


Abstract
Diuretic renal scintigraphy plays a critical diagnostic role by providing a physiologic means for differentiating between obstructive and nonobstructive hydronephrosis and by assessing the function of the affected kidney. The examination accuracy is highly dependent on and benefits from close attention to the protocol. This article reviews kidney anatomy and physiology, patient preparation, available radiopharmaceuticals, diuretic administration, acquisition, processing, quantification, and interpretation criteria in the United States.
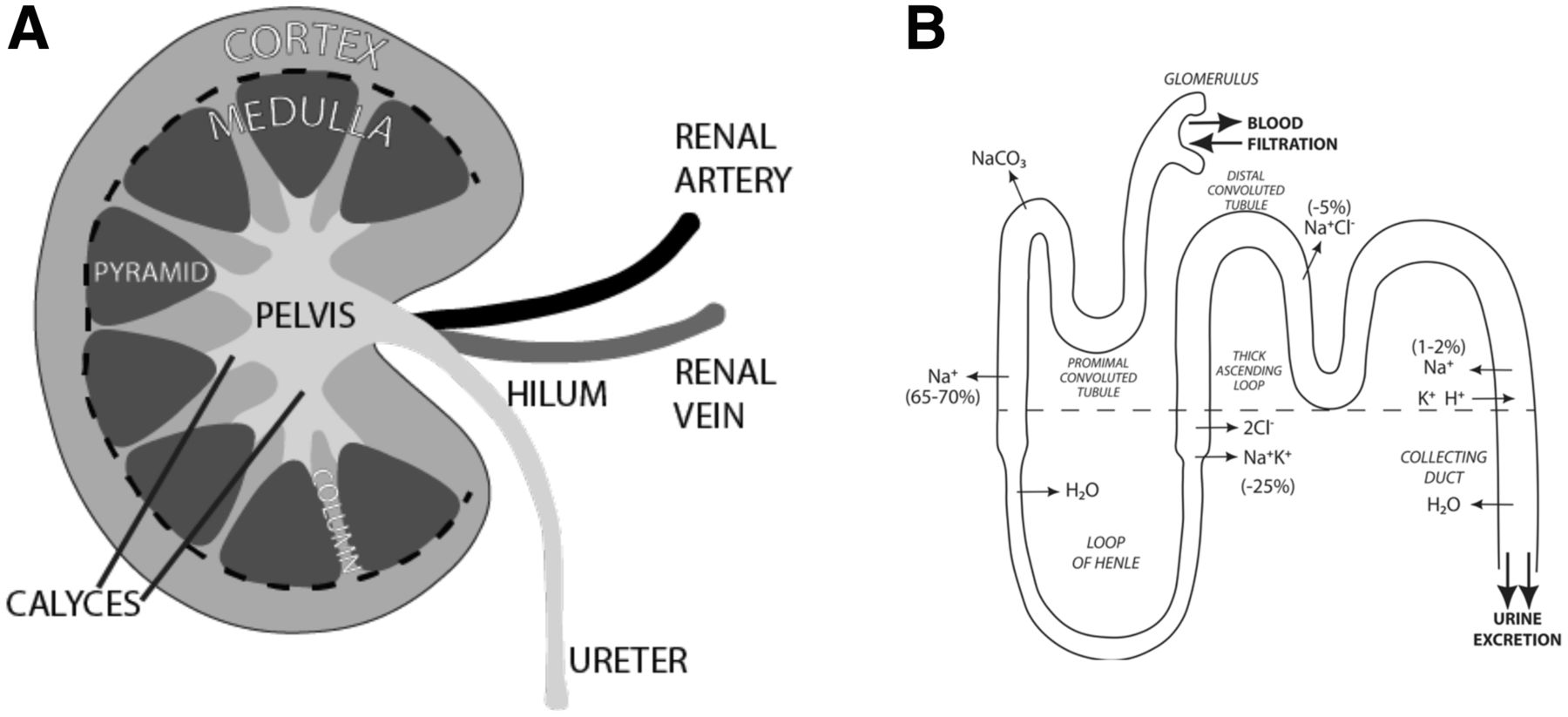
The role of the kidneys is to cleanse the blood of waste and turn the waste into urine while also maintaining the balance of fluid and electrolytes, particularly sodium. The paired organs are located along the posterior abdominal wall, on each side of the spine, between the levels of T12 and L3. Measuring about 10–13 cm in length, the kidneys are bean-shaped, with their long axis lying almost parallel to the body. The indentation of the bean, called the renal hilum, is oriented toward the spine. It is where arterial blood containing waste enters the kidney, cleansed venous blood exits, and urine containing waste exits. The renal parenchyma consists of an outer cortex and an inner medulla, encompassing the urine-collecting system (CS) comprising calyces and the renal pelvis (Fig. 1A). Each kidney has approximately a million small filters called nephrons within the parenchyma. Each nephron is a long, fine convoluted tubule 3–6 cm long, originating in the cortex at its glomerulus and ending in the medulla at the collecting duct (Fig. 1B). At the end of the collecting ducts, urine containing waste passes into the calyces and is then collected in the funnel-shaped renal pelvis. The pelvis drains via the ureter to the bladder.

Kidney anatomy and glomerulus function. (A) Kidney is bean-shaped paired organ. Indentation is called hilum and is where renal artery enters, whereas renal vein and ureter exit. Parenchyma comprises outer cortex and inner medulla, with medulla further subdivided into pyramids and columns. This all surrounds CS, which is made up of multiple calyces feeding into pelvis. (B) Blood enters glomerulus containing waste and then leaves filtered. Nephron travels into and out of cortex (separated by dashed line), whereas electrolytes are exchanged and urine concentrated before being excreted into calyces.
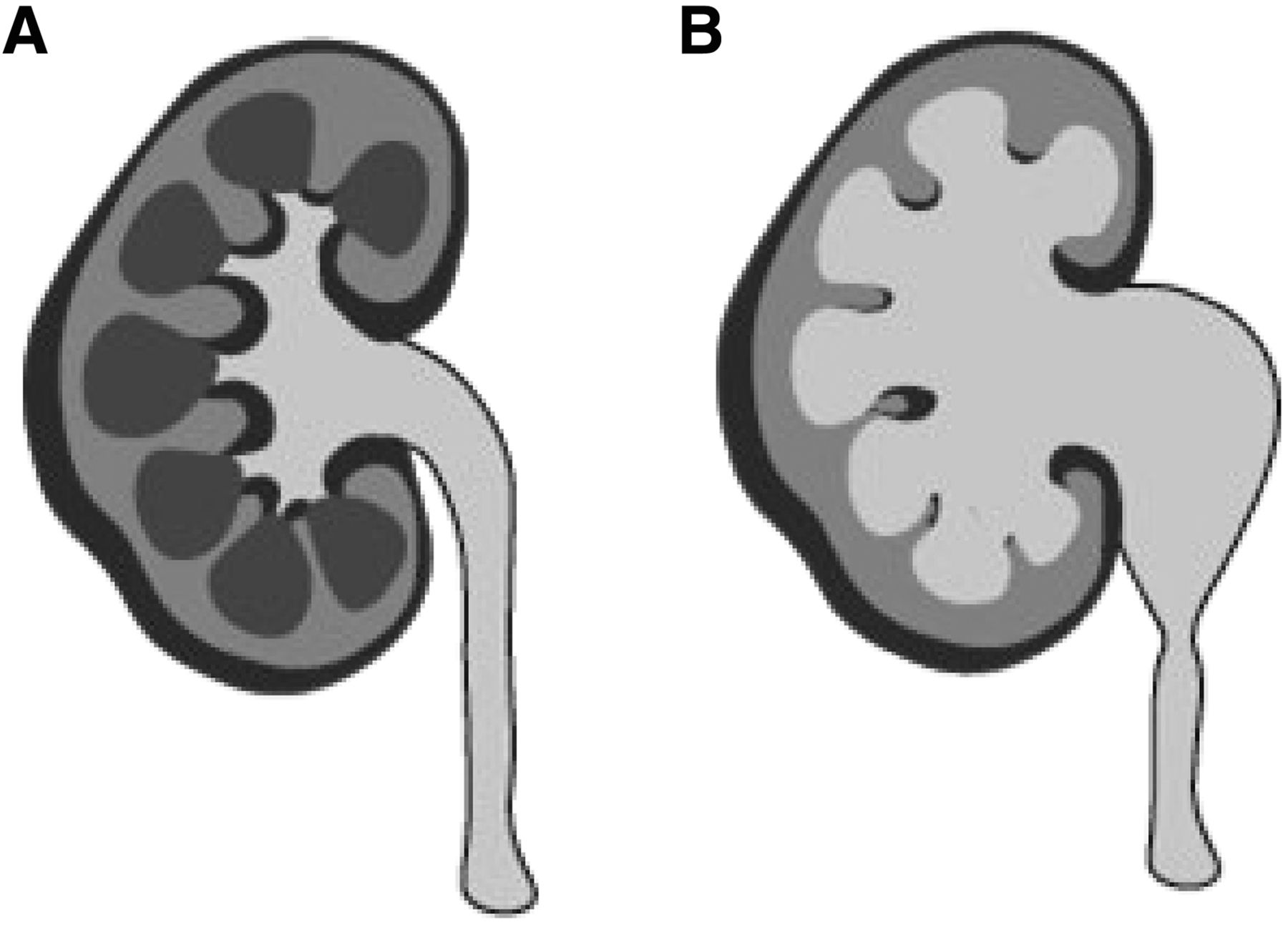
The normal drainage of urine can be blocked because of a wide range of congenital and acquired disorders. Obstruction to urinary outflow may, in turn, lead to increased pressure in the renal CS and its subsequent dilatation and swelling of the kidney (Fig. 2). This condition, termed hydronephrosis, can lead to injury of the parenchyma and loss of function. Concern about obstruction is usually raised by detection of an elevated serum creatinine level versus imaging findings of a dilated renal pelvis or calyces. Occasionally, it may also be suspected in a patient undergoing follow-up after attempted correction of a previous obstruction (1). Unfortunately, neither a decline in renal function nor CS dilation on imaging is specific for obstruction; these findings may be due to a wide variety of nonobstructive disorders such as infection, vesicoureteral reflux, congenital anomalies, or residual changes after the resolution of a previous obstruction. Hence, in this scenario, diuretic renal scintigraphy (DRS) plays a critical diagnostic role by providing a noninvasive physiologic means for differentiating between obstructive and nonobstructive hydronephrosis as well as assessing the function of the affected kidney (2). The examination is based on the principle that under physiologic conditions, urine may be retained in a hydronephrotic renal pelvis for 1 of 2 reasons: either an anatomic obstruction preventing outflow or the reservoir effect, in which urine pools in the dilated renal pelvis until enough accumulates to spill over into the ureter. The reservoir effect is a pseudoobstruction that can mimic a mechanical obstruction, leading to unnecessary urologic interventions. DRS takes advantage of the fact that the reservoir effect can be overcome under high-flow conditions created with diuretic administration. By evaluating the washout of radiopharmaceutical from the CS and analyzing the parenchymal function, the presence of an obstruction and risk of renal damage can often be correctly assessed.
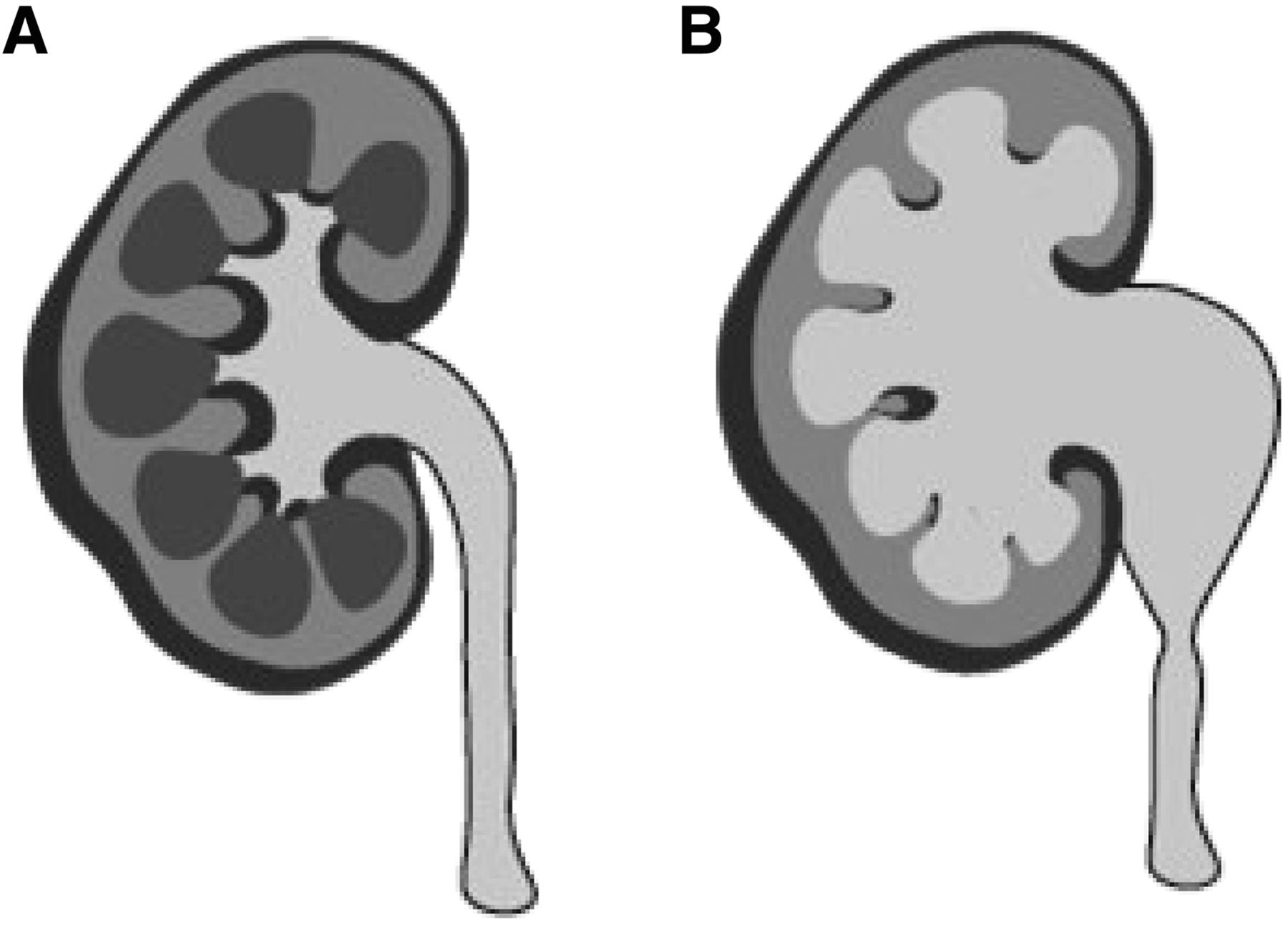
(A) Normal kidney demonstrates small calyces and decompressed renal pelvis. (B) With obstruction (and other disorders), calyces and pelvis become dilated.
BACKGROUND
Before the advent of DRS, obstructive hydronephrosis was distinguished from nonobstructive by an invasive means: a pressure perfusion study, commonly known as the Whitaker test. The Whitaker test involved percutaneous kidney access via a posterior approach. A catheter was introduced into the dilated renal pelvis, and fluid was instilled at a flow rate of 5–10 mL/min while the pressure was monitored in the renal pelvis and bladder (3). An unobstructed renal pelvis and ureter tolerated this high flow readily, with no or only a small rise in pressure from baseline. However, if the pressure between the renal pelvis and bladder rose significantly, often greater than 15–20 cm of water, then the system was deemed obstructed (4). Fortunately, in 1979, DRS was introduced using 131I-hippuran (orthoiodohippurate) and furosemide, offering a simpler, noninvasive means for evaluating equivocal pelviureteral obstruction (5,6). Soon thereafter, in 1980 (7) and 1986 (8), 99mTc-diethylenetriaminepentaacetate (99mTc-DTPA) and 99mTc-mercaptoacetyltriglycine (99mTc-MAG3), respectively, were introduced, both of which are still in widespread use today.
The examination accuracy is highly dependent on and benefits from close attention to patient preparation, timing of diuretic, method of acquisition, processing, quantification, and interpretation criteria (Tables 1 and 2).
Approach to Best Practices for Adult DRS: Patient Preparation and Acquisition
Approach to Best Practices for Adult DRS: Processing and Quantification
PREPARATION
The ability of the kidneys to significantly increase urine production in response to diuretic administration is central to the diagnostic accuracy of DRS. An increase in urine production is determined by both renal function and hydration.
To best ensure appropriate hydration, the patient should be instructed to increase fluid intake the day before and the morning of the examination while avoiding natural diuretics (typically coffee, tea, and other caffeinated beverages). An additional 12 ounces of fluid with each of the 3 meals (totaling approximately 1 L) before the examination is a reasonable goal. This step is contraindicated in individuals on a fluid-restricted diet, which is most commonly a treatment for congestive heart failure and for rare disorders such as adrenal insufficiency and hyponatremia. Additionally, unlike many other nuclear medicine examinations, fasting beforehand should be discouraged since this could impair efforts to prehydrate.
Once the patient arrives at the clinic, additional oral hydration is recommended during the 30–60 min immediately preceding the examination. The preferred amount of oral hydration is 5–10 mL/kg based on an international scientific committee’s consensus report (9), which was subsequently endorsed by the Society of Nuclear Medicine and Molecular Imaging (SNMMI) and the European Association of Nuclear Medicine (EANM) (10).
Patients prescribed diuretics as part of their routine medical care should be instructed to refrain from taking these medications the morning of the examination. Diuretics are most commonly prescribed for hypertension and to treat edema from heart, kidney, or liver failure. Having the patient withhold diuretics helps ensure adequate prehydration while avoiding the possibility of commencing the examination during an ongoing prescribed diuresis, which can last for 6–8 h after oral administration of furosemide (11).
Additionally, though not explicitly recommended in the applicable guidelines and parameters, kidney function assessment before the examination can help ensure the likelihood of a diagnostic examination. As renal function decreases, urine production and responsiveness to diuretics decrease. Hence, patients with impaired renal function may not have an adequate escalation in urine flow from the standard 40-mg intravenous dose of furosemide. Therefore, the dose may need to be increased to achieve significant enough diuresis for diagnostic DRS results (12). Fortunately, in many cases, renal function testing is obtained as part of clinical care, and the resulting serum creatinine or estimated glomerular filtration rate (GFR) may be used to determine an optimal diuretic dose. It is generally agreed on that an abnormal serum creatinine level (>1.2 ng/dL in women and >1.4 in men) usually indicates a 50% loss of renal function (i.e., GFR) and the need to increase the dose administered for DRS (10).
Unfortunately, only case reports are available comparing the effectiveness of higher doses of furosemide with the standard 40-mg dose in patients with compromised renal function, and thus no evidence-based recommendations can be made (13). Given this, the SNMMI–EANM recommends a simple approach of doubling the dose of furosemide to 80 mg for patients with an elevated serum creatinine level or a depressed estimated GFR (<90 mL/min/1.73 m2).
Some practices have further increased the dose to 120 mg or more in individuals with severe renal impairment (estimated GFR < 30 mL/min/1.73 m2), given that prior research has shown that up to 171 mg may be necessary to achieve maximal diuresis when the estimated GFR reaches 15 mL/min/1.73 m2 (14). One caveat to this approach is that individuals on chronic diuretic therapy are usually given at least the intravenous equivalent of their prescribed outpatient oral dose, with 1:2 being an acceptable intravenous-to-oral conversion for furosemide. The conversion for bumetanide and torsemide is 1:1 (15).
The final recommended preparation step is to start an intravenous line and have the patient void the bladder immediately before the examination begins. Voiding can reduce the possibility of patient motion from discomfort or needing to terminate the study prematurely for the patient to urinate. It also minimizes the backpressure effect that a distended bladder may have on slowing the draining of the upper tracts (16–19).
RADIOPHARMACEUTICAL
Two radiopharmaceuticals are currently in use for DRS: 99mTc-DTPA and 99mTc-MAG3. 99mTc-DTPA is entirely filtered by the glomerulus, allowing it to be used to measure GFR and assess the differential or relative function of each kidney and potential outflow obstruction (20). However, the kinetics of 99mTc-DTPA are poor in the setting of reduced renal perfusion and function, potentially leading to spurious results (21). In contrast, 99mTc-MAG3 undergoes extraction predominately by the tubular cells and is then secreted into the renal CS. Because its extraction fraction is more than twice that of 99mTc-DTPA, 99mTc-MAG3 kinetics are much less affected by impaired renal perfusion and function, providing superior image quality and making it the preferred agent 3:1 by institutions despite increased cost (22–24). For this reason, 99mTc-MAG3 is recommended for DRS by the SNMMI, EANM, and Society of Fetal Urology (16,25,26).
The appropriate administered activities of 99mTc-MAG3 and 99mTc-DTPA are not clearly established. Documentation of the American College of Radiology and Society of Pediatric Radiology states that up to 370 MBq (10 mCi) of 99mTc-MAG3 and up to 555 MBq (15 mCi) of 99mTc-DTPA may be used (20). The SNMMI–EANM procedure standard says that up to 370 MBq (10 mCi) is acceptable for either radiopharmaceutical, but 37–185 MBq (1–5 mCi) is preferred since a higher administered activity is significantly helpful only when higher counts are necessary for evaluating the arterial flow of a transplanted kidney (10,27).
The recommendation for using a lower administered activity was supported, in part, by a masked comparison of DRS examinations with and without the aid of the initial 1-min flow images. The results showed no significant difference in the ability to determine whether a kidney was obstructed (28). Furthermore, this same paper demonstrated the diagnostic equivalence of a lower (62.9 MBq [1.7 mCi]) and a higher administered activity (303 MBq [8.2 mCi]) of 99mTc-MAG3 for determining relative or split renal function. That said, no head-to-head studies of a higher (222 MBq [6–10 mCi]) versus a lower (37–185 [1–5 mCi]) administered activity have been performed to confirm the SNMMI–EANM recommendation for using a lower administered activity when evaluating for urine outflow obstruction. Interestingly, a recent survey of 110 U.S. nuclear medicine labs seeking Intersocietal Accreditation Commission (IAC) accreditation showed that a median administered activity of 370 MBq (10 mCi) for 99mTc-MAG3 and 447.7 MBq (12.1 mCi) for 99mTc-DTPA is used for DRS. The study also revealed that 10% of sites successfully use an administered activity averaging 185 MBq (5 mCi) (29).
DIURETIC
By far the most commonly used diuretic for DRS is furosemide, being universally used by 107 of 110 sites in the study of IAC-accredited nuclear medicine labs (24). Furosemide is a loop diuretic, meaning it decreases sodium and chloride absorption in the kidney at the ascending loop of Henle, which in turn increases water excretion (30). The adult dose of intravenous furosemide recommended by SNMMI–EANM is 0.5 mg/kg, versus 0.5–1.0 mg/kg recommended by the American College of Radiology–Society of Pediatric Radiology, with agreement on a maximum dose of 40 mg in healthy adults. A 40-mg intravenous dose of furosemide has been shown to achieve maximal diuresis in adults with normal renal function (10).
When administered intravenously, furosemide has an onset of action of approximately 5 min and reaches peak effect starting at 15 min, achieving 200–300 mL of urine production within 20–30 min after injection (31). In young, healthy adults, however, 20–30 mg may produce a diuresis sufficient for DRS and is preferred by some, given that it may avoid premature study termination in these patients because of the need to urinate (10).
Given the average weight of U.S. adults, the 40-mg dose is suitable for most patients without a history of renal insufficiency. However, those with decreased kidney function may benefit from an increased dose of 80 mg or higher in the setting of severe renal failure, whereas those on furosemide as an outpatient should receive at least as much as the intravenous equivalent of their prescribed oral dose. When higher doses of furosemide are being considered, particularly in elderly or fragile patients, it is important to consider the possibility of inducing severe drops in blood pressure, including stroke. One should consider discussing the use of high-dose furosemide with the ordering clinician.
Though infrequently used, 1 mg of intravenous bumetanide, another loop diuretic, is an acceptable alternative to DRS if furosemide is unavailable (14). Both furosemide and bumetanide contain a sulfonamide moiety similar to sulfur-containing antibiotics. Therefore, some practitioners prefer to avoid these drugs in patients with a known sulfa allergy and instead choose mannitol or ethacrynic acid (32,33). However, the concern for sulfur cross-reactivity has not been supported by research. A retrospective review of 88 patients who had a history of sulfa allergies and received intravenous furosemide demonstrated only 2 instances of potential allergic reactions. In both cases, minor rashes were treated effectively with a single dose of diphenhydramine (Benadryl; Johnson & Johnson) (34). Another study had similar reassuring results, showing no allergic reactions in 34 patients who had a reported history of sulfa allergies and were treated with sulfonamide-containing diuretics for intracranial hypertension (35). Hence, many experts now agree that these diuretics are safe for DRS in patients with a known sulfa allergy.
One of the most significant sources of debate in DRS concerns the timing of diuretic administration in relation to radiopharmaceutical administration. The parameter of the American College of Radiology and Society of Pediatric Radiology discusses 3 options, the F+20 (furosemide administered 20 min after the radiopharmaceutical), the F+0 (furosemide and radiopharmaceutical administered simultaneously), and the F−15 (furosemide administered 15 min before administration of the radiopharmaceutical).
The F+20 protocol is probably the most widely recognized approach, having been originally endorsed as the technique of choice by the SNMMI Pediatric Nuclear Medicine Council along with the Society of Fetal Urology (36). Unfortunately, up to 25% of examinations may result in equivocal results when a dilated renal pelvis empties very slowly after administration of the diuretic, preventing exclusion of a partial obstruction (37). This finding may occur when a large portion of the administered radiotracer is eliminated from the renal pelvis before the diuresis has a large enough impact on urine flow to demonstrate normal emptying (38).
In an attempt to reduce the number of equivocal results, the F−15 min approach was developed, taking advantage of the fact that maximal diuresis occurs 15–18 min after the intravenous administration of furosemide. Unfortunately, when this technique has been used, the examination has not been completed in up to 30% of patients because of the need to urinate before the study is over (10,39).
As a result, some experts have advocated for the F+0 protocol, a hybrid approach that shortens the procedure, reduces equivocal results, and improves patient comfort (40,41). However, the drawbacks to the early administration of diuretic (F−15 or furosemide and radiopharmaceutical administered simultaneously [F=0]) is that it precludes the observation of natural urine drainage kinetics, and in the setting of a poorly functioning kidney, these protocols may not allow enough time for filling of the CS and hence determination of outflow obstruction.
Thus, some experts still prefer to wait until 20 min (or later, such as F+30 or Fmax, a protocol in which the diuretic is not given until CS activity appears to have reached a maximum) after radiopharmaceutical administration to give the furosemide, whereas others have created additional protocol variants, such as F+2, F+5, and F+10, all of which likely provide diagnostic results in a large percentage of cases (10). Hence, it is still a matter of institutional and provider preference as to which approach is best for their patients. This preference is reflected in current practice patterns, with a total of 34 different approaches to the timing of diuretic administration in use among 107 sites undergoing genitourinary imaging accreditation with the IAC (24). That said, most of these sites (56%) use 1 of 5 approaches, F=0, F+10, F+15, F+20, or F+30, with the F+20 approach being most common (21% of sites).
One final note on the subject is that recently, there has been increasing interest in a variation termed F+10sp, which performs the examination with the patient in the seated position (sp) instead of supine as recommended in the guidelines. The seated position was used in the original 1978 F+20 studies introducing DRS but was changed to supine positioning as the test became widely adopted to reduce patient movement and avoid the risk of a fall secondary to potential diuresis-induced hypotension (42,43). The seated position takes into account the recognized importance of gravity assistance for the physiologic drainage of urine from a dilated CS.
ACQUISITION
For either 99mTc-MAG3 or 99mTc-DTPA, images from γ-cameras with a large field of view (400 mm) are ideally obtained with a low-energy all-purpose collimator or, as an acceptable alternative, a low-energy high-resolution collimator (20). A low-energy all-purpose collimator is preferred because, despite the slightly lower resolution, the higher counting rates result in reduced noise for quantitative measurements, particularly when using small cortical regions of interest (ROIs) (10).
Current guidelines and parameters recommend that the patient be positioned supine with the camera at the patient’s back, to take advantage of the typically posterior position of native kidneys. However, for a transplanted pelvic kidney, the camera should instead be anterior (10,20). Given that drainage of a dilated CS may be delayed in this position, even in the absence of obstruction, there is renewed interest in performing the examination with the patient seated to allow gravity to assist (44). Nevertheless, only 1 of the 107 sites undergoing nuclear medicine genitourinary accreditation at the end of 2018 used the seated position (4).
One topic of debate is how to address nephroptosis, a condition in which a native kidney drops into the pelvis when the patient is standing, potentially resulting in a transient obstruction. This finding has been observed in up to 22% of individuals referred for DRS and may negatively impact both the measured relative function and the CS drainage of the ptotic kidney, depending on the position used during imaging (45). Thus, 2 examinations of the patient—supine and seated—might be best in this scenario.
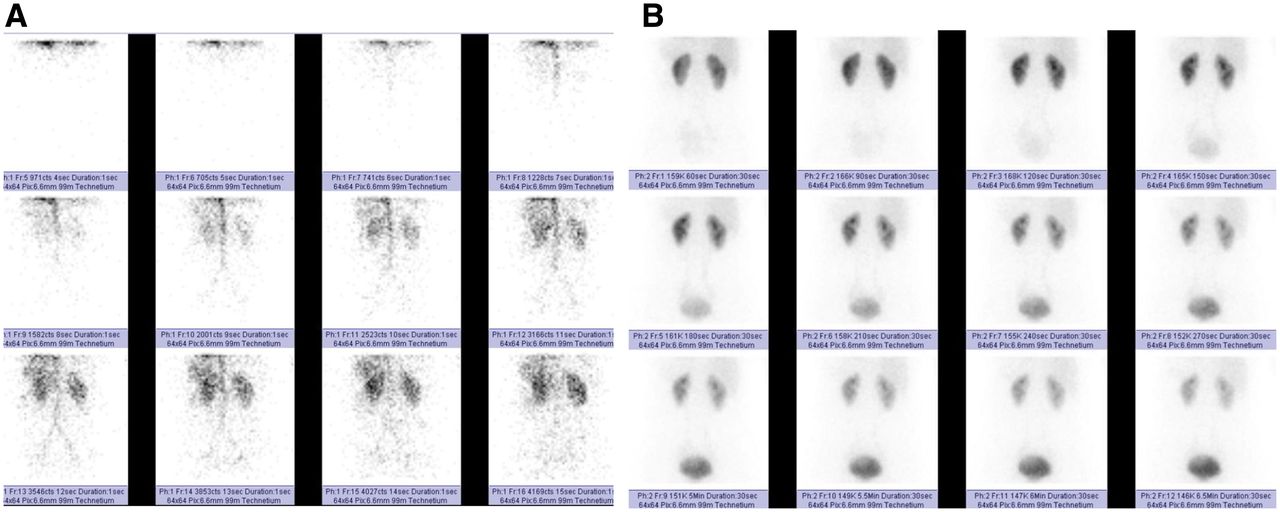
When DRS begins, the first minute of imaging is typically acquired using 1- to 3-s images to assess renal arterial flow (Fig. 3A). Starting with minute 2, all subsequent images are acquired for 15–60 s and are used to evaluate the parenchymal function and urine outflow from the CS (Fig. 3B). This technique can be performed as either a single or a 2-phase acquisition, depending on the timing of diuretic administration. Traditionally, if the diuretic is given before or simultaneously with the radiopharmaceutical, a single acquisition is used. If the diuretic is administered 20 min or later into the study, the acquisition is typically 2 separate phases based on the Santa Fe consensus (10). The first acquisition is performed for 20–30 min without diuretic augmentation; afterward, the patient stands or walks for a while and then voids. If the baseline study is suggestive of obstruction, the intravenous diuretic is given and an additional 20 min of imaging is performed (Fig. 4) (16).

(A) First-minute blood flow phase with frames acquired every second (first 12 s displayed). (B) Dynamic phase with frames acquired every 30 s (minutes 2–7 displayed). Phase is helpful for assessing both parenchymal function and urine drainage.
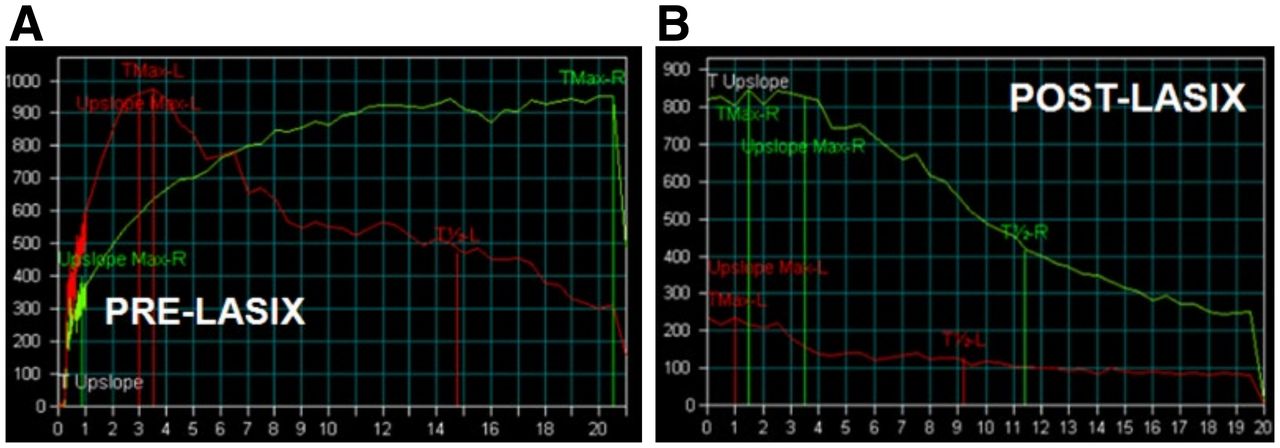
Dual-phase acquisition. (A) First 20 min of findings for right kidney are concerning for obstruction, necessitating diuretic administration. (B) Postdiuretic T-½ of slightly less than 10 min excludes obstruction. Green curve = right kidney; red curve = left kidney; Lasix (Aventis Pharma) = furosemide.
Although imaging of renal perfusion using 1- to 3-s images of the initial radiopharmaceutical bolus as it transits the aorta and renal arteries is typical, it has not been demonstrated to provide useful information for interpretation of DRS. Therefore, experts agree that this traditional protocol component can be omitted, simplifying both interpretation and reporting while also lowering administered activity (28).
CS emptying can be delayed in the absence of obstruction when the patient is supine. A postvoid image is recommended by both the SNMMI–EANM guideline and the American College of Radiology–Society of Pediatric Radiology parameter to account for this delay. The image is obtained after the patient stands, ambulates for 5 min, and then voids before getting back into the supine position for this final image. The image should be acquired using the same interval (15–60 s) as the previous images to optimize comparison (10). Some experts consider measurement of the voided urine volume helpful. At least 200 mL of urine produced over a 20-min acquisition and 300 mL over a 30-min acquisition indicate adequate hydration and response to the diuretic (44). Despite the simple nature of this potentially helpful adjunct, none of the facilities undergoing IAC accreditation during the cycle ending in 2018 included this step in their adult DRS protocol (24).
PROCESSING
Time–activity curves are generated by placing ROIs around all or portions of the kidneys. The whole-kidney (WK) ROI, which includes all of the renal parenchyma and pelvis, is necessary to assess relative function accurately. It may also be used to evaluate other parameters such as time-to-peak (Tpeak—the time from baseline to maximum activity in the WK ROI), T-½ emptying (the time for activity in the ROI to decrease by 50% from Tpeak), and 20-min/max (the percentage of activity remaining 20 min after Tpeak) (Fig. 5A). Because this curve is affected by activity in both the parenchyma and the pelvis, an abnormality in one can give the perception of an abnormality in another. As such, a diseased cortex as seen with chronic renal failure from disorders such as hypertension or glomerulonephritis can lead to a prolonged T-½ emptying in the absence of urine outflow obstruction, whereas stasis of activity in a dilated CS may result in a spuriously high 20-min/max and the appearance of cortical dysfunction.

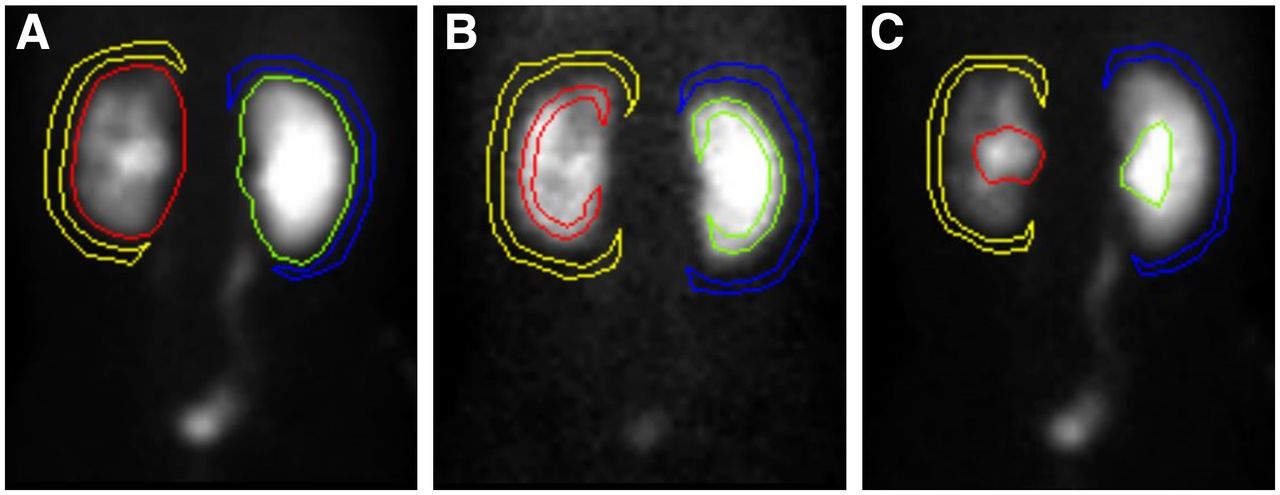
Kidney and background ROI techniques. (A) WK ROI with perirenal background. (B) Cortical ROI with perirenal background. (C) CS ROI with perirenal background. Yellow = left kidney background; red = left kidney; green = right kidney; blue = right kidney background.
To address problems from the WK ROI, additional ROIs may be created explicitly encompassing the renal cortex or the CS, and their subsequent time–activity curves can be used for analysis. The cortical ROI is created by delineating the cortex while excluding any activity in the pelvis and calyces, making it optimal for assessing parenchymal function parameters such as Tpeak and renal retention (Fig. 5B). In contrast, the CS ROI is limited to outlining the pelvis and calyces and has been shown to allow for more accurate measurement of T-½ emptying than the WK ROI (Fig. 5C) (46).
The relative function (also called the differential renal function or split function) is the percentage of renal function performed by each kidney in relation to the overall function. It is relative since it does not indicate the absolute function of each kidney (mL/min), just the percentage. Hence, a kidney with 50% renal function may be healthy but could also be poorly functioning in cases of bilateral medical renal disease, such as frequently seen with long-standing diabetes. Therefore, some facilities choose to combine the DRS examination with a plasma- or camera-based clearance measurement, such as the Christensen and Groth iterative method (single-sample plasma method) or the Gates method (camera-based method for 99mTc-DTPA) (47,48). The relative function is measured by 1 of 2 methods: either by placing a WK ROI over each kidney and measuring the integral of the counts between 1 and 2 min, 1 and 2.5 min, or 2 and 3 min after injection of the radiopharmaceutical (deconvolution method) or by using a technique called the Rutland method, which results in a Rutland–Patlak plot. Details and advantages of these techniques are provided in the consensus report by the Scientific Committee of Radionuclides in Nephrourology (9). In the integral method, if the diuretic is administered at the same time as the radiopharmaceutical, the 1- to 2-min or 1- to 2.5-min periods are preferred to minimize the possibility that activity will already have drained into the ureters and bladder and thus not be included in the WK ROI measurements, since asymmetric CS emptying would artifactually skew the results (10).
A background correction needs to be performed to correct for activity in the ROIs that is not actually in the kidney but in the blood, interstitial spaces, and tissues superficial and deep to the kidney. A separate background ROI is created beside each kidney ROI and is then normalized to account for the differences in size. The SNMMI–EANM guideline states that a perirenal background ROI, either C-shaped around most of the kidney or reniform-shaped and completely surrounding the WK ROI, 2 pixels in thickness, and 1 pixel away from the WK ROI to reduce scatter, is preferred over background rectangular or triangular shaped ROIs superior, medial, or inferior to the WK ROI (Fig. 5) (49). Fortunately, automated background assignments are an acceptable approach that reduces processing time and enhances reproducibility (10). When automated background assignments are used, it is important to review the location of the ROIs to ensure that an ROI is not drawn outside the body.
Before quantification, it is important to qualitatively evaluate the time–activity curve to assess for possible obstruction, nonobstruction, or other renal pathology. A standard, nonobstructed, time–activity curve demonstrates a rapid uptake phase based on the renal vascular supply and then a concentration and cortical transit phase, followed by an exponential excretion phase through the renal CS (left kidney in Fig. 4A). Obstruction can be suspected if a time–activity curve flattens after the peak, continues to rise throughout the time–activity curve (right kidney in Fig. 4B), or demonstrates an incomplete or delayed return to baseline. The qualitative analysis should always accompany the quantitative analysis to ensure fidelity.
QUANTIFICATION
Although the shape of the time–activity curves created from the WK ROI, and cortical or CS ROIs, if used, are central to the accurate assessment of DRS, several quantitative values have been recognized as helpful in determining obstruction and risk of future renal function decline.
Relative function is a measure of what percentage of the total renal function is performed by each kidney. It is calculated by comparing the area under the left and right WK time–activity curves from anywhere between 1 and 3 min, with the 1- to 2-min and 30-s intervals preferred. If the measurement is made after a significant amount of activity has passed into the ureter or bladder, the relative uptake measurement may be skewed because the initial amount of urine drainage from each kidney may not be proportional (10). Normal values are between 45% and 55%, but many physicians allow for greater variability and consider 40%–60% the upper limit of normal for relative function. It is important to avoid the pitfall of using the cortical data for this measurement. Although cortical ROIs are optimal for other parenchymal assessments, they do not include the entire parenchyma and thus could artificially skew the results because of ROI asymmetry (Fig. 6).
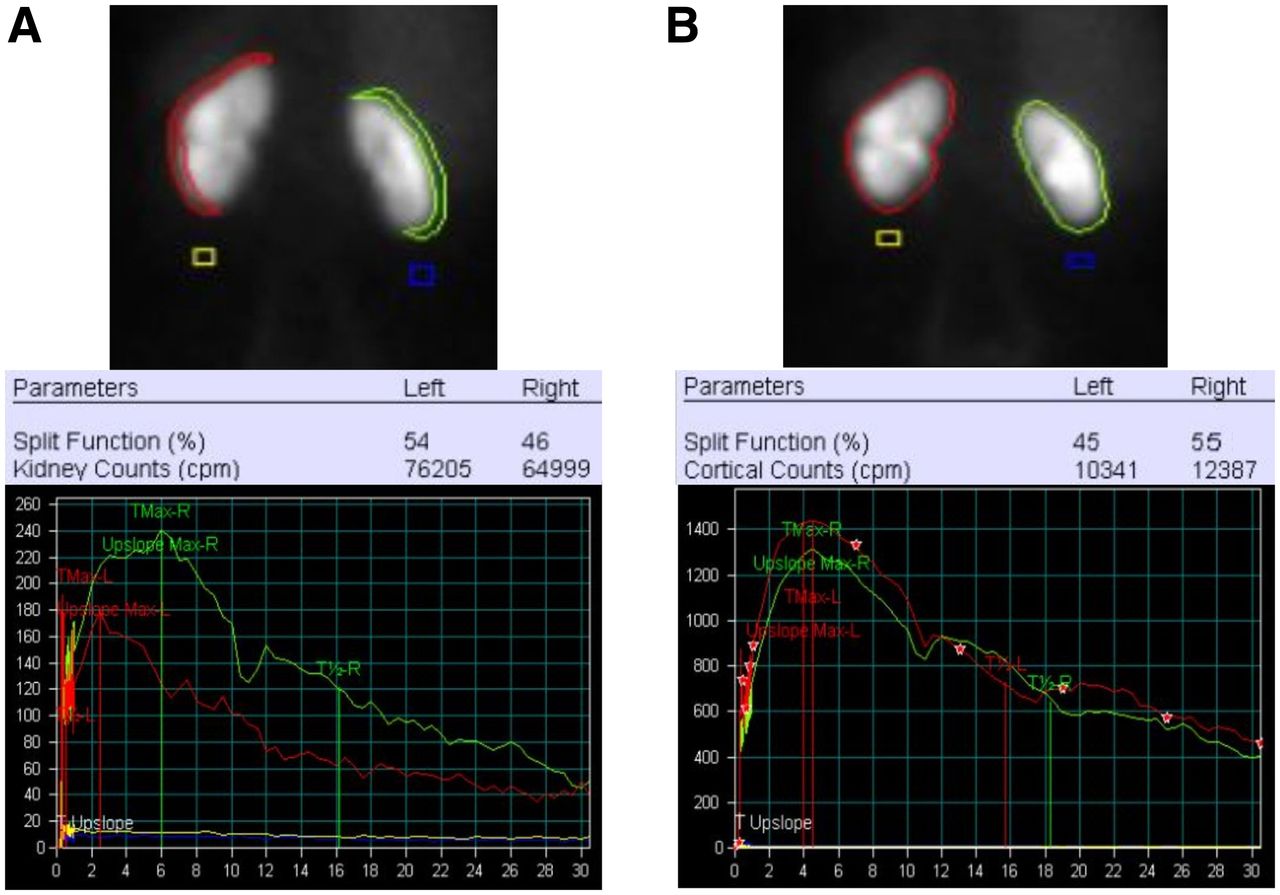
Cortical vs. WK for determination of relative function. (A) Cortical ROIs, calculated relative (split) function, and cortical time–activity curves. (B) WK ROIs, calculated relative (split) function, and WK time–activity curves. Cortical data incorrectly show right kidney to have decreased function compared with left, 46% vs. 54%. Correct data are shown by WK data, with right kidney having greater function than left, 55% vs. 45%, difference of 9%. Also note, a crescent shaped background region of interest is preferred over square background region (yellow and blue).
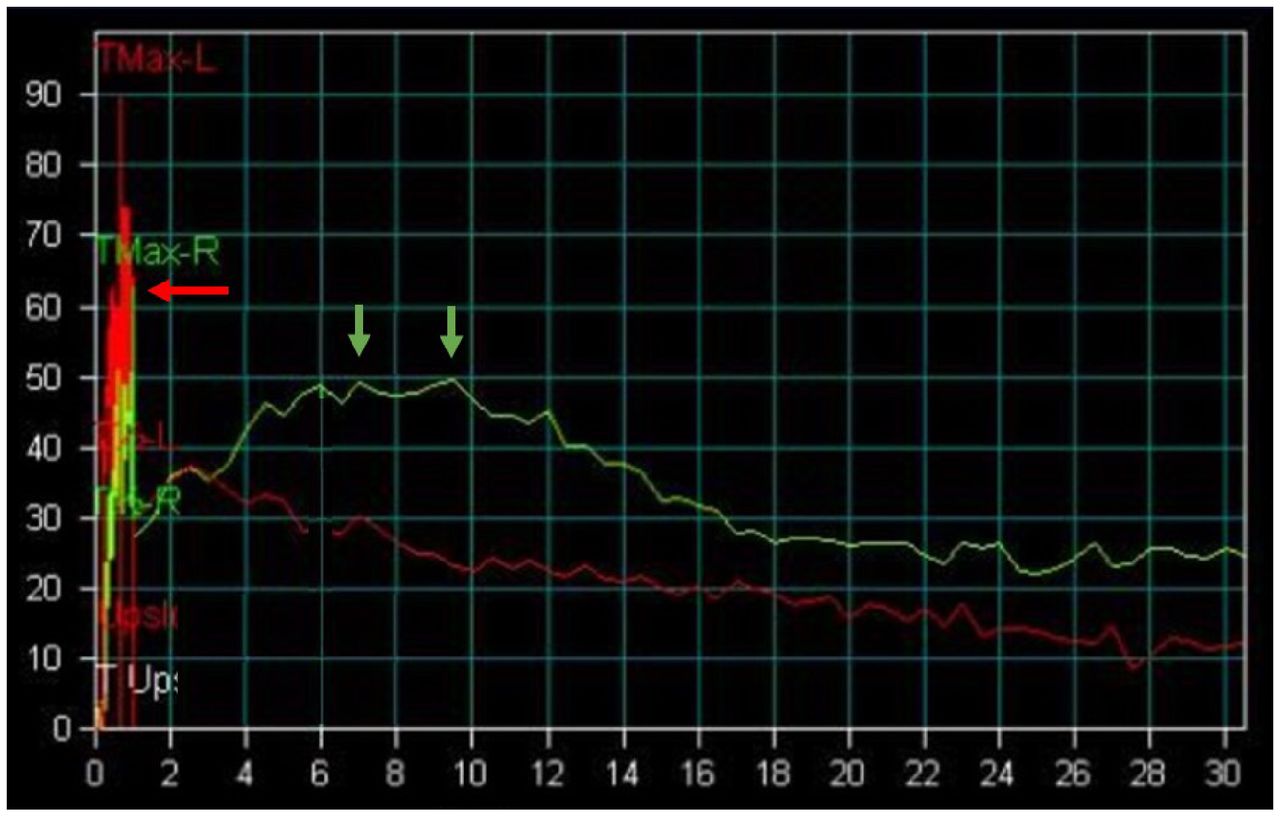
Tpeak is a marker of parenchymal function. It should occur no later than 5 min after injection of the radiotracer for either 99mTc-MAG3 or 99mTc-DTPA, whether derived from the WK or the cortical ROI. One source of error is that this value is often derived automatically, with the software assigning it on the basis of the time of the highest point of the time–activity curve. However, there are often significant errors in the first minute of the time–activity curve during the flow-phase acquisition because of the very short acquisitions (1–3 s each), which are highly prone to motion artifacts. Hence, the time–activity curve and derived Tpeak should be reviewed and corrected appropriately (Fig. 7).
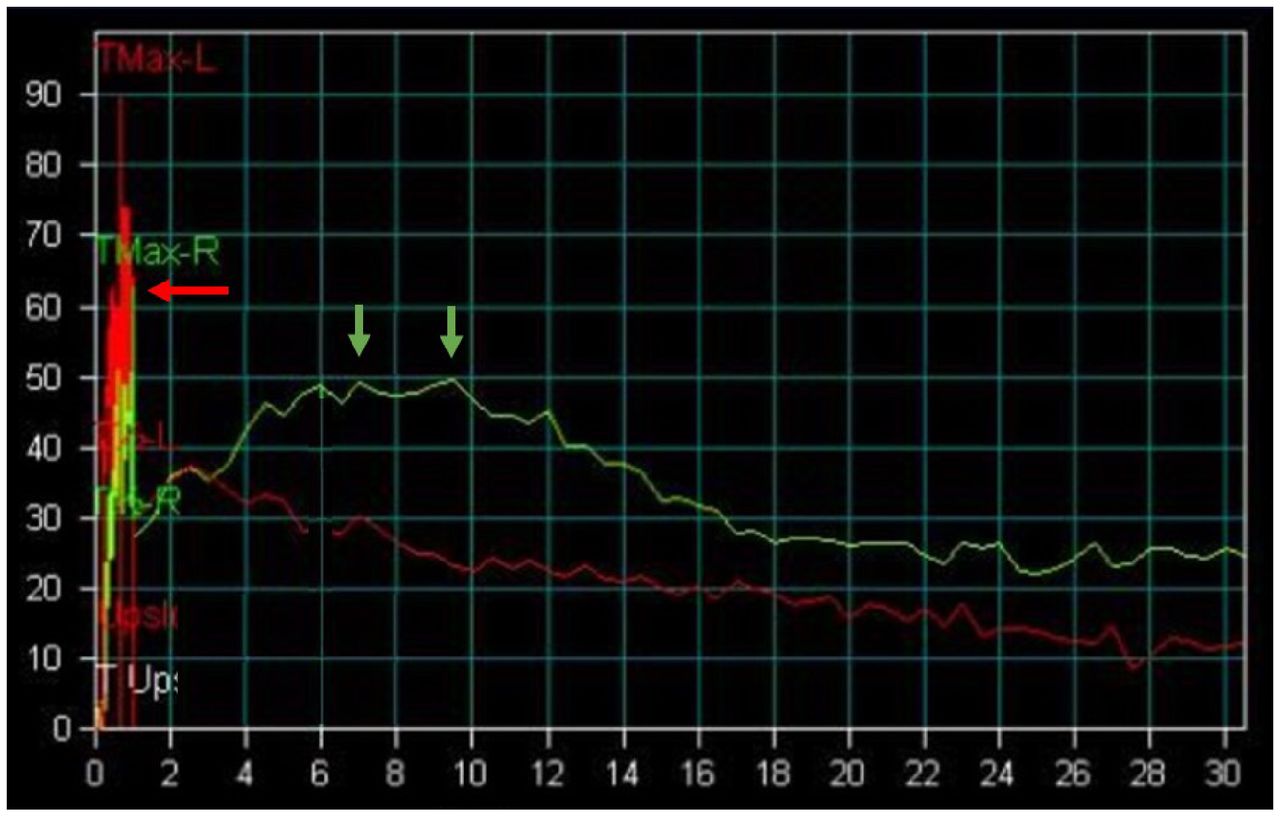
Extensive motion artifact involving first minute of time–activity curve representing flow phase acquired at 1 s per frame. This results in erroneous elevated value at 1 min due to ROIs overlapping vascular activity in liver and spleen (red arrow). Actual right kidney Tpeak is delayed (>5 min) in 7- to 9-min range (green arrows).
A second marker of parenchymal function is 20-min/max. No more than 35% of the activity should be remaining 20 min after Tpeak, as measured using the cortical ROI (50). A known pitfall is to calculate the value using the time point 20 min after the start of the examination instead of 20 min after Tpeak, leading to a spuriously high value.
T-½ emptying is an assessment of how quickly activity is leaving the CS. It is ideally obtained using the CS ROI but may also be accurately obtained from the WK ROI in the absence of significant parenchymal dysfunction. There is wide agreement that a value of no more than 10–15 min excludes obstruction (51). That said, a prolonged T-½ emptying is not diagnostic of obstruction given the other factors that may negatively impact this value (dehydration, poor renal function, severe hydronephrosis, and the presence of significant backpressure from a full or noncompliant bladder).
Additional Measures
In addition to the values discussed above, some supplementary values are recommended by the guidance documents of the SNMMI–EANM and International Scientific Committee of Radionuclides in Nephrourology for a more robust DRS interpretation (10,44). However, these values were assessed using specific protocols for the timing of the diuretic injection in relation to radiopharmaceutical administration. Thus, they cannot be universally applied to all approaches.
Postvoid kidney-to-maximum count is a simple ratio that incorporates gravity into the emptying assessment and provides valuable information. After the acquisition, the patient stands, walks, and then voids. Then, typically at 30 min after administration of the radiopharmaceutical, a supine 1-min postvoid image is acquired, and the postvoid counts in the WK or CS ROI of the kidney of concern are divided by the maximum counts normalized for time (50). In a study of 18 variables by Bao et al. at Emory, this value was most helpful for excluding obstruction (46).
Tissue transit time (also called parenchymal transit time) is based on the fact that urine outflow obstruction negatively affects the function of the nephrons (obstructive nephropathy). This impairment of nephron function results in slow transit of the radiotracer through the tissue. Although a prolonged tissue transit time is not specific for obstruction, it increases the likelihood that obstruction is present (10). The simplest method for determining tissue transit time is visual assessment based on the appearance of activity in the CS, which should occur within 5 min of the radiopharmaceutical injection. Appearance at 8 min or more is considered delayed (52,53).
Output Efficiency and Normalized Residual Activity
Even with these parameters, diseased kidneys with a suboptimal response to diuretics are still a diagnostic challenge, because the shape of the parenchymal phase influences the shape of the CS-emptying phase of the time–activity curve.
Output efficiency was developed as a metric to help overcome the negative effect that impaired renal function has on the perceived CS drainage. Output efficiency allows for an evaluation of the amount of activity remaining in the kidney as a percentage of what entered the kidney and is derived using the integral of the heart activity curve. A value of at least 82% has been shown as normal in a study of healthy individuals, though results are protocol-specific (18,54).
Given the relative complexity of determining the output efficiency and the need for specific processing software, a more simplified approach was developed with normalized residual activity. Normalized residual activity is simply a measurement of the renal activity at a given 1-min interval divided by the renal activity at 1–2 min after radiopharmaceutical injection (55). A value of less than 1.0 when comparing the 1- to 2-min interval with the 20- to 21-min interval or a value of less than 0.10 when using the 1-min interval acquired after voiding at 60 min from the examination start represents good renal drainage (56). Unfortunately, this technique lacks standardization and appears to be influenced more by renal function and background selection than by output efficiency. It also necessitates an accurate assessment of when the radiopharmaceutical reaches the kidneys (57).
Despite their diagnostic utility, output efficiency and normalized residual activity have not yet entered routine clinical practice. Neither variable appeared in the 174 adult DRS reports reviewed in a survey of IAC-accredited facilities (24).
CONCLUSION
DRS plays a critical diagnostic role by providing a physiologic means for differentiating between obstructive and nonobstructive hydronephrosis and by assessing the function of the affected kidney. The examination accuracy is highly dependent on and benefits from close attention to patient preparation, timing of diuretic, method of acquisition, processing, quantification, and interpretation criteria. Until standardized guidelines exist, it is critical for facilities to ensure application of a consistent high-quality approach that best meets the diagnostic needs of the referring providers and allows for accurate follow-up and comparison of results.
DISCLOSURE
Mary Beth Farrell is an employee of the IAC. No other potential conflict of interest relevant to this article was reported.
Footnotes
CE credit: For CE credit, you can access the test for this article, as well as additional JNMT CE tests, online at https://www.snmmilearningcenter.org. Complete the test online no later than December 2025. Your online test will be scored immediately. You may make 3 attempts to pass the test and must answer 80% of the questions correctly to receive 1.0 CEH (Continuing Education Hour) credit. SNMMI members will have their CEH credit added to their VOICE transcript automatically; nonmembers will be able to print out a CE certificate upon successfully completing the test. The online test is free to SNMMI members; nonmembers must pay $15.00 by credit card when logging onto the website to take the test.
Published online May. 24, 2022.
REFERENCES
- Received for publication January 12, 2022.
- Revision received May 10, 2022.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}