


Abstract
Hepatic splenosis is a rare entity, for which indeterminate liver lesions can pose a clinical dilemma. In difficult cases, scintigraphy can be of great value, especially with novel SPECT/CT and SPECT/MRI techniques.
Splenosis commonly occurs incidentally and locates to bowel surfaces, the parietal peritoneum, the mesentery, and the diaphragm but can potentially occur anywhere in the peritoneal cavity. Patients frequently have a history of splenectomy or trauma. On the other hand, hepatic splenosis is a rare entity and may present clinically. Indeterminate liver lesions can pose a clinical dilemma and may lead to additional investigations, anxiety, follow-up imaging, and even invasive procedures. MRI usually performs extremely well. In difficult cases, scintigraphy can be of great value, especially with novel SPECT/CT and SPECT/MRI techniques. We describe the impact of hybrid imaging in the case of a 29-y-old woman with hepatic splenosis.
CASE REPORT
Our patient presented with epigastric, right-upper-quadrant abdominal pain. She had undergone splenectomy and cholecystectomy 10 y previously because of hereditary spherocytosis. A year earlier, for workup of nephrolithiasis, she had undergone abdominal CT, which demonstrated an incidental hepatic hypodensity that could not be characterized (Fig. 1A). After symptomatic management, the patient was discharged but returned twice in the subsequent weeks because of continued abdominal pain and showed mildly elevated results on liver function tests. Consequently, the patient underwent abdominal ultrasound, which demonstrated a small, hyperechoic lesion within the right lobe of the liver (Fig. 1B). The findings were confirmed by MRI, which demonstrated an indeterminate exophytic mass within segment VI of the liver (Fig. 2).

(A) Single-phase CT scan obtained at different hospital does not demonstrate typical arterial enhancement (arrow). (B) Ultrasound image shows hyperechoic mass (arrow). Mass would typically be hypoechoic.
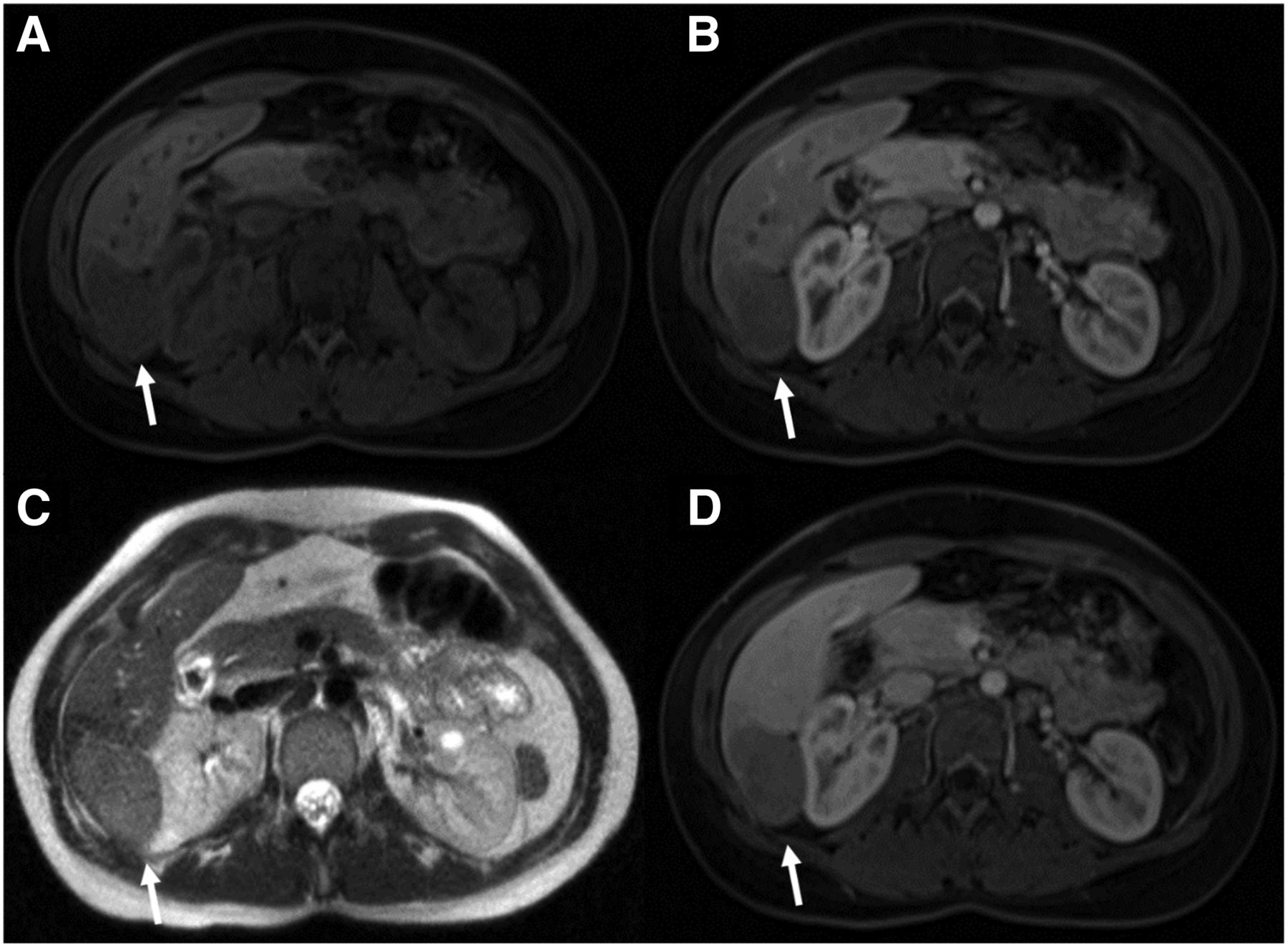
Axial MR images of area of lesion (arrows). (A) T1-weighted fat-saturated volumetric interpolated breath-hold examination (VIBE) sequence shows typical hypointensity. (B) Arterial-phase T1-weighted VIBE sequence shows no uptake of gadoxetate disodium (Eovist; Bayer). (C) T2-weighted sequence shows typical hyperintensity. (D) Portal venous–phase T1-weighted VIBE sequence shows no gadoxetate disodium uptake.
After developing fevers and malaise and experiencing continued pain, the patient was admitted to the hospital, and her blood work showed atypical lymphocytes, elevated levels of lactate dehydrogenase and uric acid, and Epstein–Barr virus serologies consistent with acute mononucleosis. A biopsy of the liver lesion yielded islands of mature red blood cells and hematopoietic tissue but no hepatic tissue. Pathologic examination could not yield a definitive diagnosis.
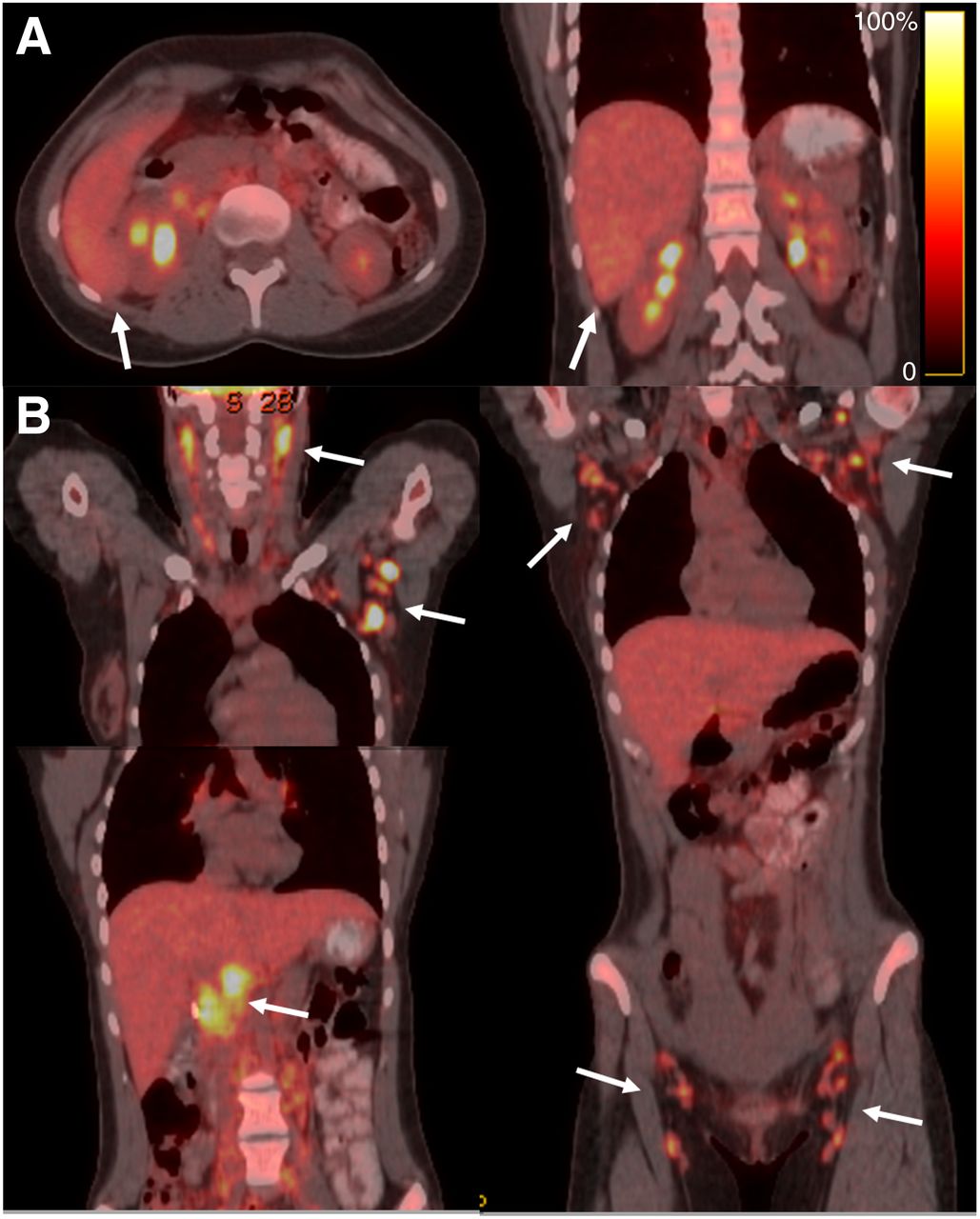
18F-FDG PET/CT was then performed to evaluate for a possible malignancy. The scan revealed extensive metabolically active lymphadenopathy throughout the body. A pertinent finding is that the hepatic mass was not metabolically active, as seen in Figure 3. However, this finding was not sufficient, as some cancers may not be 18F-FDG–avid.
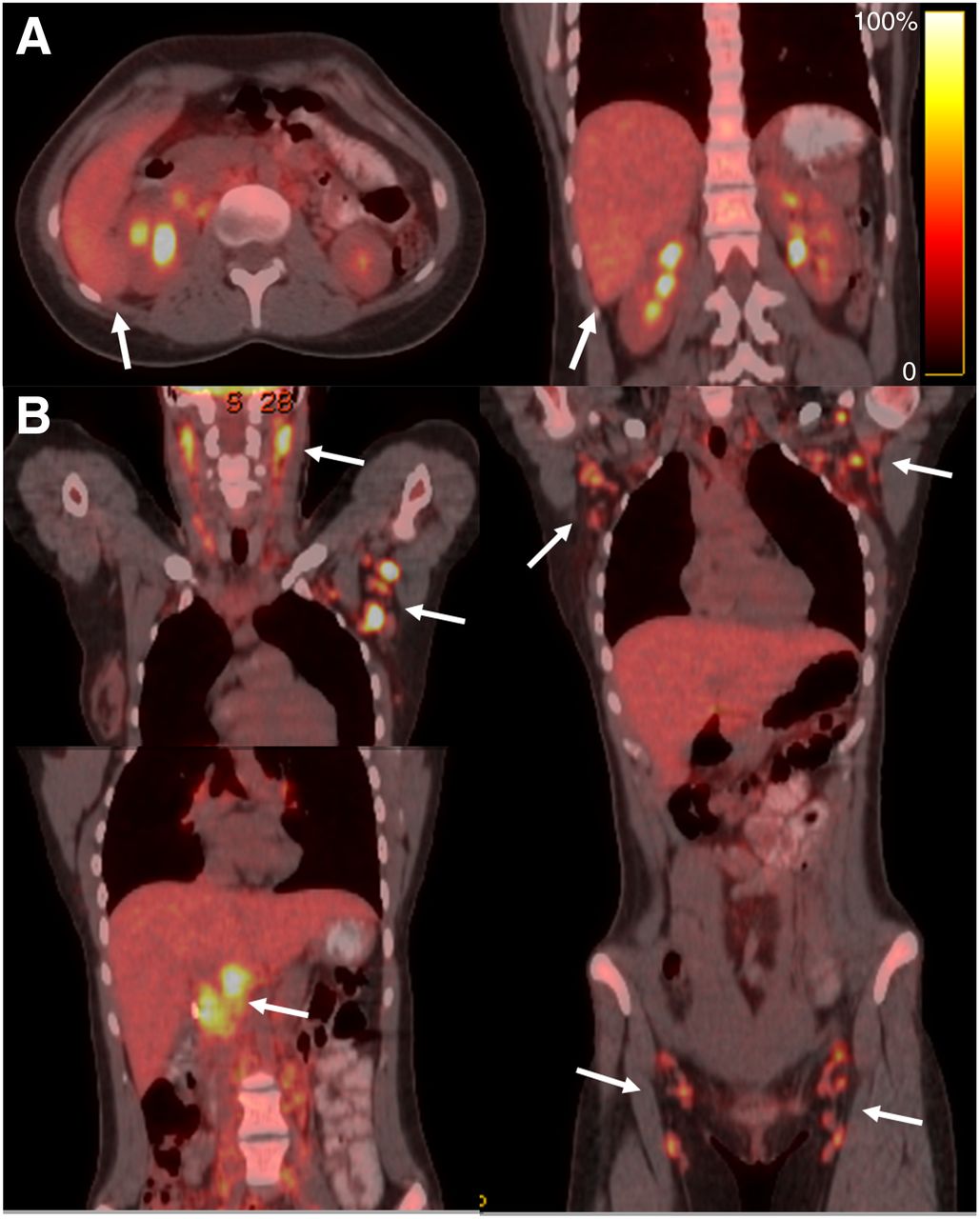
18F-FDG PET/CT images of lesion and lymphadenopathy (arrows). (A) Axial (left) and coronal (right) images show liver lesion exhibiting glucose metabolic activity similar to that of surrounding normal parenchyma. (B) Coronal (bottom left and right) images show widespread 18F-FDG–avid lymphadenopathy.
Biopsy of the left axillary lymph node biopsy was performed and found reactive lymphoid hyperplasia positive for Epstein–Barr virus. Infectious mononucleosis was established; however, the nature of the hepatic lesion remained unclear even after a biopsy. Further investigations were sought.
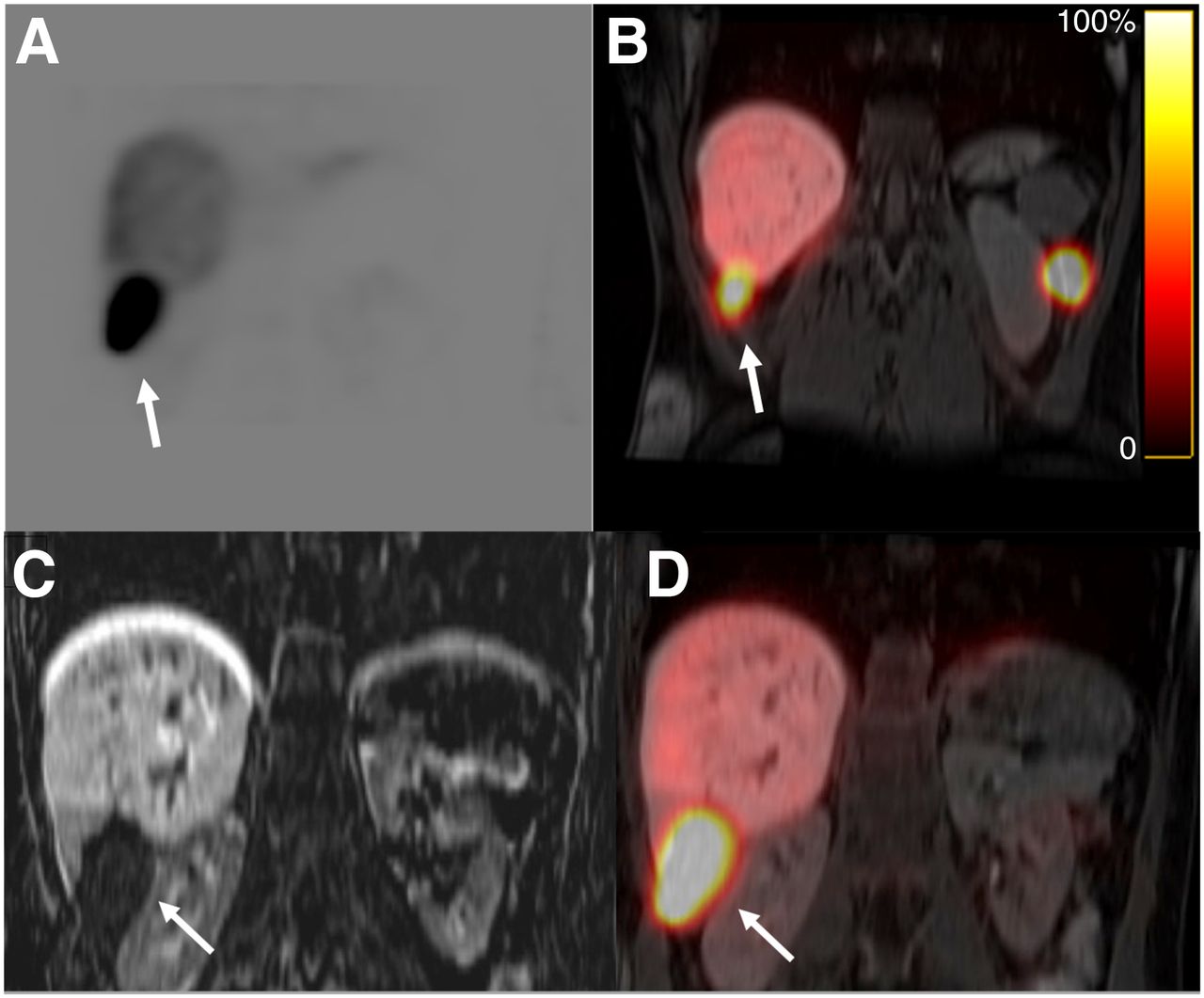
Because hematopoietic tissue was found in the hepatic lesion biopsy sample, a 99mTc-radiolabeled heat-damaged red blood cell SPECT/CT scan was obtained to evaluate for hepatic splenosis. This scan showed focal uptake correlating with the mass seen on the MRI (confirming hepatic splenosis) and a smaller focus of uptake in the left upper quadrant of the abdomen (splenule), shown in Figure 4. The patient was advised that her abdominal pain was likely related to inflammation of the ectopic splenic tissue and would improve with resolution of her infectious mononucleosis. She has done well.
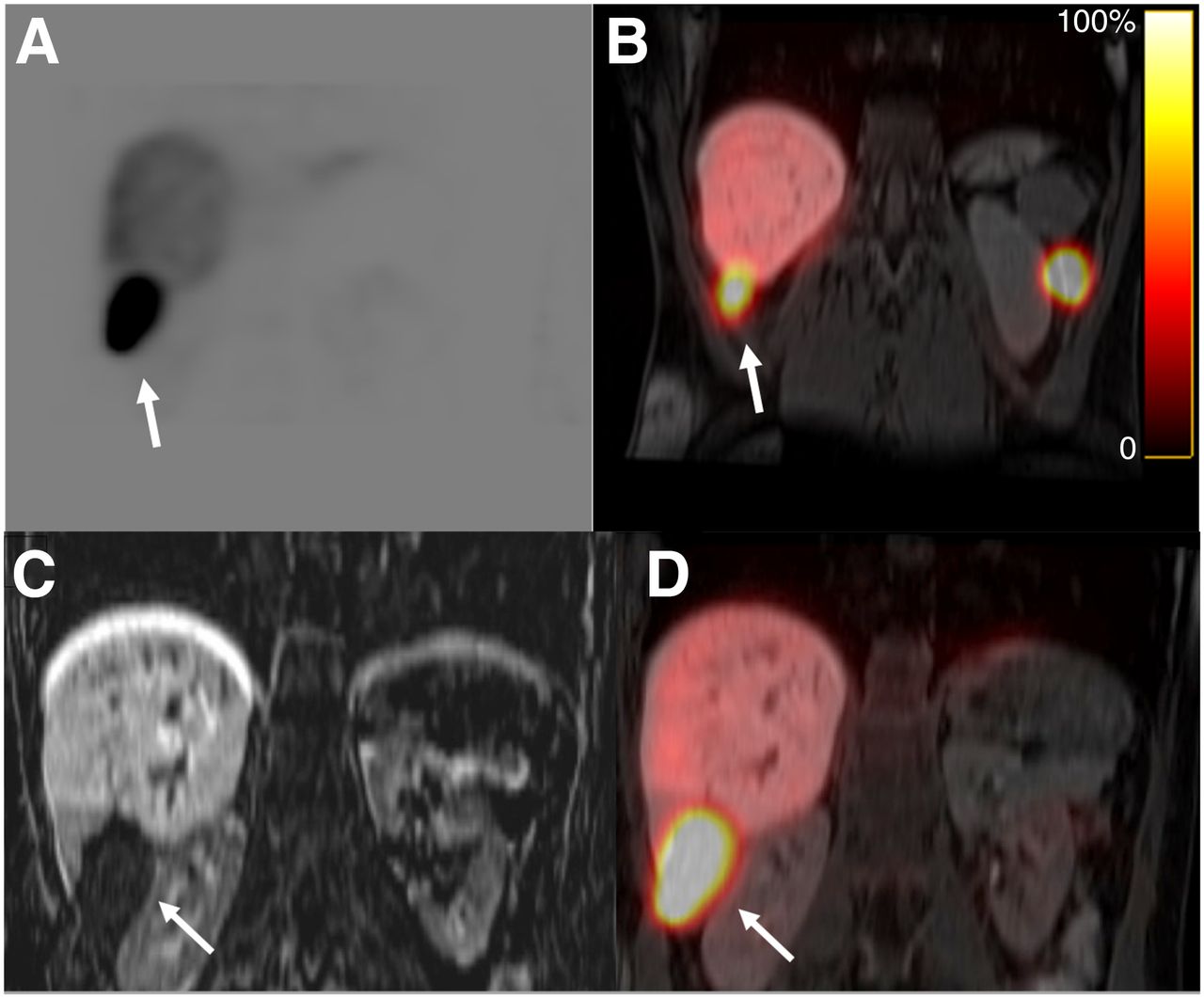
(A and B) 99mTc-labeled heat-damaged red blood cell images show increased uptake in hepatic (A) and left flank (B) splenule. (C and D) Coronal T1-weighted MR (C) and SPECT/MR (D) images show intrahepatic splenosis in unusual location (arrows).
DISCUSSION
Even with a relevant clinical history (splenectomy, trauma), hepatic splenosis can be challenging to diagnose and can be confused with focal nodular hyperplasia, adenoma, hepatocellular carcinoma, or metastases (1–4). MRI is the modality of choice for evaluating liver lesions. However, in clinical practice, the findings may not always be straightforward.
A review of the literature showed that about 75% of reported cases of hepatic splenosis were in men and that 95% of reported cases had a history of splenectomy. Only about 37% had no risk factors, and about 60% either had risk factors for hepatocellular carcinoma or had a preexisting malignancy.
The blood supply of splenules is derived from local arteries at implantation sites (1). Even though 99mTc-sulfur colloid or 99mTc-labeled heat-damaged red blood cells efficiently target ectopic splenic tissue (5,6) and clinch the diagnosis, invasive diagnostic measures are still performed in more than 50% of cases. About 79% of reported cases used a biopsy, fine-needle aspiration, or surgery to fully diagnose the hepatic lesion. It is surprising that only 21% underwent scintigraphy.
Coregistration of datasets from SPECT/CT or SPECT/MRI and 99mTc-labeled heat-damaged red blood cells is the best test to evaluate for splenosis or accessory spleens. Sulfur colloid, because of its normal liver biodistribution, would be a second choice. The sensitivity, specificity, and accuracy of these studies have improved. Prior reported concerns about the detectability of small lesions, or proximity to major vascular structures and the remaining spleen, are no longer applicable. As in our case, several tests were performed, whereas scintigraphy would have completed the work-up early. These techniques should be used more frequently to decrease complications, the financial burden, and anxiety related to costly follow-up imaging and invasive procedures.
CONCLUSION
In difficult cases of hepatic splenosis, scintigraphy can be of great value, especially with novel SPECT/CT and SPECT/MRI techniques.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Dec. 6, 2021.
REFERENCES
- Received for publication August 6, 2021.
- Revision received October 25, 2021.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.