


Abstract
A sentinel event is any unexpected event that results in death or serious physical or psychologic injury to a patient unrelated to a patient’s illness. Establishing and determining cause-and-effect relationships are key to preventing future sentinel or near-miss events. However, it can be challenging to establish a cause-and-effect relationship when a process involves multiple steps or people. Root cause analysis (RCA) is a technique that can pinpoint the causes of sentinel events for medical procedures involving numerous steps and people. This article provides a rationale for RCA and the basic steps in a nonmedical RCA investigation. The article then describes a more detailed, 9-step, RCA approach for investigating sentinel events and illustrates the technique with a nuclear medicine example.
A sentinel event is any unexpected event that results in death or serious physical or psychologic injury to a patient unrelated to a patient’s illness (1). In contrast, near-miss events are errors occurring during medical care that are detected and corrected before a patient is harmed. Health-care providers must be aware of and scrutinize both event types critically to improve the safety and quality of care.
When investigating sentinel events and near misses, one must first identify the cause—or why something happened—and the effect of what happened. Establishing and determining cause-and-effect relationships are key to preventing future sentinel or near-miss events.
Determining the cause and the effect is usually straightforward for simple processes involving only one step or person. However, it is difficult to establish a cause-and-effect relationship when a process involves multiple steps or people. Root cause analysis (RCA) is a technique that can pinpoint the causes of sentinel or near-miss events for processes involving multiple steps and people.
FACTORS GIVING RISE TO THE NEED FOR RCA IN HEALTH CARE
The United States’ current, multifaceted health-care system has led to increased attention on sentinel and near-miss events and the need for providers to be familiar with how to perform a systematic RCA. When the causes of events are identified, problems can be addressed and health-care quality improved.
Need for Efficiency
First, the demand for scarce health-care financial resources in the United States is at critical levels (2). One reason is that life expectancy has increased from 70.1 y in 1960 to 76 in 2021 (3,4). Meanwhile, the percentage of gross domestic product spent on health care has increased from $247 billion (9.4% of the U.S. gross domestic product) in 1980 to around $4 trillion (18% of the U.S. gross domestic product) in 2020 (5). Thus, health-care spending has increased considerably, with only a modest increase in life expectancy. This finding points to the need for increased efficiency.
Medical Error Prevention
One strategy to increase efficiency is to decrease cost and waste. Medical errors are one of the leading causes of not only waste and increased cost but also morbidity and mortality. Original estimates in 2000 published in the Institute of Medicine’s landmark report, To Err Is Human: Building a Safer Health System, pegged annual deaths related to medical errors at 98,000 (6). Today that number is estimated to be over 200,000 (7). In response to the unacceptable number of medical errors, the Joint Commission adopted the time-out, or call-to-order, concept in 2003 to curb the rising number of medical errors.
A time-out is an immediate pause by every surgical team member before any medical intervention or procedure to verify the correctness of the patient, procedure, and site (8). The initial time-out process evolved and expanded to become a review of detailed checklists—a concept borrowed from the airline industry, the industry with the best safety record. The checklist model was further popularized in health care by Atul Gawande (9).
Time-outs and checklists have become standard practice. However, the number of sentinel events did not significantly change between 2005 and 2016 (1,10). In 2021, the Joint Commission registered 1,197 sentinel events (11). Although time-outs and checklists play a significant role in preventing medical errors, their weakness is that they cannot address a sentinel event or medical error after it happens.
Teamwork Care Delivery Model
Another factor supporting the need for RCA is the substantial change in how health care is delivered. In the past, solo or small groups were the typical practice model. However, solo practices decreased from 41% to 17% between 1983 and 2014 (12). Large medical groups and hospital conglomerations are now the norm. As a result, health care has become more team-based.
To become more efficient, health care unwittingly adopted the team-based assembly line approach of the auto industry popularized by Henry Ford in the early 1900s (13). The assembly line approach subdivides processes into multiple sequential tasks involving numerous people. Many steps are simple. However, a few steps are always more complex.
For example, in the nuclear medicine scenario, tasks are divided into scheduling, patient preparation, scan performance, interpretation, transcription, and coding and billing. With various personnel completing each task, the physician’s time is spent interpreting images and making diagnoses (more complex tasks), whereas the other steps are distributed among schedulers, nurse navigators, technologists, transcriptionists, or coders (less complex tasks).
Another feature of the assembly line approach is that it matches task complexity to the skills and pay of the staff on the team (13). The more complex the task, the higher the wage. With only a fraction of the tasks paid at the higher rate and most tasks paid at the lower rate, overall payroll costs are reduced. However, the distribution of work into multiple steps performed by various people increases the risk of errors.
ORIGIN OF RCA AND THE 5 WHYS
Sakichi Toyoda, a Japanese inventor and industrialist, recognized the trade-off between the distribution of labor in the assembly line approach and mistakes. He developed the “5-whys analysis” to determine and eliminate the root causes of problems in the Toyota Motors manufacturing process (14).
The 5 whys is a simple problem-solving method for quickly getting to the root of a problem (15). The technique starts by identifying a problem and then asking “why?” 5 times sequentially to drill down and determine what caused a problem. Each time a why is questioned, the answer becomes the premise for the next why question. The technique forces the investigator to dig more deeply to find a problem’s true cause.
To demonstrate, consider an example of administration of a bone scan dose to the wrong patient:
Why did the patient receive the wrong radiopharmaceutical? Because the technologist escorted the wrong patient from the waiting room.
Why was it the wrong patient? Because 2 patients with the same last name but scheduled for different tests were in the waiting room.
Why did the wrong patient come forward? Because the technologist only called out “Mr. Smith” in the waiting room.
Why did the technologist not realize it was the wrong Mr. Smith? Because the technologist did not use 2 patient-specific forms of identification.
Why did the technologist not use 2 forms of patient identification to identify the correct patient? Because use of 2 patient-specific identifiers was not standard practice at the clinic.
When asking and answering the 5 whys, one must obtain clear and concise answers, avoiding answers that are too simple or that overlook important details. The answers to the questions should be logical and backed by proof. One should look for patterns and not just at the isolated event, look for causes for which practical recommendations can be recommended, and ask why—multiple times—to identify the cause and not just the symptoms of a problem. Problems will usually resurface if only the symptoms are treated and the root cause is not identified and corrected.
For example, suppose a patient with chest pain were to go to the doctor to get a prescription to make the chest pain go away. If the doctor merely gives the patient nitroglycerin to make the chest pain go away, the chest pain would probably return and worsen. However, suppose the doctor were to ask why the patient has chest pain and investigate further. In that case, the doctor could diagnose a coronary artery blockage and fix the root of the problem with a stent or bypass.
BASIC RCA STEPS
RCA is a useful technique for pinpointing the cause of safety events. The term event is used here to refer to sentinel or near-miss events. To prevent similar recurrences, RCA discovers why, what, and how something happened (16).
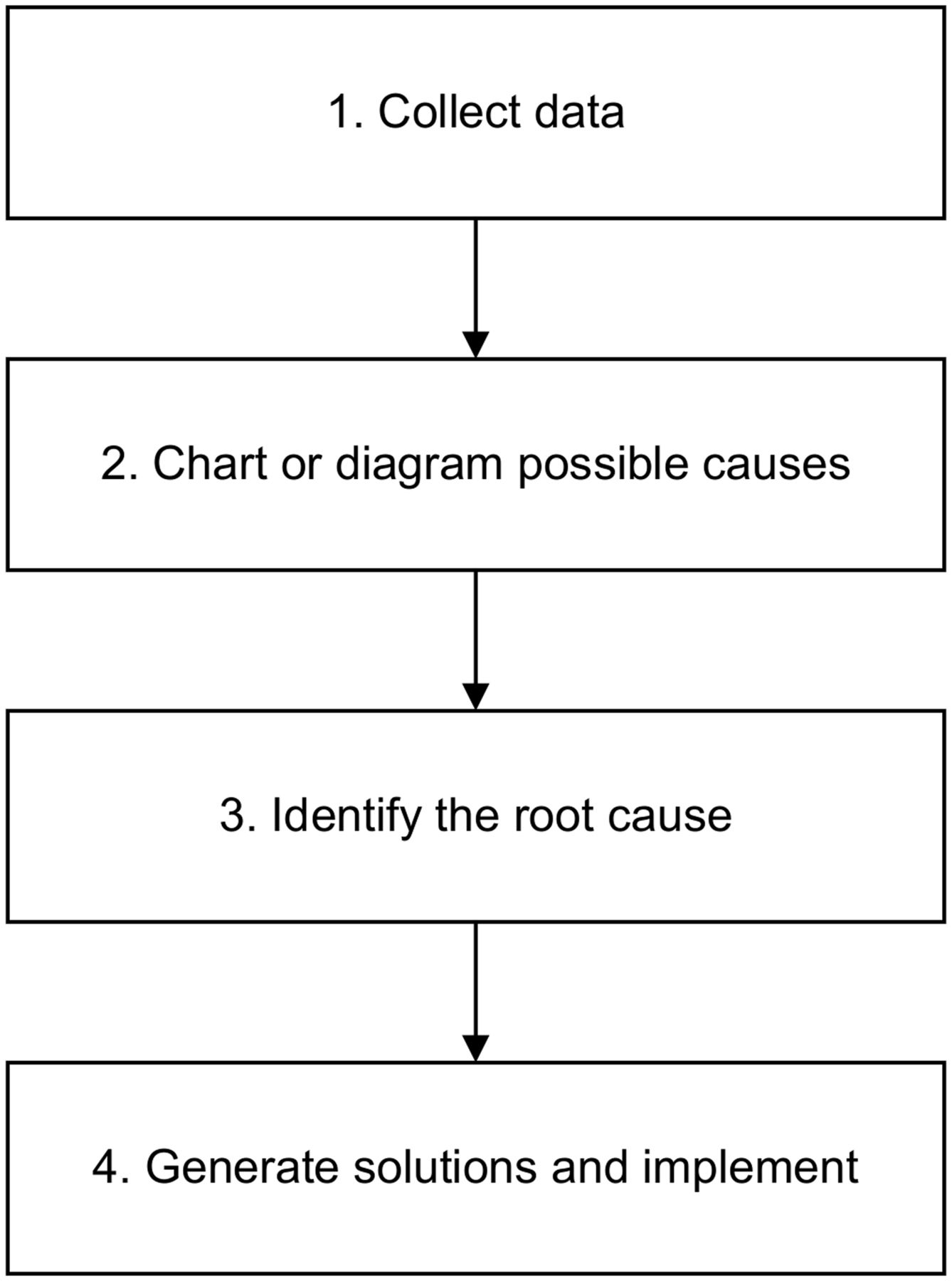
There are 4 primary steps in the RCA process (Fig. 1). The first is to collect data. Data collection is critical for obtaining complete information, understanding the event, and identifying causal factors. Diagraming, the second step, helps to organize and analyze information and to identify knowledge gaps. After the causal factors have been identified, the third step is pinpointing the root cause. Finally, the fourth step is generating and implementing a solution. The solution should be achievable and aimed at preventing the event’s recurrence.
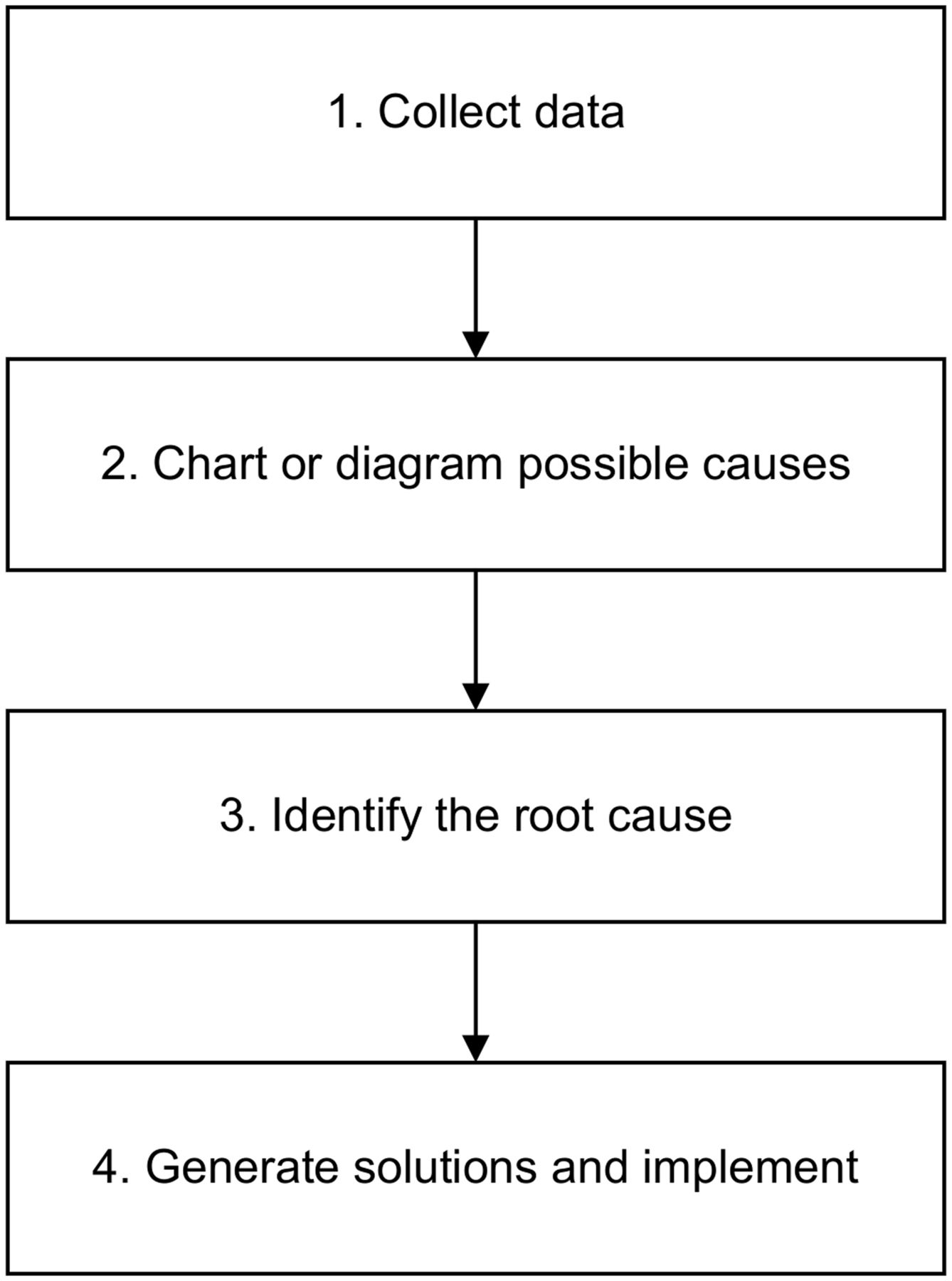
At its simplest, basic RCA involves 4 steps.
APPLYING RCA TO SENTINEL EVENTS
Use of RCA to examine sentinel events, in which a patient could be harmed or die needlessly, must be systematic and comprehensive. The analysis should focus on systems and processes and not just the human element of error. Nine steps are recommended (Fig. 2) (17).
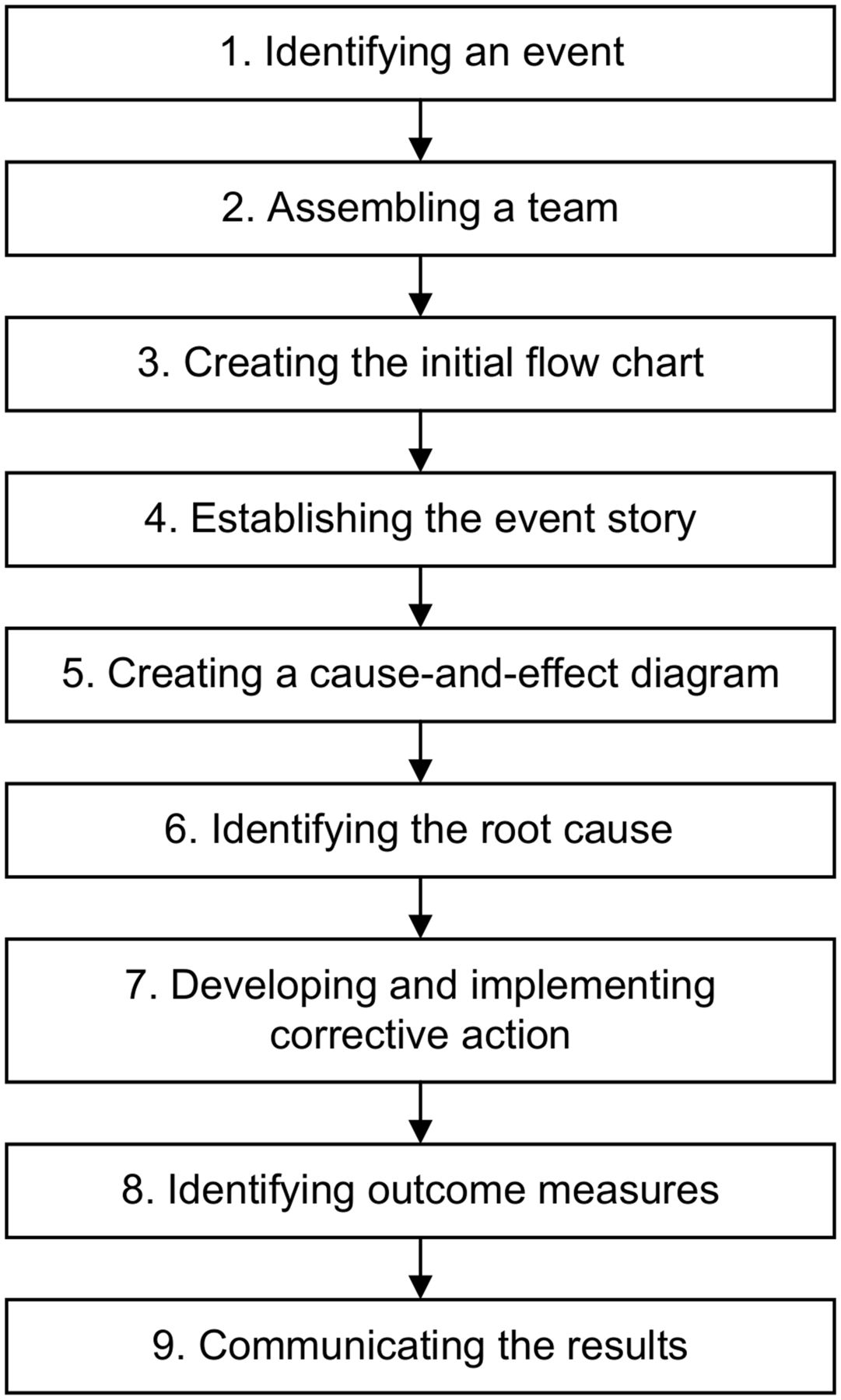
Because sentinel events happen in health-care settings involving multiple people and steps, RCA process is more involved than basic RCA.
Step 1: Identifying an Event
The Joint Commission clearly defines and provides a long list of what is and is not considered a sentinel event (18). Common examples of sentinel events include falls, unintended retention of foreign objects, suicide, wrong surgery, and treatment delay. All staff should be trained to recognize sentinel events or close-call incidents and report them within the system. Usually, a risk-based triage system or committee is used to evaluate the incident and determine the need for RCA.
A fundamental principle of RCA is honest reporting without fear of reprisal. Regrettably, fear of retaliation can be a significant barrier that inhibits staff reporting of incidents. Besides the candid reporting of events, reporting must be prompt (without delay) to ensure that details are thoroughly and accurately documented (17).
Step 2: Assembling a Team
Once the need for RCA is established, a small team is assembled to analyze the incident. First, the team collects preliminary data to understand what the event was, where it happened, when it happened, who was involved, and how it happened.
Teams are usually made up of 4–6 individuals experienced in the field and conversant with the nuances of the process leading to the sentinel or near-miss event. Typically, teams include physicians, supervisors, staff, and quality improvement experts. The team members who perform an RCA investigation should not have been directly involved in the event, as bias can be an undesirable source of problems and inaccurate analysis.
Step 3: Creating an Initial Flowchart
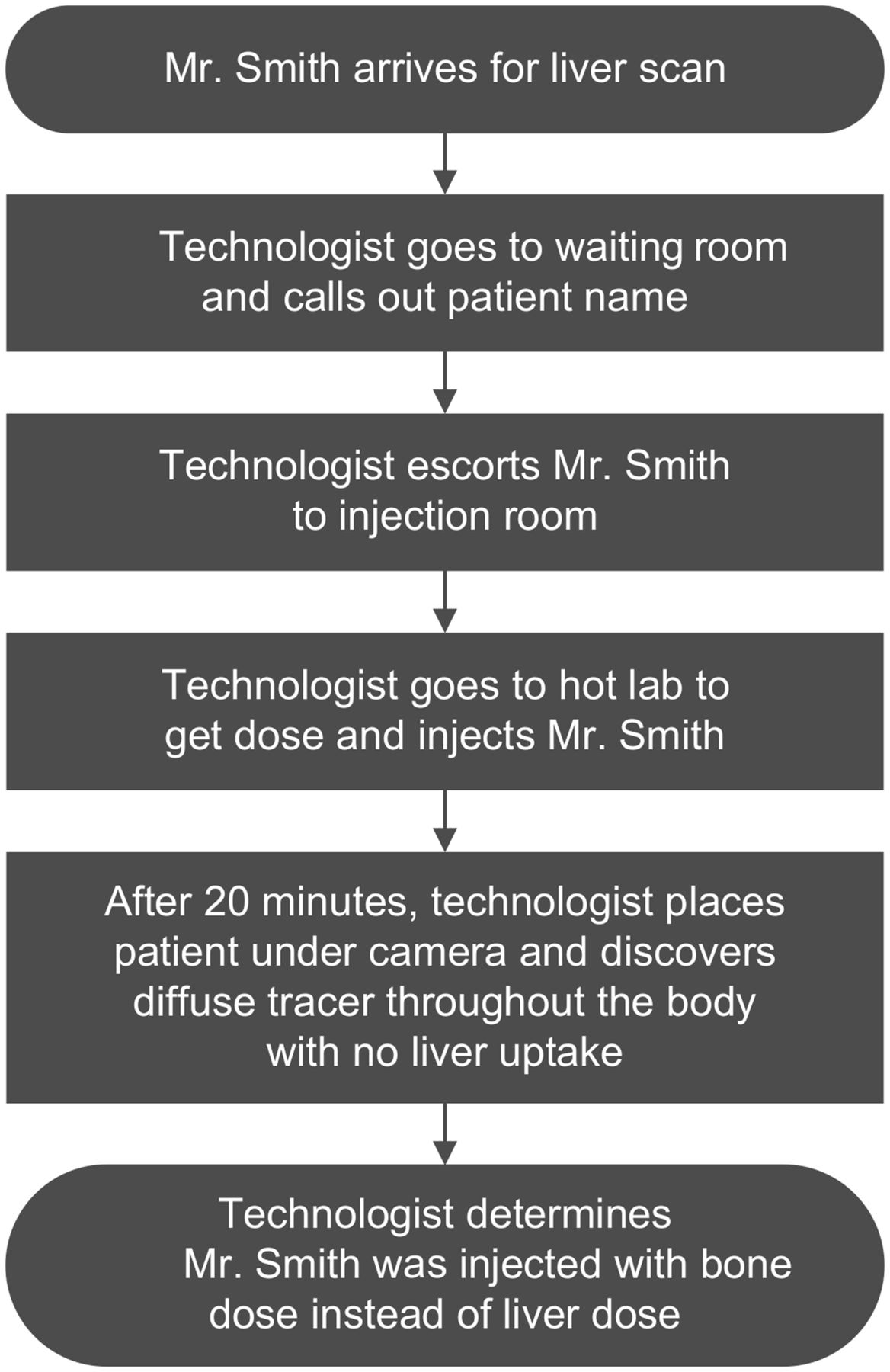
Flowcharts are one of the best tools to describe a process or event graphically, in a manner that usually can be better understood than an essay description. Using the preliminary data, the team creates a flowchart to display the processes leading to the event and organize the facts (Fig. 3).
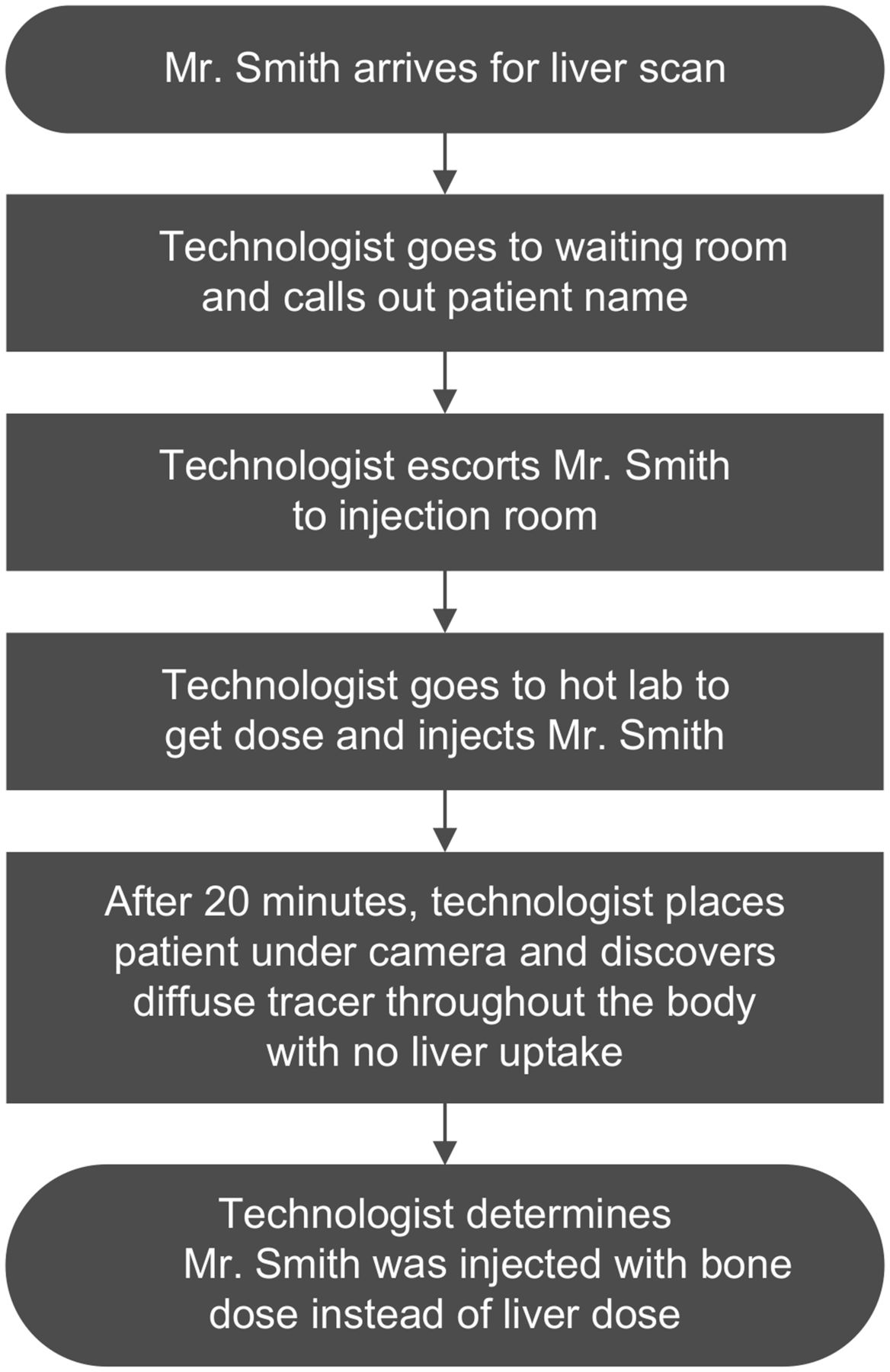
Initial flowchart for misadministration demonstrates facts surrounding situation in which technologist administered bone scan dose instead of liver scan dose.
Step 4: Establishing the Event Story
The flowchart should trigger questions to guide the investigation into contributing factors. The 5-whys technique is used at this point. The goal is not only to assess the sentinel event but also to thoroughly evaluate the processes leading to the event. Therefore, fine granularity is essential in pinpointing the root cause or causes. The information gathered from the investigation adds detail to the initial flowchart for development of the event story map.
Step 5: Creating a Cause-and-Effect Diagram
Once the event story map is generated, the next step is to produce a cause-and-effect diagram. A cause-and-effect diagram is another visual tool to logically organize potential causes of a problem (effect). The diagram’s purpose is to help the investigating team identify causal links and contributing factors to the root cause.
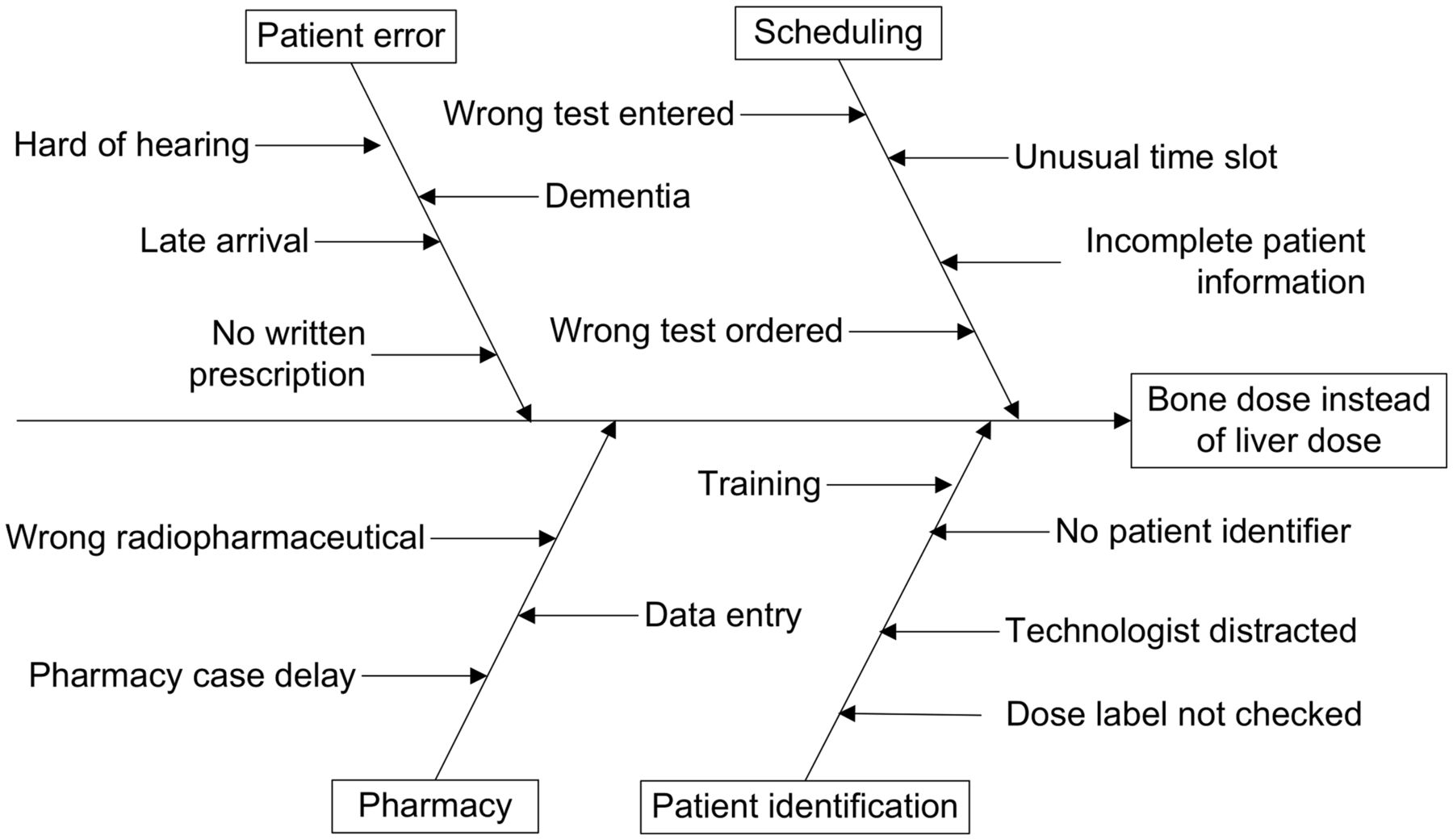
The components of a cause-and-effect diagram include a problem statement, potential causes (categories), and potential reasons for the causes. Using the same example of administering the wrong radiopharmaceutical to the patient (effect), there could be multiple causes related to scheduling, patient identification, pharmacy error, or patient factors (Fig. 4).
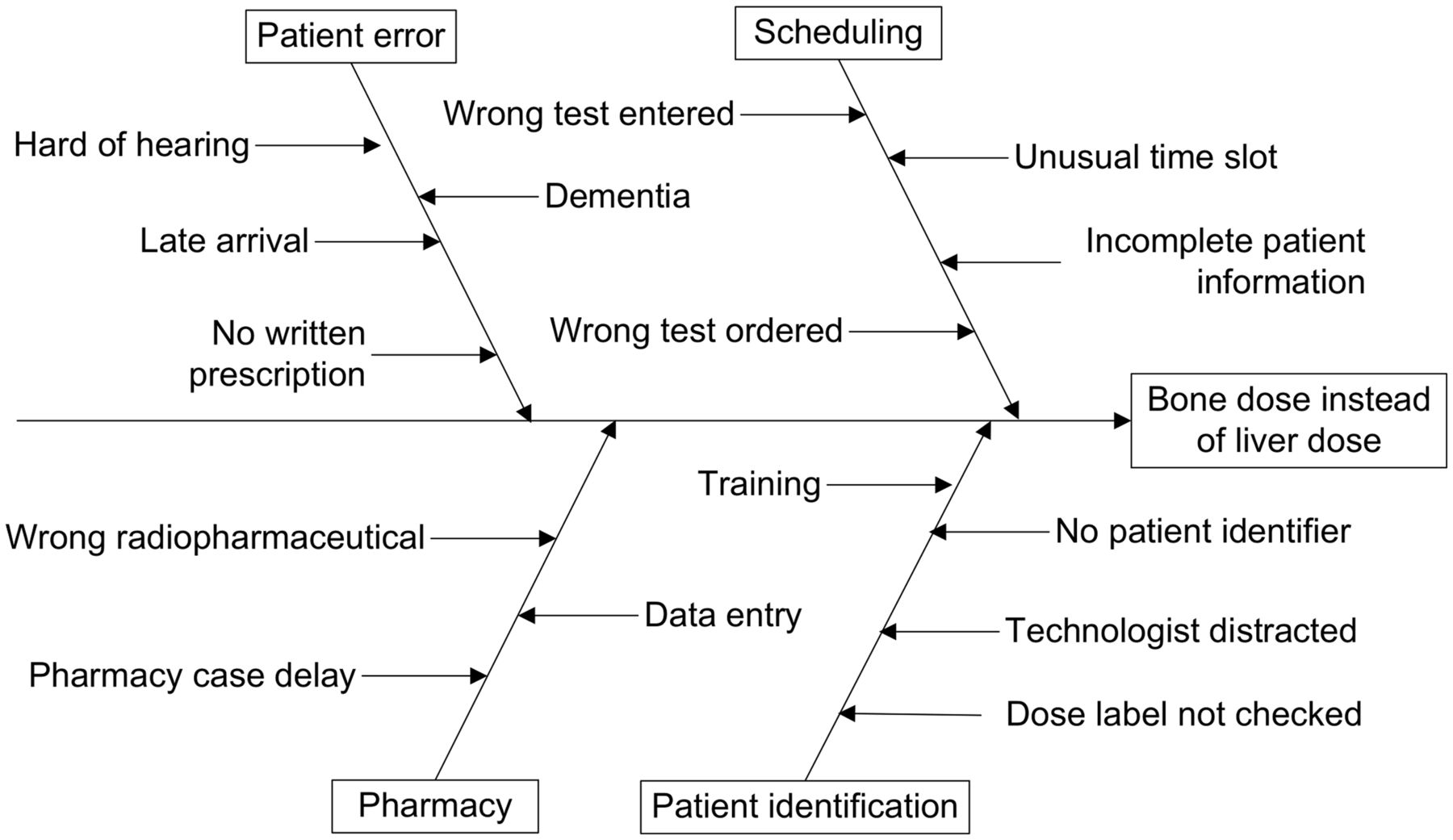
Effect and potential causes of misadministration of bone dose instead of liver dose are demonstrated in this fishbone diagram. Each probable cause has multiple reasons or contributing factors.
It is helpful to place the flowchart and event story map side by side when identifying causes. Potential causes are then repeatedly identified until knowledge of the event is exhausted. If few causes are identified, additional investigation is required.
Step 6: Identifying the Root Cause
The cause-and-effect diagram will show multiple causes for, steps to, or reasons that led to the event. It is crucial to single out the one cause of the cascade of failed steps that led to the event. Each cause is examined and discussed along with the contributing factors until a root cause is identified.
Step 7: Developing and Implementing Corrective Actions
The identified root cause is then examined again to develop corrective actions. The team should identify barriers and risk reduction strategies to ensure that the root cause does not recur. Multiple corrective steps may be required for each cause. Planning of the corrective action should include policy changes, training, and other steps to ensure and sustain compliance. In addition, the planning must eliminate implementation barriers and identify outcome measures. The corrective actions are then implemented.
Step 8: Identifying Outcome Measures
The success of any intervention or change implementation can be measured only by outcome analysis. The outcome metrics should be specific, quantifiable, and able to be measured over time. The time required for accurate outcome analysis depends on how frequently the procedure or process in question is done. The more frequently a procedure is performed, the shorter the period of outcome analysis.
Step 9: Communicating Results
The last step is communication of the results. The event, RCA, corrective actions, and outcome results should be reported to all staff involved and, more broadly, throughout the institution. If deemed important and not institution-specific, reporting an RCA in a peer-reviewed publication can have a more significant positive impact.
SPECIAL CIRCUMSTANCES FOR RCA IN NUCLEAR MEDICINE
The nuclear medicine and molecular imaging field is diverse, comprising nearly 100 diagnostic examinations and a rapidly increasing number of theranostic procedures (19). Numerous procedures require several staff members or the assistance of personnel from outside the department, such as personnel from cardiology, endocrinology, or oncology. In theranostic procedures, opportunities for variability are multiplied, with the added burden of risk of harm. This diverse number of procedures with multiple steps and various personnel presents many different opportunities for error (Tables 1 and 2).
Opportunities for Error in Diagnostic Nuclear Medicine
Opportunities for Error in Therapeutic Nuclear Medicine
NUCLEAR MEDICINE RCA EXAMPLE
Let us apply the RCA process to a potential nuclear medicine sentinel event (a patient falls off the scan table) to make the RCA steps more understandable and meaningful. Was the technologist just careless?
Step 1: Identifying an Event
On August 26, 2022, an elderly patient, Mrs. Darling, underwent whole-body bone scanning and fell off the table while unattended. The incident happened at approximately 12:30 pm. Technologist Ray Gamma started the acquisition and left the room. About 15 min later, he found Mrs. Darling on the floor, moaning and complaining of hip pain. Technologist Gamma immediately reported the event to his nuclear medicine supervisor, who completed the incident form and notified the risk management department. Subsequent radiography and examination found that Mrs. Darling had a broken right hip. The risk management director, Dr. Guardian, determined that the harm was not related to the patient’s illness or the procedure. The harm was thus classified as a sentinel event.
Step 2: Assembling a Team
Dr. Guardian appointed an RCA team to investigate the event. The team included Dr. Roentgen, a staff nuclear medicine physician vacationing in Florida on the day of the event; the radiology department nurse, Nurse Ivy Line; the nuclear medicine scheduler, Ms. Ida Arrangér; a nuclear medicine technologist who works at a satellite office, Mr. Pho Ton; and one of the risk managers who is an expert in RCA, Nurse Al Waysmad.
Step 3: Creating an Initial Flowchart
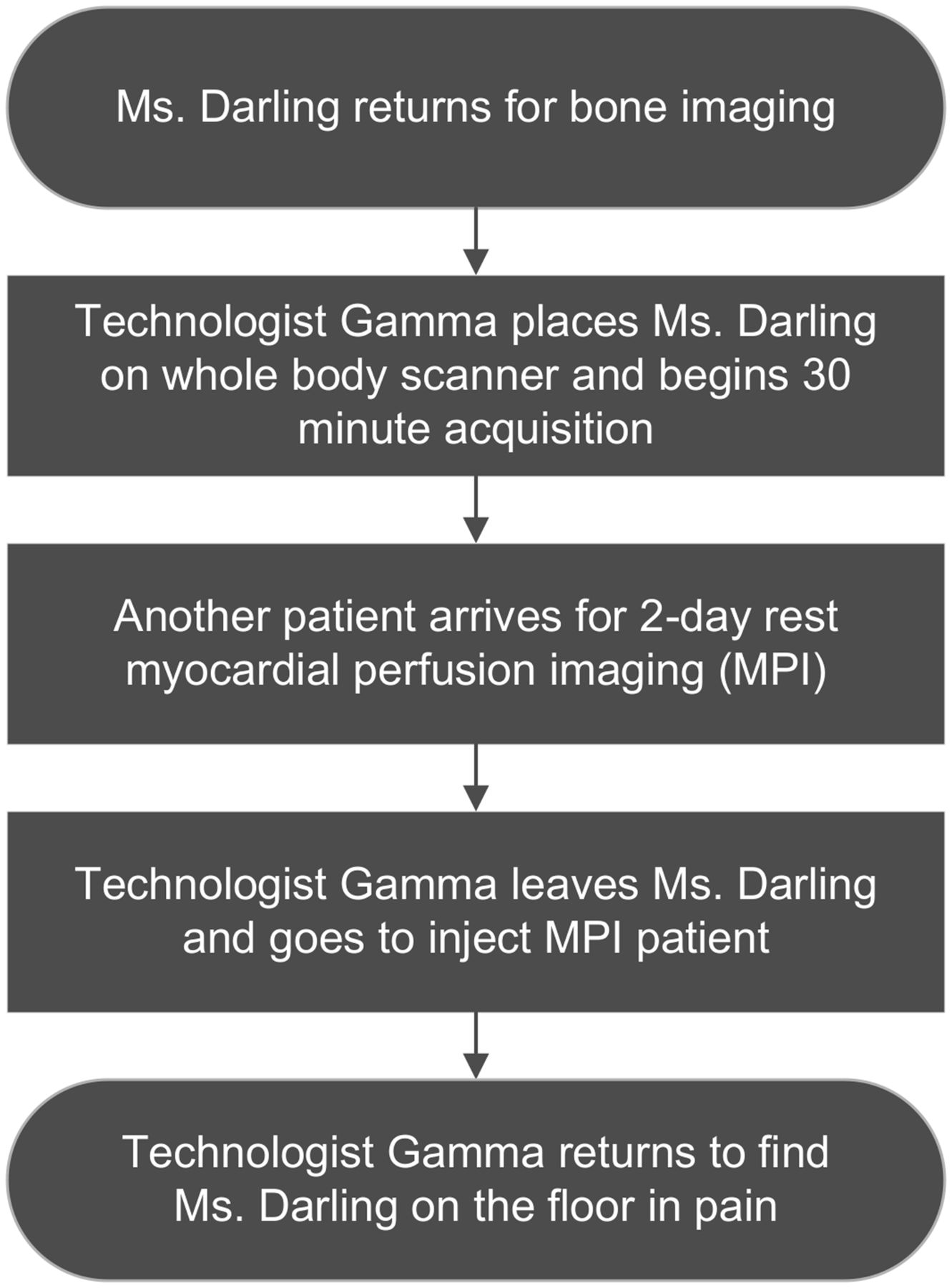
The team created a simple flowchart to organize the preliminary facts and began the investigation (Fig. 5)
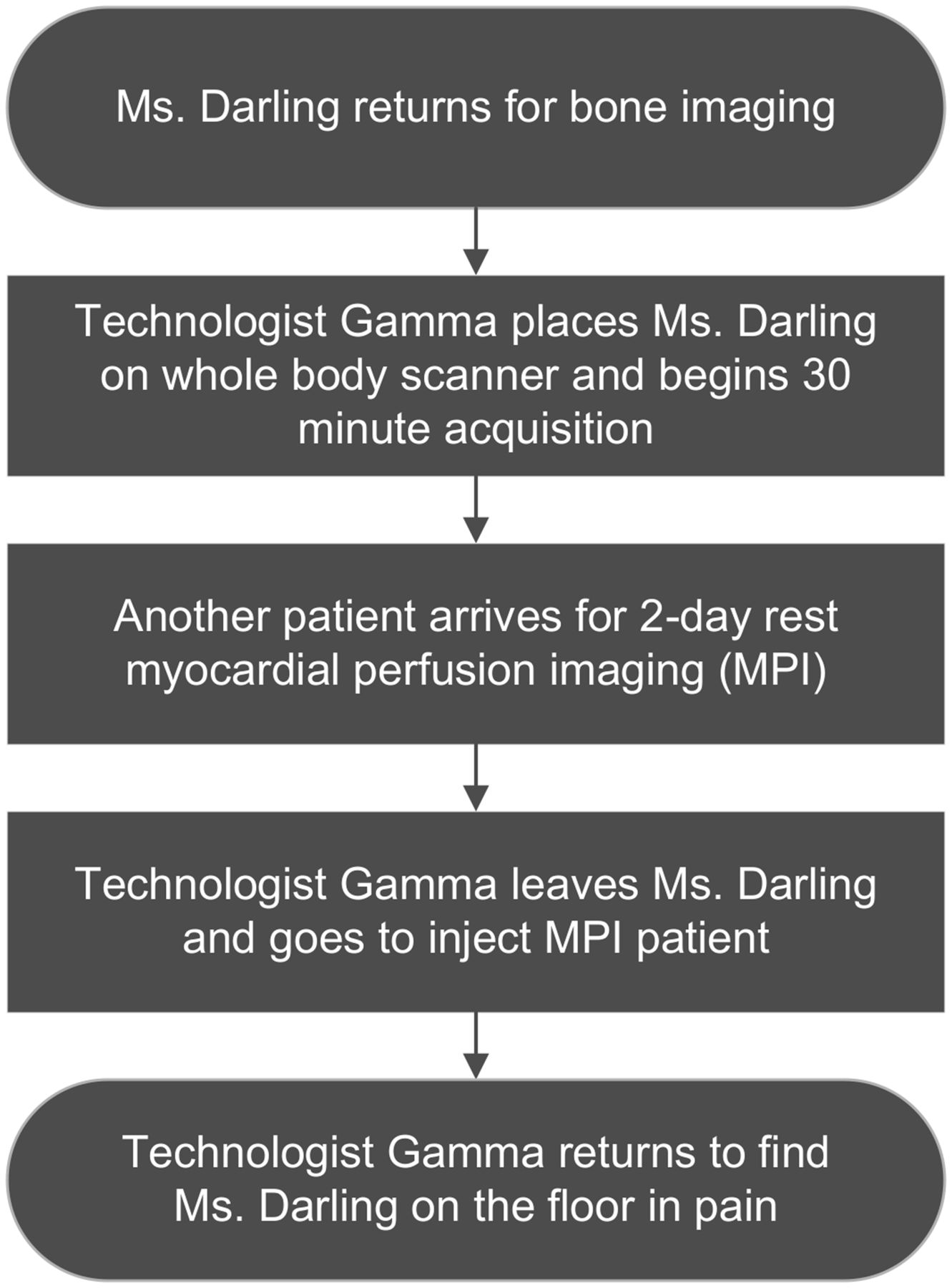
Initial flowchart for patient’s falling off scanner table describes facts related to this sentinel event. These facts are used to stimulate questions for investigation and to create event story.
Step 4: Establishing the Event Story
Using the 5 whys, the team asked questions and interviewed other staff, such as the receptionist, lead technologist, and other technologists. The team asked questions such as why did Technologist Gamma leave the patient unattended? Why did not another staff member inject the patient who was to undergo rest myocardial perfusion imaging (See Fig. 5)? Could Technologist Gamma maintain visual surveillance of the patient? What was the patient’s mental acuity? Did Technologist Gamma tell Mrs. Darling he was leaving the room? Why did Mrs. Darling fall off the table?
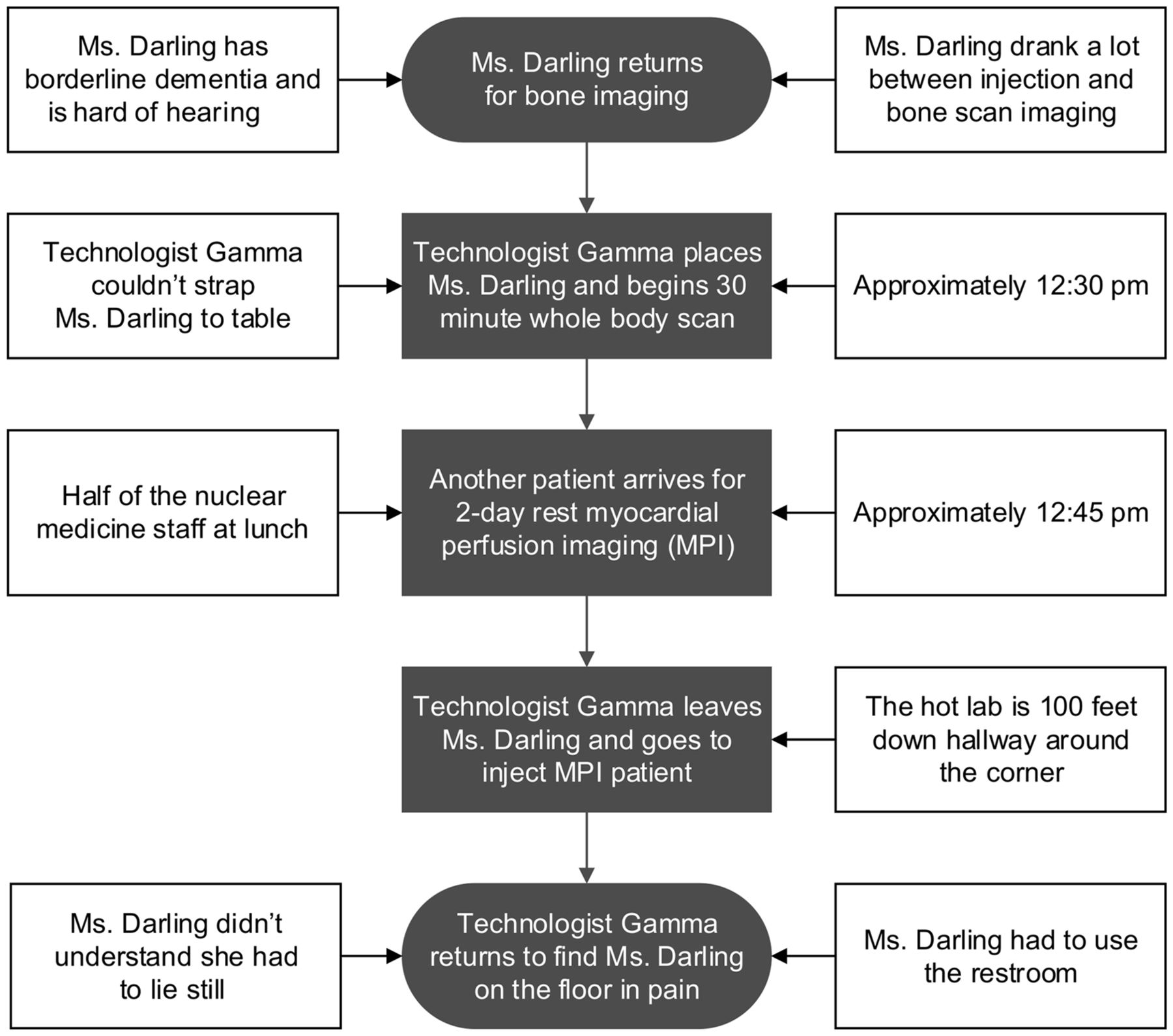
During the investigation, the team discovered several contributing factors. First, between the bone scan injection and the image acquisition, Mrs. Darling was told to drink 1.9 L (64 oz) of water. Second, Mrs. Darling did not empty her bladder right before the scan began because the restroom, located outside the department, was occupied. Third, Mrs. Darling had mild dementia and was hard of hearing. Fourth, half the technologists were at lunch when the myocardial perfusion patient was scheduled for injection; there were no other technologists available to inject the patient. Fifth, the hook-and-loop straps on the table were worn and would not fasten well. Finally, Mrs. Darling was uncomfortable and had to use the restroom. These factors and several others contributed to the patient’s fall (Fig. 6).

Event story flowchart adds factors contributing to patient-fall sentinel event, as determined during RCA.
Step 5: Creating a Cause-and-Effect Diagram
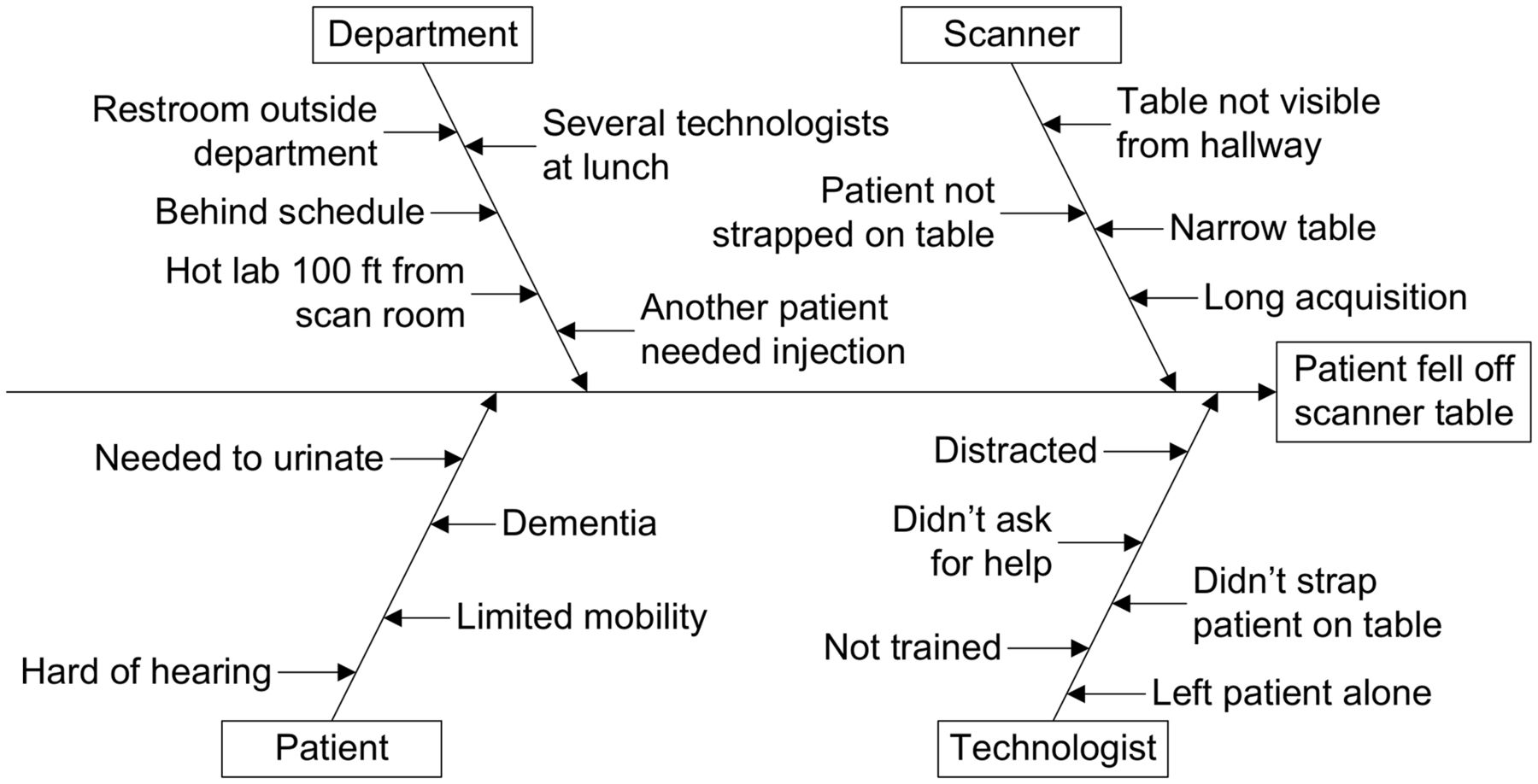
The team organized all the discovered factors to create the cause-and-effect diagram (Fig. 7). The problem (effect) was that the patient fell off the scan table. The major causal factors were related to the patient, department operation, equipment, and technologist. There were also multiple underlying reasons for each of the major causal factors.
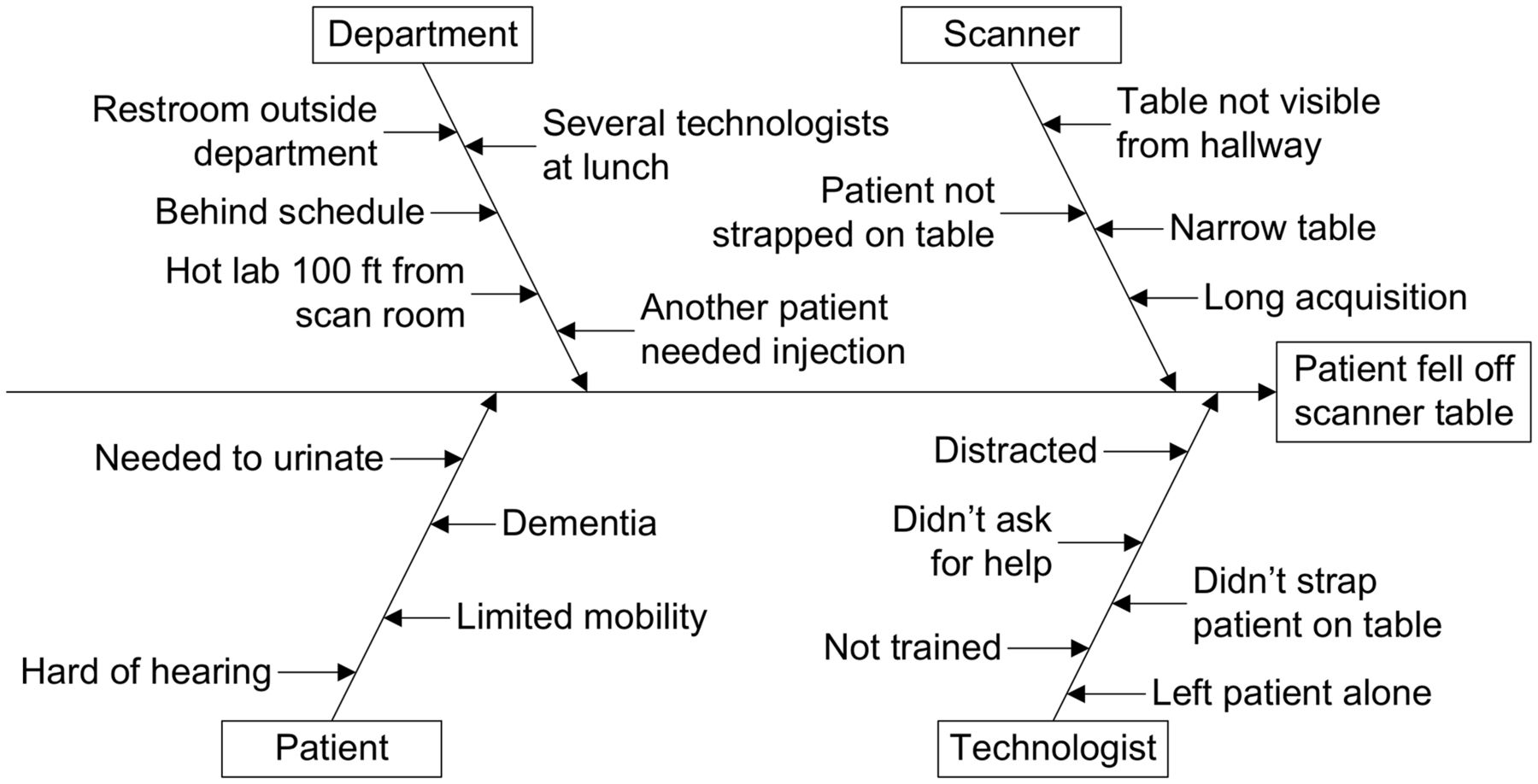
Effect and potential causes of, and contributing factors to, patient’s falling off scanner table are demonstrated in this fishbone diagram.
Step 6: Identifying the Root Cause
The team evaluated the fishbone diagram related to Mrs. Darling’s fall and identified the root cause. The department was short-staffed during lunch, but patients were routinely scheduled during that time, resulting in technologists caring for multiple patients simultaneously. Technologist Gamma believed he had no choice but to leave Mrs. Darling and inject the myocardial perfusion patient because no other technologists were available and the department was running behind schedule. Contributing factors were the nature of bone scan hydration requirements, lack of an available restroom near the nuclear medicine department, malfunctioning table straps, and the patient’s need for continuous monitoring. Although Technologist Gamma could have made other choices, there was more to the story than that he was simply careless.
Step 7: Developing and Implementing Corrective Actions
The team, the nuclear medicine supervisor, and other staff reviewed the cause-and-effect diagram and discussed the root cause. They implemented several changes. First, lunches were staggered over a more extended period so that fewer technologists were simultaneously absent from the department. Second, the schedule was adjusted so that technologists would not be responsible for more than one patient at a time. For example, a technologist would not have to inject one patient while scanning another. Finally, the table straps were replaced as a minor corrective action.
Step 8: Identifying Outcome Measures
To assess the effectiveness of the intervention, the team and nuclear medicine department monitored the number of times technologists had to care for more than one patient at a time. Because numerous procedures were performed daily, the team collected data for 1 mo and then evaluated and made changes as necessary.
Step 9: Communicating Results
To ensure that the corrective actions were implemented and sustained, the nuclear medicine supervisor created a new scheduling grid and shared instructions with the scheduling department. The supervisor also made a lunch schedule, which she posted on the lounge wall and shared during a staff meeting. Finally, the entire nuclear medicine department attended training on caring for patients with varying needs.
LIMITATIONS OF RCA
The limitations of applying the RCA methods of the automobile manufacturing industry to medicine have been well documented (20). Although RCA may be well suited to automobile manufacturing, in which the parts and final product are standardized in the form of model, year, and make of the vehicle, medicine deals with humans without the same model, year, and make. The diverse composition of the patient population and the unique needs of individual patients, including emotional and psychologic, create a situation far more complex than in an automobile assembly line. Consequently, RCA in health care must be more detailed and more involved, as described in the 9 steps for RCA in sentinel event investigation.
Another limitation of RCA is that it must be supported by the top administration and then by all administrative levels downward to improve safety and induce cultural changes (21). There must be a blame-free environment so that individuals feel safe and can be persuaded to talk openly about events. Effective sentinel event communication is key to institutional learning and preventing future events (20).
Finally, RCA can be time-consuming and requires adequately trained personnel. RCA is a complex, multistep process that is operator-dependent. The fact that it is often not properly performed affects the tool’s utility. As a result, there is limited published research demonstrating the effectiveness of RCA in reducing sentinel events and near misses. Thus, to be effective, nuclear medicine personnel, including technologists, must be knowledgeable and skilled in the technique.
CONCLUSION
The reliability and accuracy of nuclear medicine procedures are highly dependent on the competency of the nuclear medicine technologist. Despite a technologist’s training and skill, the complexity of nuclear medicine procedures increases the likelihood of sentinel events and near misses. Therefore, technologists play a pivotal role in RCA performance and the subsequent prevention of future events.
Team members need to know not only their assigned job but also the jobs of those who work in earlier and later steps of the multistep procedure. This knowledge can help to identify and correct errors before a small error snowballs into a catastrophic avalanche.
The technologist team player should not only understand and follow protocols but also understand the principle behind a protocol. Because of the diversity of procedures and of human anatomy and physiology, along with the need for patient-centered care, nuclear medicine technologists must be able to modify protocols without affecting the outcome. The use of RCA in nuclear medicine is an invaluable tool to address the many challenges encountered in the field.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
CE credit: For CE credit, you can access the test for this article, as well as additional JNMT CE tests, online at https://www.snmmilearningcenter.org. Complete the test online no later than December 2025. Your online test will be scored immediately. You may make 3 attempts to pass the test and must answer 80% of the questions correctly to receive 1.0 CEH (Continuing Education Hour) credit. SNMMI members will have their CEH credit added to their VOICE transcript automatically; nonmembers will be able to print out a CE certificate upon successfully completing the test. The online test is free to SNMMI members; nonmembers must pay $15.00 by credit card when logging onto the website to take the test.
Published online Oct. 4, 2022.
REFERENCES
- Received for publication August 28, 2022.
- Revision received September 14, 2022.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}