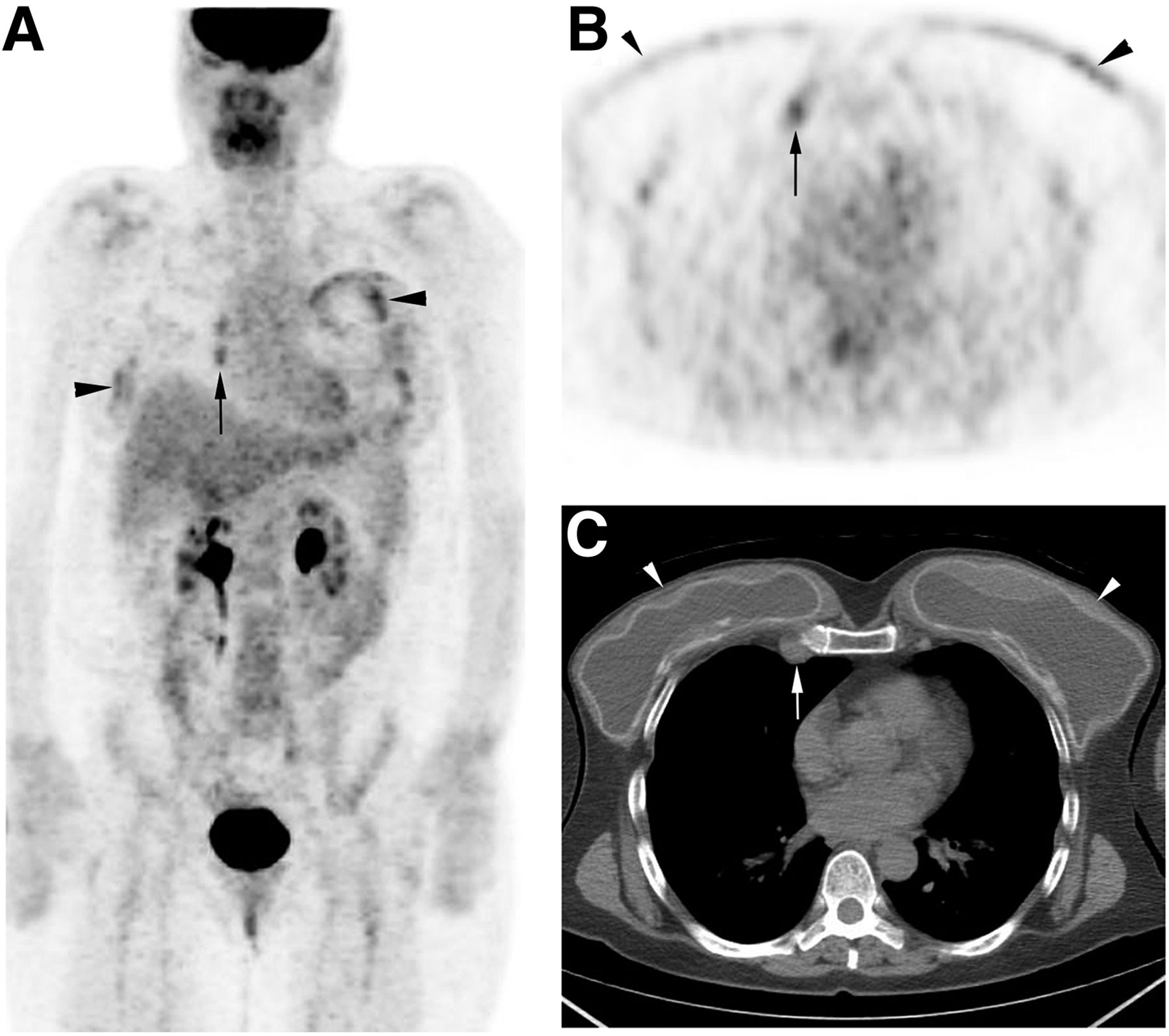
A 54-y-old woman presented to our hospital with bilateral pain in the chest wall deep to her breast implants. She had undergone bilateral mastectomy with reconstruction 14 y previously. Right mastectomy was done as definitive treatment for ductal carcinoma in situ, and the left mastectomy was prophylactic. She was referred for whole-body PET/CT to rule out tumor recurrence and help reach a more conclusive diagnosis. The PET scan showed nonspecific multifocal moderate hypermetabolic activity around the breast implants, more prominent on the left (Figs. 1A and 1B), possibly representing inflammatory changes. A bilaterally wavelike contour of the breast implants (Fig. 1C) suggested implant rupture. Moderate hypermetabolic activity was noted (Figs. 1A and 1B) in enlarged right internal mammary lymph nodes (Fig. 1C). No abnormal findings were noted elsewhere. Breast MRI confirmed bilateral breast implant rupture and right internal mammary lymphadenopathy (not shown). The suggestive node was excised. Histopathologic examination showed that the lymph node had a foreign-body giant-cell response.
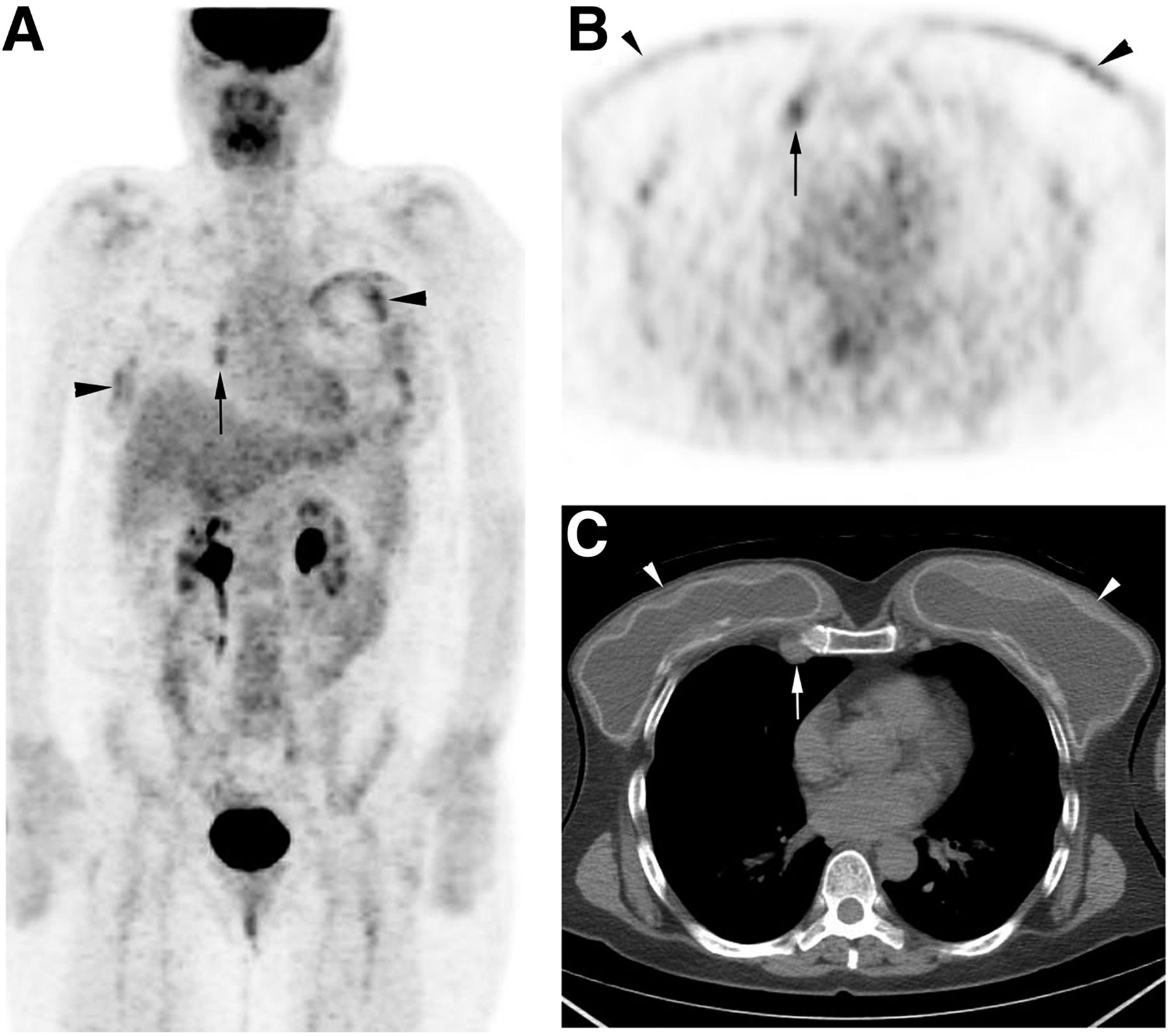
(A and B) Maximum-intensity projection (A) and axial (B) 18F-FDG PET images show patchy activity around breast implants, on left more than on right (arrowheads), and hypermetabolic right internal mammary nodes (arrows). (C) Axial unenhanced CT component of PET/CT image at level of breasts shows bilateral wavy contour of breast implants (arrowheads), suggesting rupture, and enlarged right internal mammary node (arrow).
DISCUSSION
Breast implant rupture is categorized as intracapsular or extracapsular. Intracapsular rupture is often unnoticed clinically because the free silicone is kept in place by a surrounding fibrous capsule. Extracapsular rupture is often associated with silicone migration (1). Leaked silicone can either remain within the breast or migrate to axillary and sometimes internal mammary nodes and even distal nodal and extranodal sites (2). The differential diagnosis on PET includes cancer recurrence, de novo malignancy, metastasis, and silicone granuloma.
Physical examination is less sensitive to the detection of silicone breast implant rupture, especially when there is no capsular contracture. Dedicated breast MRI is the imaging modality used to detect and evaluate a clinically unnoticed rupture (3). Unfortunately, some women cannot undergo MRI because of contraindications such as having a cardiac pacemaker, another device, or claustrophobia. PET imaging can show increased 18F-FDG uptake in regions of silicone-induced inflammation (4). Histopathologic examination is crucial for a definitive diagnosis (5). Removal of the ruptured implant should be considered to prevent further complications from silicone-gel migration.
CONCLUSION
18F-FDG uptake in nodal or even extranodal sites is nonspecific in patients with a history of breast cancer and breast implant rupture. Any uptake should be interpreted with caution as it may represent a malignancy and not a benign finding such as granulomatous inflammation. Once foci of increased 18F-FDG uptake are found, correlation with histopathologic findings is critical before treatment.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Aug. 3, 2018.
- Received for publication April 8, 2018.
- Accepted for publication May 7, 2018.





{kind=link}