


Abstract
When patients are referred for SPECT myocardial perfusion imaging with 99mTc agents, attention focuses on the tracer activity in the myocardium. Apart from myocardial activity, normal biodistribution of 99mTc-sestamibi and 99mTc-tetrofosmin is seen in the thyroid, liver, gastrointestinal tract, kidneys, and urinary bladder. These structures may be visualized when a γ-camera with a large field of view is used for SPECT imaging. This case report presents a serendipitous finding of a pelvic mass, which was identified because of the extended field of view afforded by the conventional γ-camera used for SPECT myocardial perfusion imaging and detected because of a review of the raw images by the nuclear medicine technologist. This case emphasizes the importance of training the nuclear medicine technologist to review the raw data in the entire field of view before study completion.
Incidental extracardiac findings in patients who undergo PET/CT and SPECT/CT have been documented, with the fraction of incidental findings being as high as 60% (1). The number of incidental findings that led to potentially treatment-altering diagnoses of previously unknown and treatable malignancies was low, at no greater than 0.5% (1). It is important to review incidental findings, as these will occasionally be found when the CT datasets of hybrid SPECT/CT and PET/CT myocardial perfusion imaging (MPI) studies are carefully reviewed in different imaging windows (1). Another published study showed that 60% of the major findings and 48% of the minor findings in SPECT/CT MPI studies were unknown at the time of nuclear imaging (2). This study stated that potentially significant abnormal findings on the nondiagnostic-CT portion of the cardiac SPECT/CT examination were detected in 10.5% of reported patients (2). These data suggest that, in addition to the emission image findings, the CT findings should routinely be assessed for major diagnostic abnormalities (2). The requirement for institutional review board approval was waived, as this retrospective descriptive report of observations does not attempt to answer research questions; every attempt has been made to protect the patient’s privacy.
CASE REPORT
A 73-y-old man with a past medical history of tobacco use, non–insulin-dependent diabetes, hypertension, and hyperlipidemia was referred for an MPI pharmacologic stress test because of increasing dyspnea symptoms at rest and with exercise. He was unable to undergo a treadmill exercise test because of symptomatic claudication of the right leg after walking more than a short distance. The findings of a chest radiograph were unremarkable. A transthoracic echocardiogram showed normal left ventricular systolic function and mild diastolic dysfunction. Both pulmonary function tests and the ankle brachial index test had normal results.
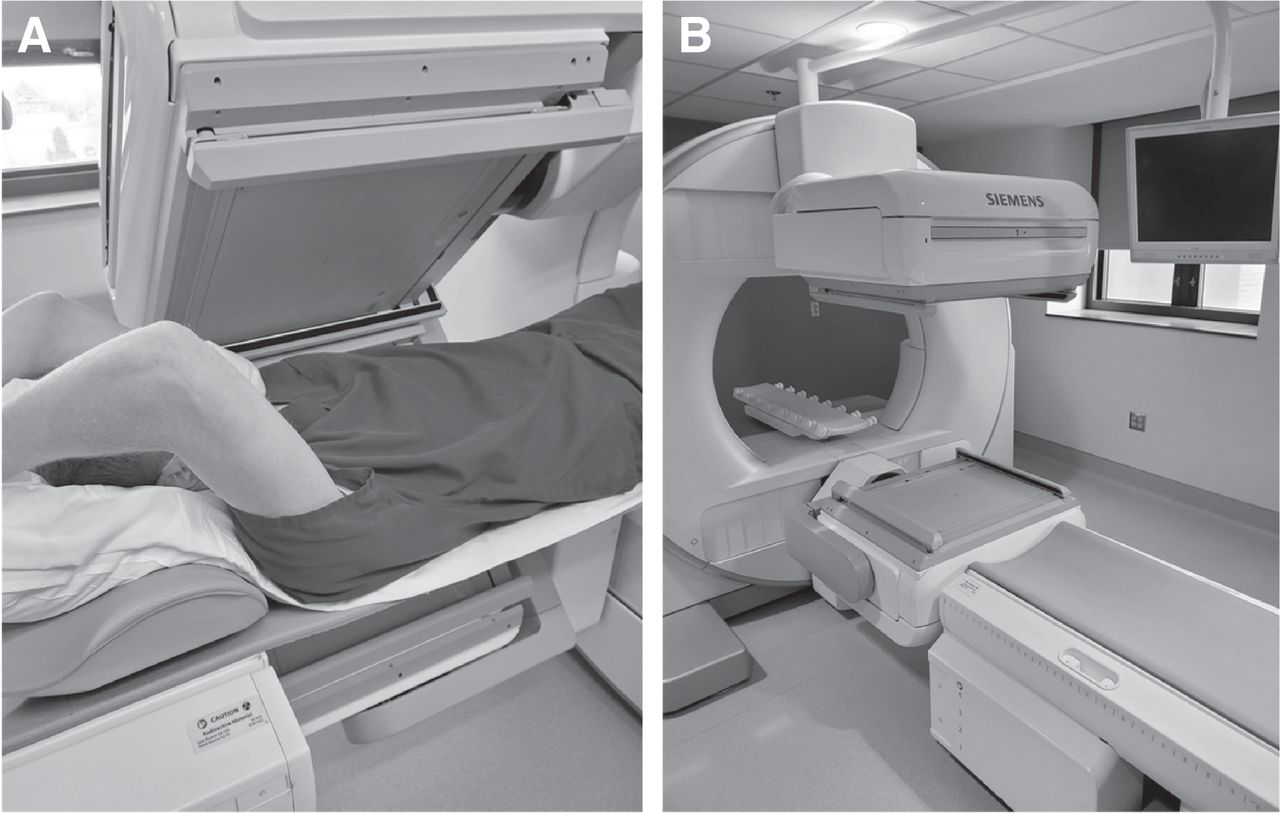
The patient was given an intravenous injection of 307.1 MBq (8.3 mCi) of 99mTc-sestamibi on arrival in the nuclear medicine department and underwent ungated rest SPECT MPI 30 min later. The imaging was acquired on a Siemens Symbia with dual large-field-of-view detectors (53.3 × 38.7 cm detector dimensions) and parallel-hole low-energy, high-resolution collimation (Fig. 1). Subsequently, in the stress laboratory, 0.4 mg of regadenoson followed by 1,172.9 MBq (31.7 mCi) of 99mTc-sestamibi was administered intravenously, and gated SPECT MPI was performed 60 min later.
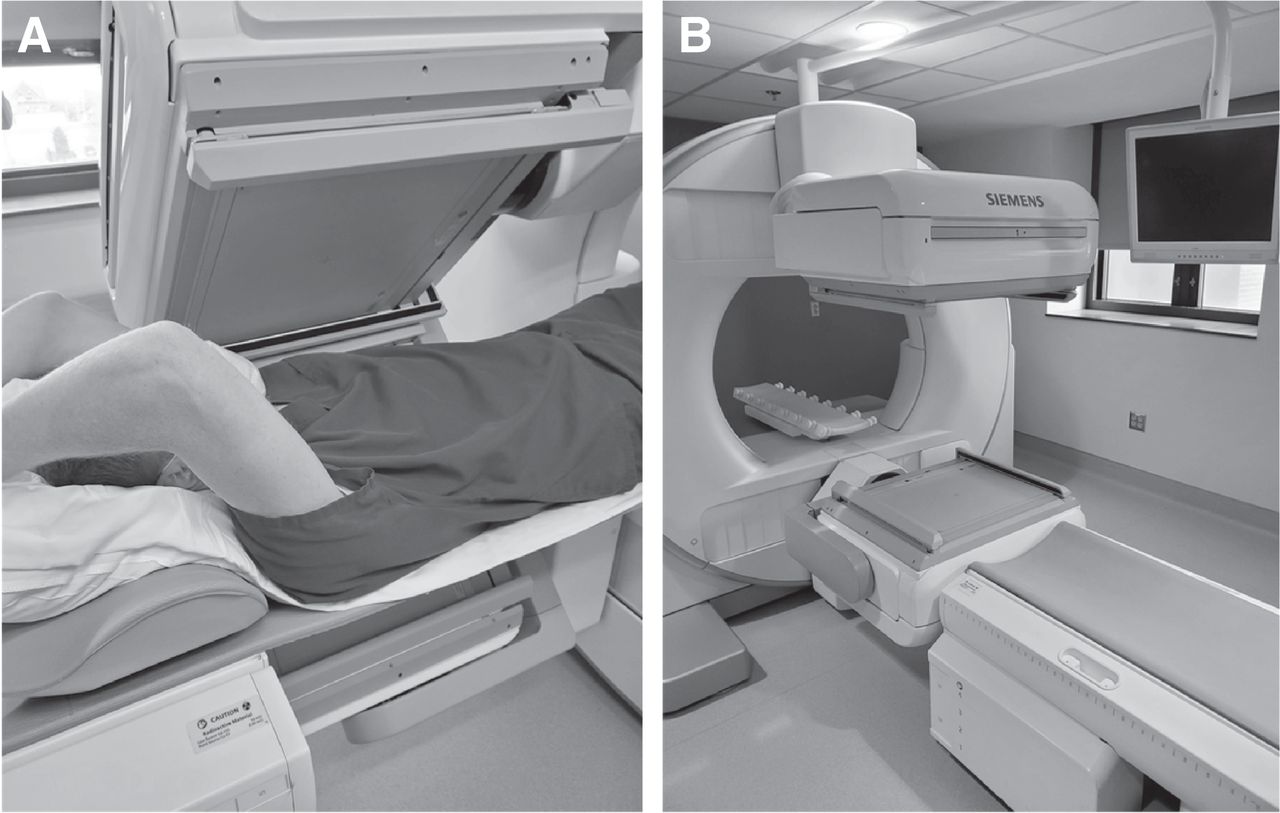
(A) Photograph showing typical patient positioning (supine with arms raised) during MPI and relative size of field of view. (B) Photograph of Siemens Symbia dual-head γ-camera in John Cochran Division of VA St. Louis Healthcare System.
When reviewing the rotating raw SPECT images before reconstruction of the rest and stress MPI images, the nuclear medicine technologist (NMT) noticed unusual displacement of the urinary bladder to the left, which was visible because of urinary excretion of the radiotracer (Fig. 2A). Before releasing the patient, the NMT brought this finding to the attention of the attending nuclear medicine physician. The patient denied knowledge of a pelvic abnormality, and no prior cross-sectional images of the abdomen or pelvis were found in the electronic medical record. It was decided that SPECT imaging with CT of the abdomen and pelvis was warranted to further characterize the finding.
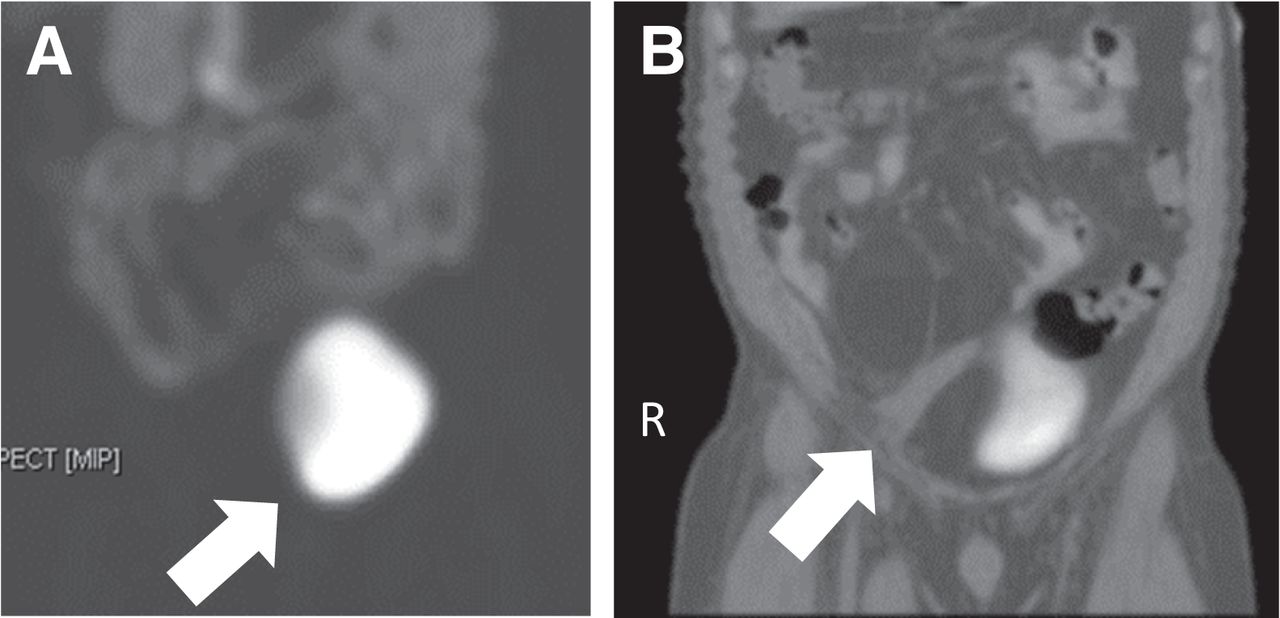
(A) SPECT image of abdomen and pelvis showing deviation of urinary bladder (maximum-intensity projection). Arrow shows deviation of urinary bladder. (B) SPECT/CT image of abdomen and pelvis showing deviation of urinary bladder by large mass (coronal view). Arrow shows deviation of urinary bladder in CT portion of image.
The MPI scan showed normal myocardial perfusion and normal left ventricular function. The SPECT/CT scan of the abdomen and pelvis showed deviation of the urinary bladder anteriorly, superiorly, and to the left by a large lipoma in the pelvis (Fig. 2B). The lipoma, which appeared to be multilocular and to have a thin capsule, measured approximately 10 × 15 × 9 cm, and caused a leftward deviation of the bowel loops, the inferior vena cava, and the infrarenal aorta. The right iliac arteries and veins were draped over the lipoma and were stretched anteriorly and to the left of midline. These findings were confirmed on diagnostic contrast-enhanced CT of the abdomen and pelvis (Fig. 3A), and CT angiography showed displacement and stretching of the right common iliac, external iliac, and internal iliac arteries without stenosis. The patient underwent surgical excision, with no untoward surgical complications. Dedicated CT of the abdomen and pelvis was completed after resection (Fig. 3B). Pathologic examination confirmed a benign lipoma, and the patient reported resolution of claudication after excision.

(A) Coronal view of abdomen and pelvis from dedicated diagnostic CT scan showing large lipoma in pelvis. This scan was obtained immediately after MPI study. Arrow shows deviation of urinary bladder before resection. (B) Coronal view from dedicated CT scan after resection of lipoma. Arrow shows where lipoma was before resection.
DISCUSSION
This case highlights the unique role of the NMT, who, in many clinical units, is the one individual reviewing raw rotating images in the entire field of view before image reconstruction. By virtue of such a dedicated review, unexpected findings can be further explored before the patient leaves the department. As we describe in this report, following such a protocol may reveal clinically important findings leading to appropriate investigation and diagnosis, thereby expediting patient management.
CONCLUSION
This case emphasizes the importance of training the NMT to review raw data in the entire field of view before study completion.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Feb. 23, 2021.
REFERENCES
- Received for publication October 7, 2021.
- Revision received December 28, 2021.
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.