


RATIONALE/INTRODUCTION
Hydronephrosis can be caused by obstruction or by nonobstructive disorders such as infection, vesicoureteral reflux, or congenital anomalies. Diuretic renal scintigraphy is critical in differentiating between obstructive and nonobstructive hydronephrosis. Under physiologic conditions, urine may pool in the renal pelvis during hydronephrosis because there is an anatomic obstruction or because of the reservoir effect, in which urine remains in the dilated renal pelvis until enough accumulates to spill over into the ureter. During diuretic administration, the resultant high flow condition can overcome the reservoir effect. The presence of obstruction can be assessed by evaluating the washout of radiopharmaceutical from the collecting system and assessing parenchymal function.
INDICATIONS
Evaluation of obstructive renal nephropathy.
Evaluation of hydronephrosis.
Differentiation between obstructive hydronephrosis and nonobstructive collecting system dilation.
CONTRAINDICATIONS/TECHNICAL CONSTRAINTS
Pregnancy/breastfeeding (pregnancy must be excluded in accordance with local institutional policy; if the patient is breastfeeding, appropriate radiation safety instructions should be provided).
A recent nuclear medicine study (radiopharmaceutical-dependent).
Furosemide (contraindicated in anuric or dehydrated patients).
PATIENT PREPARATION/EDUCATION
The patient may eat and take medications as necessary before the study.
The patient should be well hydrated and instructed to increase fluid intake the day before and morning of the study. Thirty minutes to 1 h before the study, the patient should drink an additional 500 mL (16 oz) of water. Children should receive intravenous hydration with a 10- to 15-mL/kg volume of normal saline over 30 min (5% dextrose for patients younger than 1 y).
Diuretics should be discontinued 24 h before the study.
A focused history containing the following elements should be obtained:
Past medical history, including diabetes, hypertension, kidney disease (urinary tract infections, calculi, renal surgery, stents), and autoimmune disease.
Signs and symptoms.
Current medications, especially the chronic use of diuretics.
The results of clinical laboratory tests, including serum creatinine or estimated glomerular filtration rate.
The results of other diagnostic tests, including ultrasonography, MRI, and CT (including contrast administration).
Fluid input and output.
RADIOPHARMACEUTICAL IDENTITY, DOSE, AND ROUTE OF ADMINISTRATION
Table 1 provides the radiopharmaceutical identity, dose, and route of administration.
Radiopharmaceutical Identity, Dose, and Route of Administration
ACQUISITION PARAMETERS: DYNAMIC/STATIC/PLANAR
Table 2 provides the dynamic, static, and planar acquisition parameters
Acquisition Parameters: Dynamic/Static/Planar
ACQUISITION INSTRUCTIONS
Instruct the patient to void immediately before the study to reduce the possibility of patient motion or of the need to terminate the study prematurely. Voiding also minimizes the backpressure effect of a distended bladder, which may slow draining of the upper urinary tracts.
Position the patient supine on the imaging table with the camera in the posterior position, ensuring that the kidneys and bladder are in the field of view.
Administer the radiopharmaceutical intravenously as a bolus, and begin imaging when the activity is about to enter the abdominal aorta.
Acquire immediate blood flow images at 2–4 s/frame for 60–120 s to assess renal arterial flow.
Acquire serial sequential images at 1–2 min/frame for 20–30 min to evaluate parenchymal function and urine outflow from the collecting system.
On the basis of the Santa Fe consensus, have the patient stand and walk around for a few minutes, followed by voiding of the bladder. The furosemide is then administered over 1–2 min by slow intravenous injection at the start of an additional 20-min acquisition at 1–2 min/frame.
Obtain a prevoid and postvoid kidney and bladder 60-s image; an erect postvoid image is optional.
COMMON OPTIONS
If the patient is unable to void, bladder catheterization may be required. Increased bladder pressure may diminish the effect of the diuretic.
PROCESSING INSTRUCTIONS
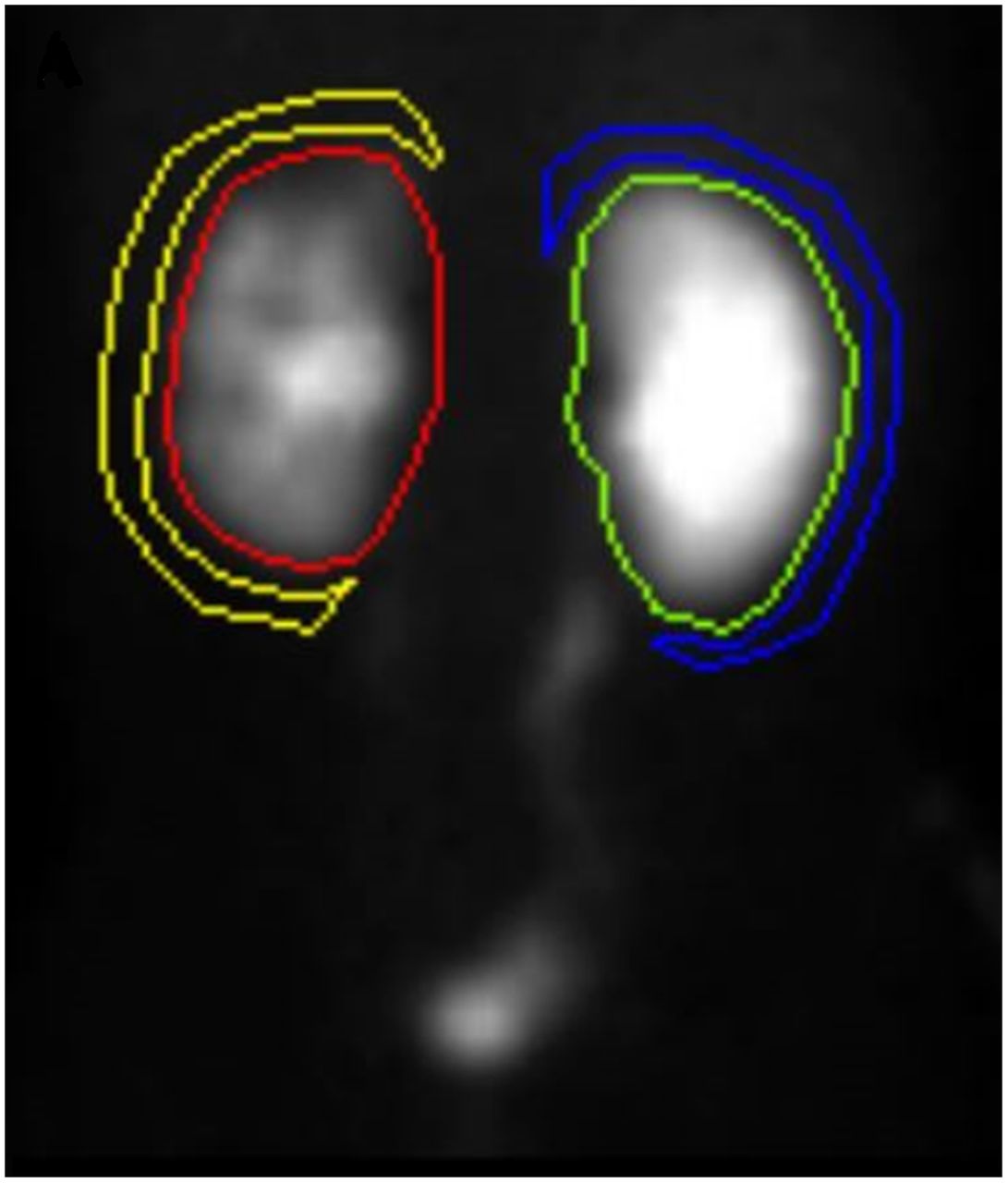
Draw regions of interest around the entire kidney and pelvis. Draw additional C-shaped perirenal background regions 2 pixels thick and 1 pixel away from the whole kidney region (Fig. 1).
Generate time–activity curves.
Calculate the collection system clearance half-time or washout half-time (T½). T½ may be measured from the time the diuretic is given to the time it takes to reach half the original level. Computer quantitative software can more precisely calculate T½ by fitting a curve to the steepest portion of the washout time–activity curve. Normally, a T½ of less than 10 min indicates that no obstruction is present.
Use the automatic software to calculate relative function (if available), which is the percentage of the total function of both kidneys. It is calculated by comparing the area under the curve for both kidneys between the 1- and 3-min intervals. Normal values are between 45% and 55%.
Sum the dynamic images, and display them for optimal visualization of the area of interest.
Scale planar images to accurately visualize areas of normal anatomy and increased uptake.

Whole kidney region of interest with perirenal background region. Yellow = left kidney background; red = left kidney; green = right kidney; blue = right kidney background.
PRECAUTIONS
Caution should be used when furosemide is given to patients who have just undergone urologic surgery, because of the increased urine flow rate.
SUGGESTED READING
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.





{kind=link}