


Article Figures & Data
Figures
- FIGURE 1.
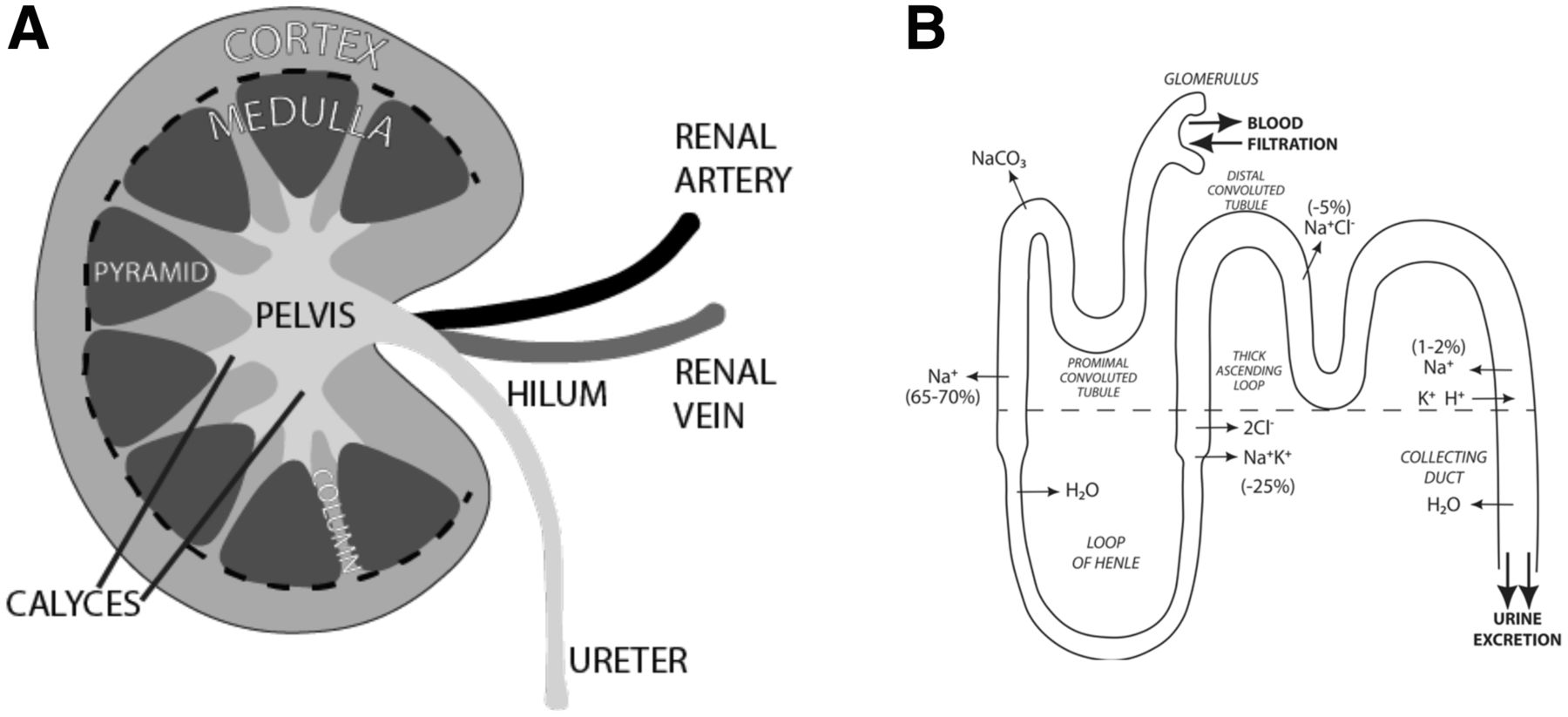
Kidney anatomy and glomerulus function. (A) Kidney is bean-shaped paired organ. Indentation is called hilum and is where renal artery enters, whereas renal vein and ureter exit. Parenchyma comprises outer cortex and inner medulla, with medulla further subdivided into pyramids and columns. This all surrounds CS, which is made up of multiple calyces feeding into pelvis. (B) Blood enters glomerulus containing waste and then leaves filtered. Nephron travels into and out of cortex (separated by dashed line), whereas electrolytes are exchanged and urine concentrated before being excreted into calyces.
- FIGURE 2.
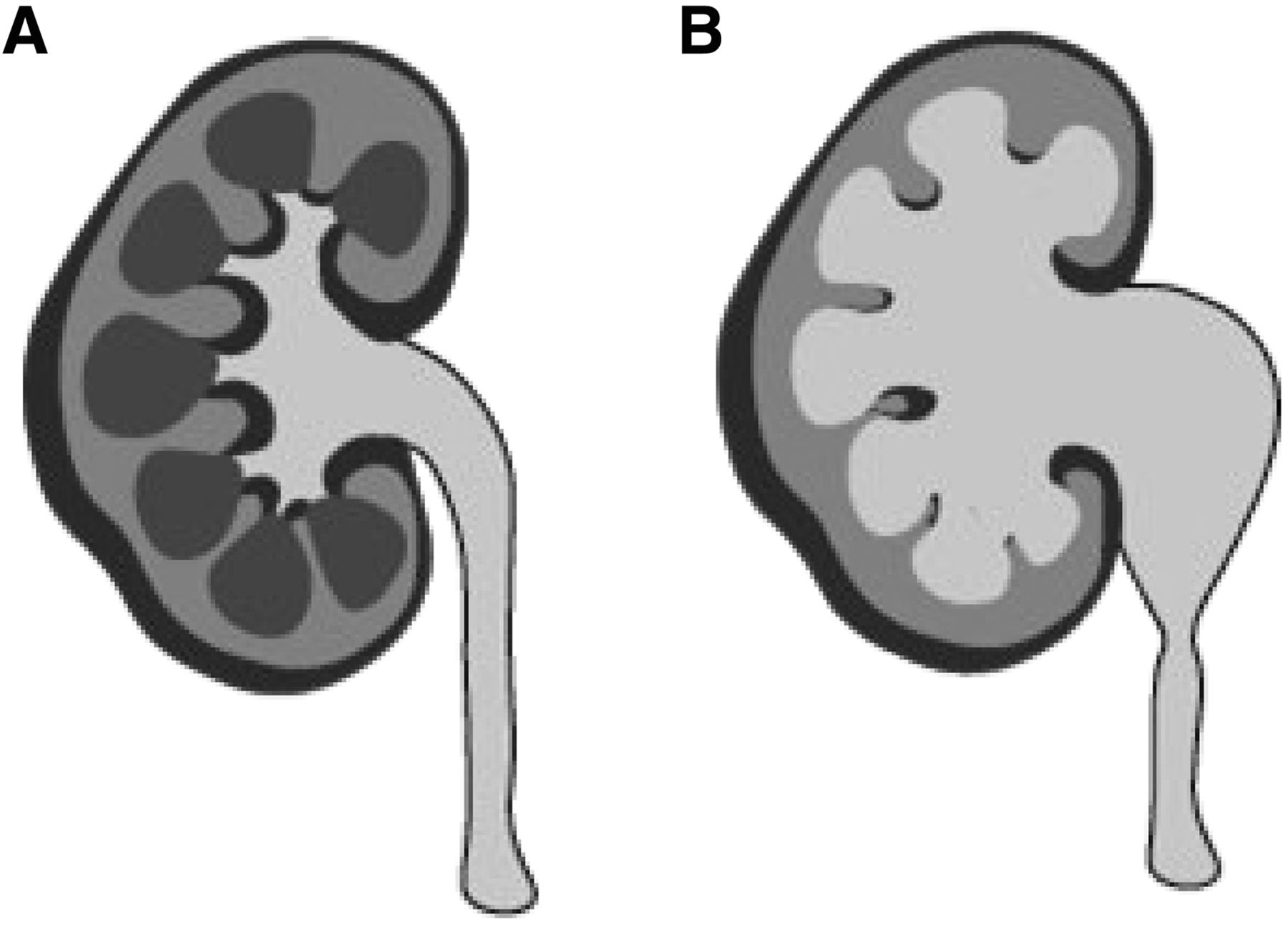
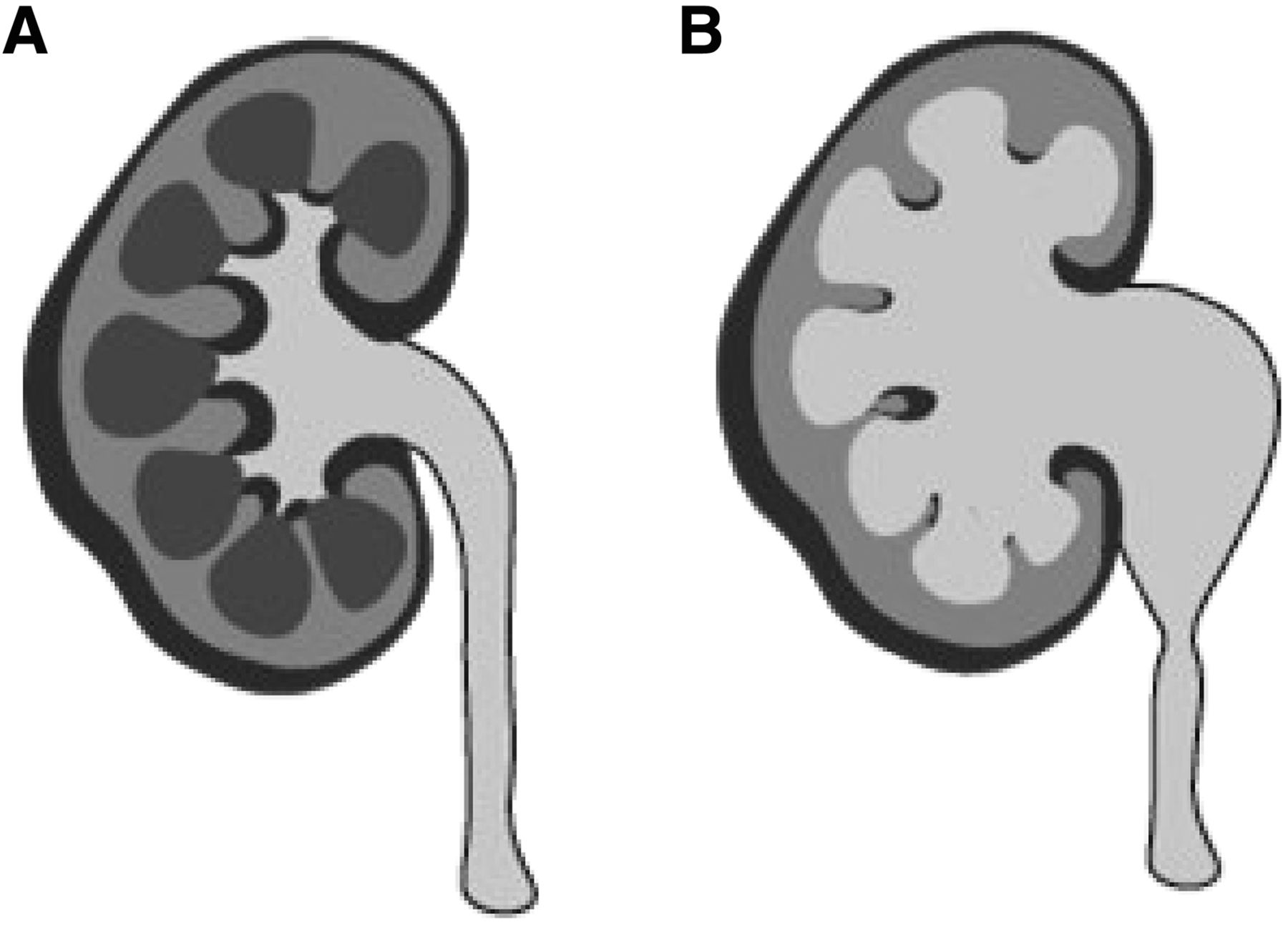
(A) Normal kidney demonstrates small calyces and decompressed renal pelvis. (B) With obstruction (and other disorders), calyces and pelvis become dilated.
- FIGURE 3.
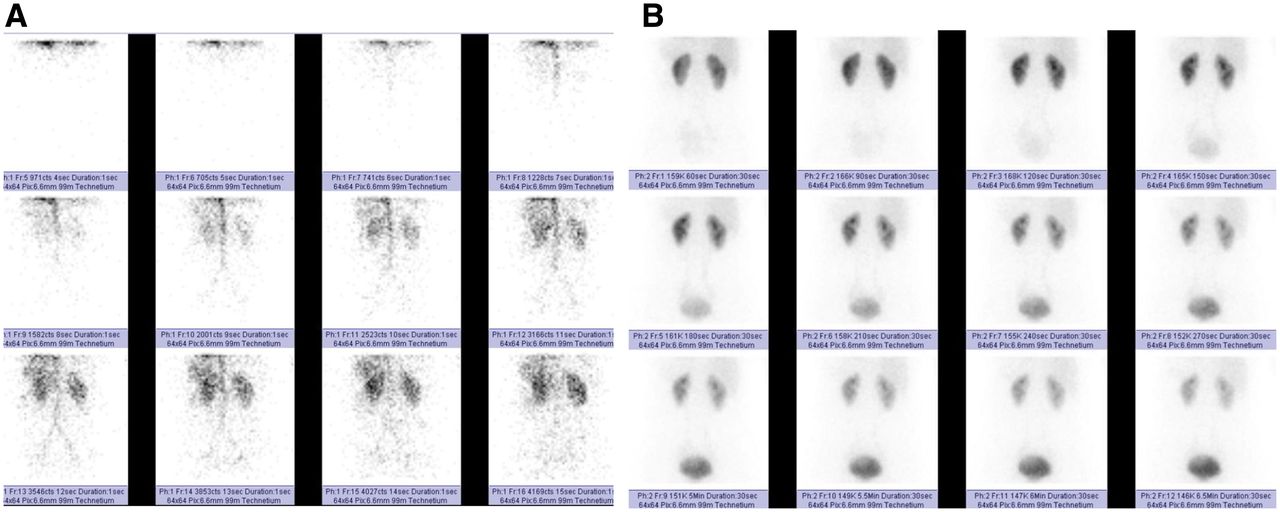
(A) First-minute blood flow phase with frames acquired every second (first 12 s displayed). (B) Dynamic phase with frames acquired every 30 s (minutes 2–7 displayed). Phase is helpful for assessing both parenchymal function and urine drainage.
- FIGURE 4.
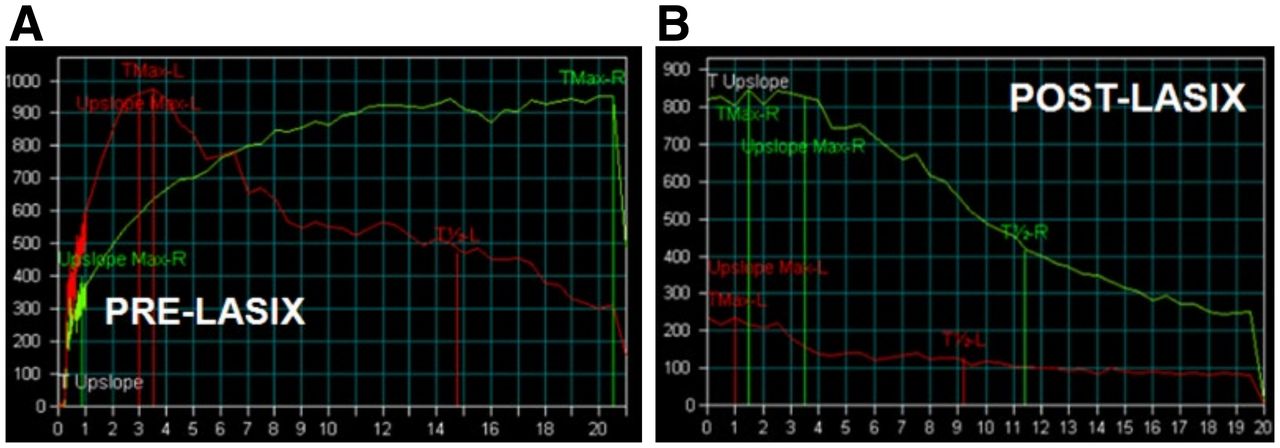
Dual-phase acquisition. (A) First 20 min of findings for right kidney are concerning for obstruction, necessitating diuretic administration. (B) Postdiuretic T-½ of slightly less than 10 min excludes obstruction. Green curve = right kidney; red curve = left kidney; Lasix (Aventis Pharma) = furosemide.
- FIGURE 5.
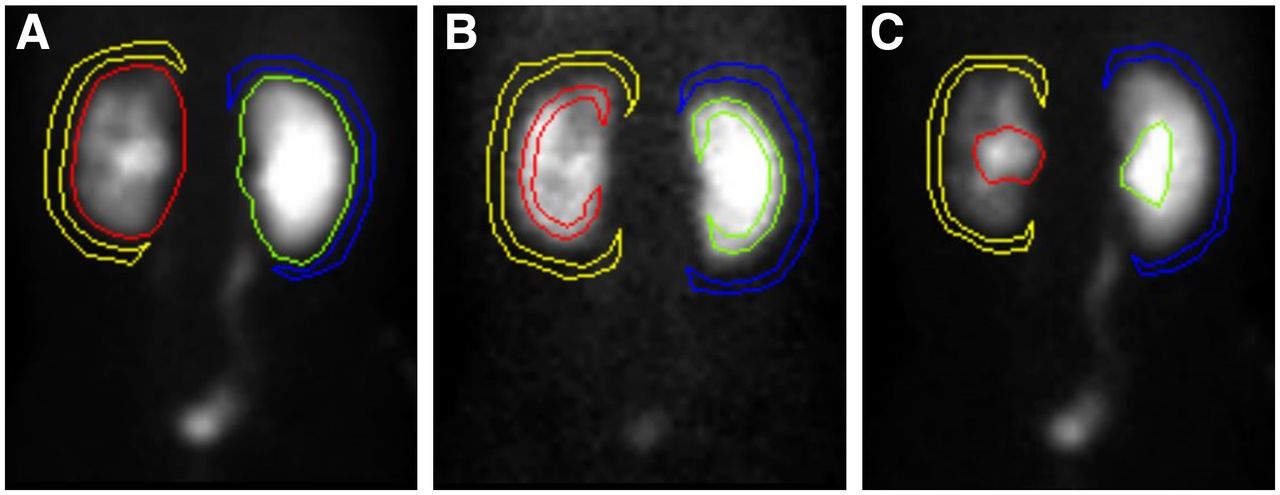
Kidney and background ROI techniques. (A) WK ROI with perirenal background. (B) Cortical ROI with perirenal background. (C) CS ROI with perirenal background. Yellow = left kidney background; red = left kidney; green = right kidney; blue = right kidney background.
- FIGURE 6.
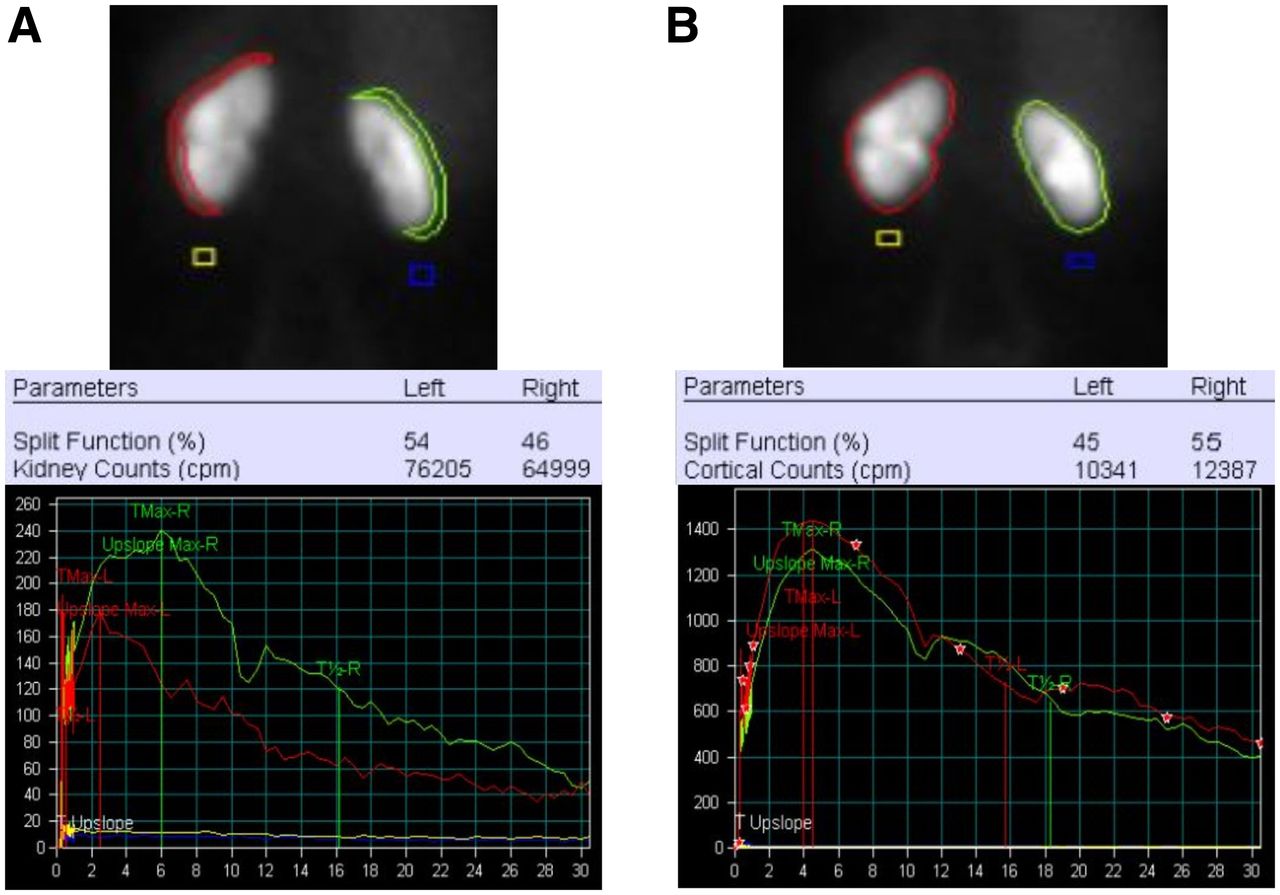
Cortical vs. WK for determination of relative function. (A) Cortical ROIs, calculated relative (split) function, and cortical time–activity curves. (B) WK ROIs, calculated relative (split) function, and WK time–activity curves. Cortical data incorrectly show right kidney to have decreased function compared with left, 46% vs. 54%. Correct data are shown by WK data, with right kidney having greater function than left, 55% vs. 45%, difference of 9%. Also note, a crescent shaped background region of interest is preferred over square background region (yellow and blue).
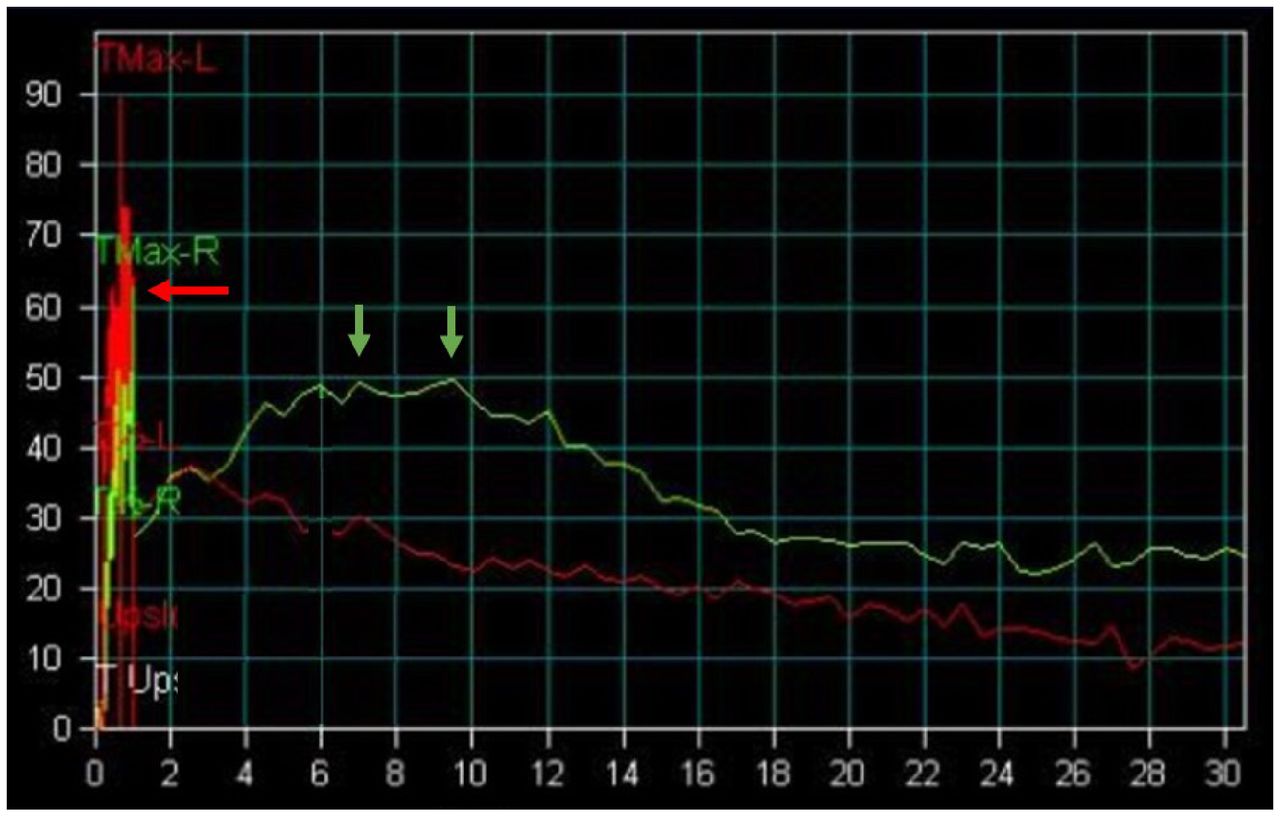
- FIGURE 7.
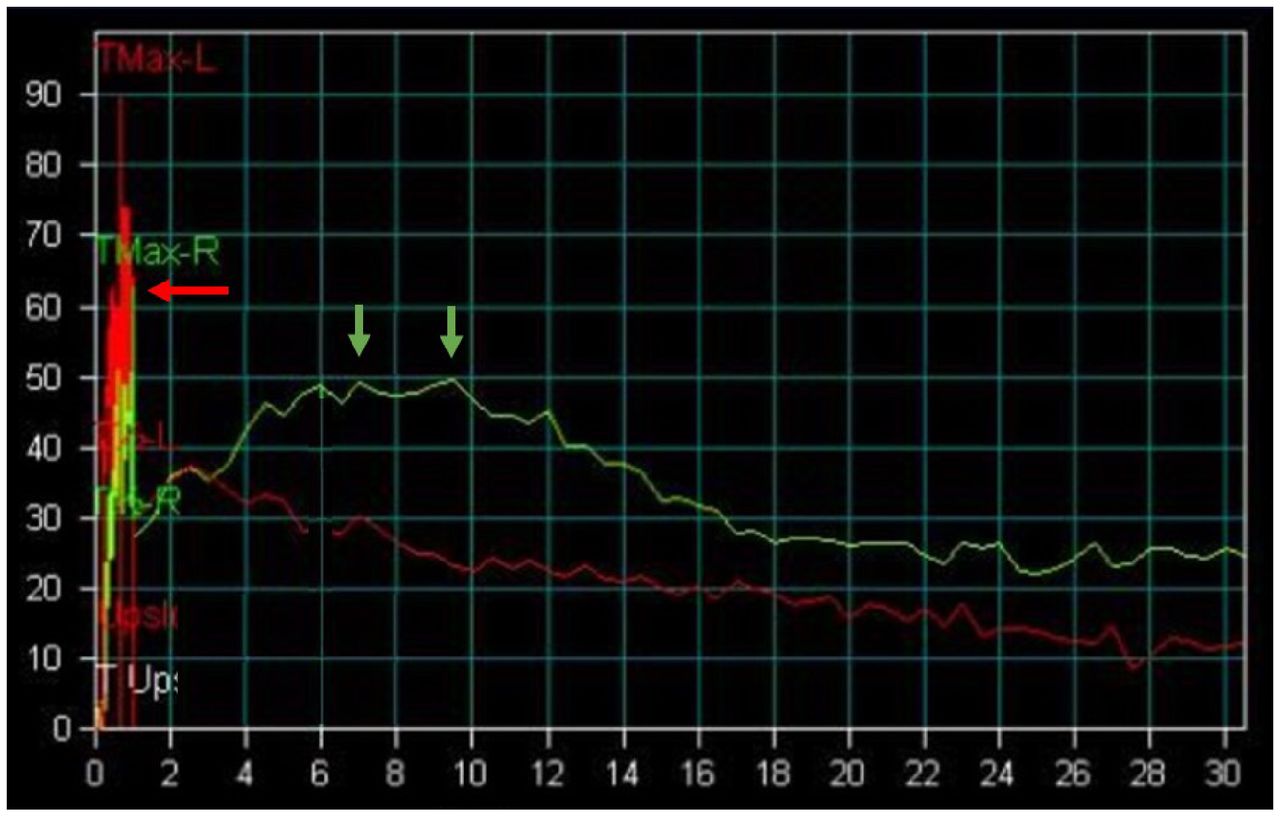
Extensive motion artifact involving first minute of time–activity curve representing flow phase acquired at 1 s per frame. This results in erroneous elevated value at 1 min due to ROIs overlapping vascular activity in liver and spleen (red arrow). Actual right kidney Tpeak is delayed (>5 min) in 7- to 9-min range (green arrows).



Tables
Parameter Best practice Patient preparation Increase in fluid intake day before and morning of examination It may be optimal also to have patient avoid natural diuretics, though some experts believe effect is less than fluid consumed Withdrawal of prescribed diuretics on morning of examination Thiazides: hydrochlorothiazide, indapamide, metolazone, chlorthalidone Loop diuretics: furosemide, bumetanide, torsemide, ethacrynic acid Potassium sparing: amiloride, spironolactone, triamterene, eplerenone Carbonic anhydrase inhibitors: acetazolamide Oral hydration 30–60 min beforehand Patient drinks 5–10 mL/kg 450–900 mL (15–30 oz, or 2–4 cups) for adults weighing 90.7 kg (200 lb) 385–770 mL (13–26 oz, or 1.5–3 cups) for adults weighing 77.1 kg (170 lb) Prevoiding Patient voids immediately before beginning of examination Acquisition 99mTc-MAG3, 37–185 MBq (1–5 mCi) intravenously 99mTc-MAG3 is preferred over 99mTc-DTPA despite cost; lower doses are adequate given that flow/arterial phase can be omitted Furosemide, 40 mg intravenously If patient is on higher dose of furosemide at home, increase to match; consider 80–120 mg if known renal insufficiency Serum creatinine level > 1.2 ng/dL (women) or > 1.4 ng/dL (men) Estimated GFR < 90 mL/min/1.73 m2 (either sex) Acquisition and timing of diuretic (most common source of variability; remains actively debated topic with no clear best practice for all situations) F=0 single acquisition or F+20 2-part acquisition; F+10, F+15, and F+30 are also used by many practices, and F+10sp is also considered suitable technique Postvoid image (maximizes pressure differential between kidneys and bladder, facilitating physiologic drainage) Patient stands or walks for 5 min, voids, and then is imaged in same position as examined Many quantitative values are dependent on protocol and cannot be universally applied.
Parameter Best practice Processing WK ROI Is essential for relative function measurement; generally adequate if kidney function is normal Cortical ROI Includes only parenchyma, not CS and calyces; optimal for assessing functional parameters such as 20-min/max (renal retention) and Tpeak CS ROI Excludes parenchyma and has been shown to better represent CS drainage when calculating T-½ Background ROI Is C-shaped or reniform, 2 pixels wide, and 1 pixel away from cortex Relative (split) function Must be derived from WK ROIs; may be measured using 2- to 3-min intervals, but intervals of 1–2 or 1–2.5 min are recommended if F=0 protocol is used Quantification Relative (split function) Normal is 45%–55%; abnormal if <40% Tpeak Normal is <5 min T-½ emptying Normal is <10–15 min; abnormal does not equate to obstruction 20-min/max Normal is <0.35 as measured 20 min after Tpeak Tissue transit time Activity should be seen in CS by 5 min; >8 min is delayed Postvoid kidney to maximum Postvoid image is acquired 30 min after start, and activity is compared with Tpeak Output efficiency Helps overcome confounding effect of poor renal function on CS drainage assessment; requires special processing software Normalized residual activity Normal is <1.0 for 20- to 21-min interval and <0.10 when using 1-min interval acquired after voiding at 60 min from examination start Many quantitative values are dependent on protocol and cannot be universally applied.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}