


Article Figures & Data
Figures
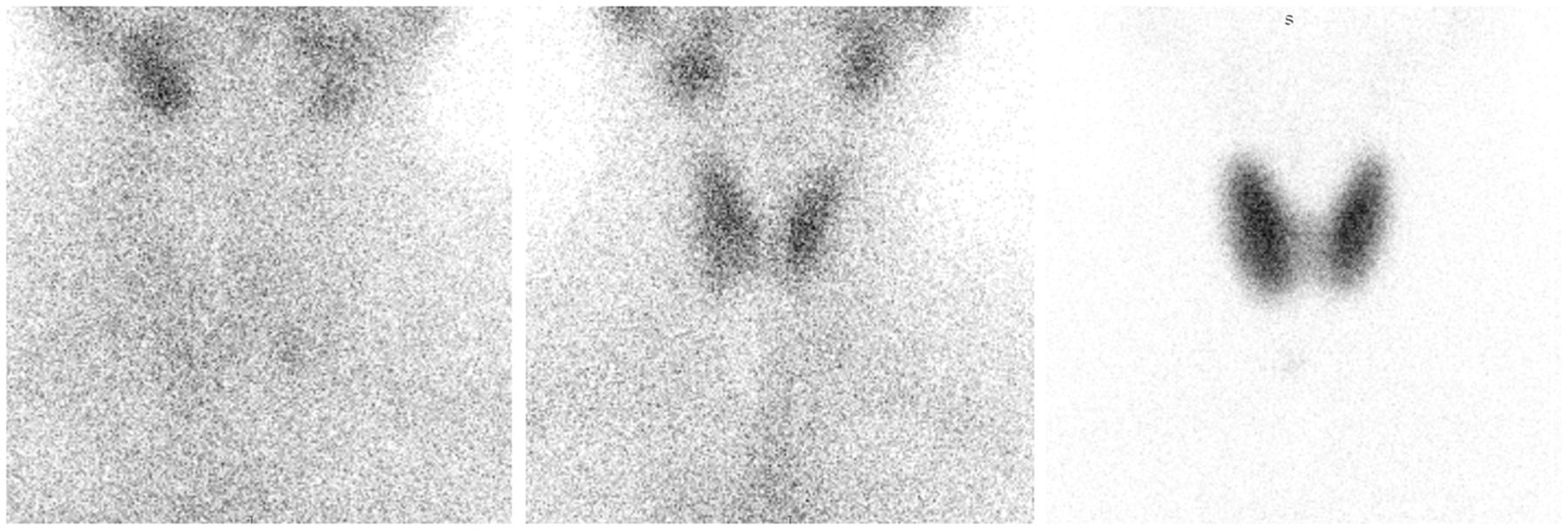
- FIGURE 1.
Intuitive, but sometimes inaccurate, visual evaluation of thyroid status relative to salivary gland activity. (Left) Salivary gland activity exceeding thyroid gland activity suggests hypothyroidism. (Middle) Salivary gland activity and thyroid gland activity being similar (within same scale) suggests euthyroidism. (Right) Salivary gland activity not being apparent relative to thyroid activity suggests hyperthyroidism. All images were obtained with 99mTc-pertechnetate using high-resolution, parallel-hole imaging.
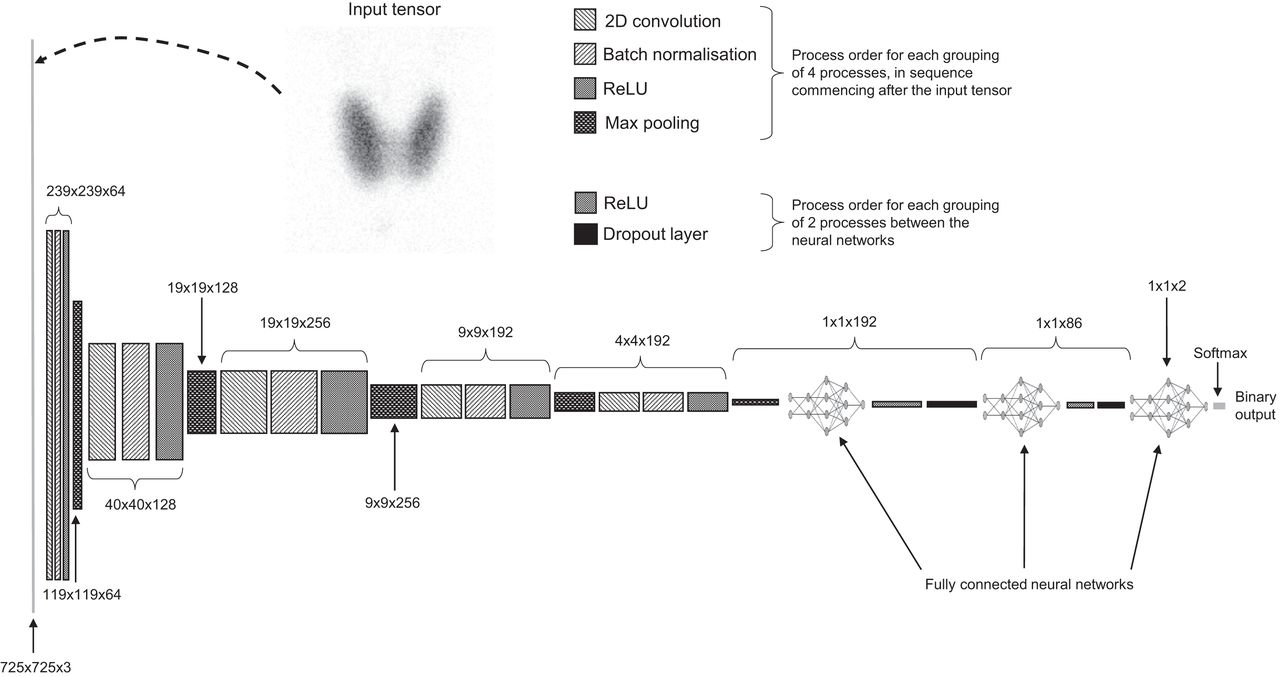
- FIGURE 2.
CNN architecture. 2D = 2-dimensional; ReLU = rectified linear unit.
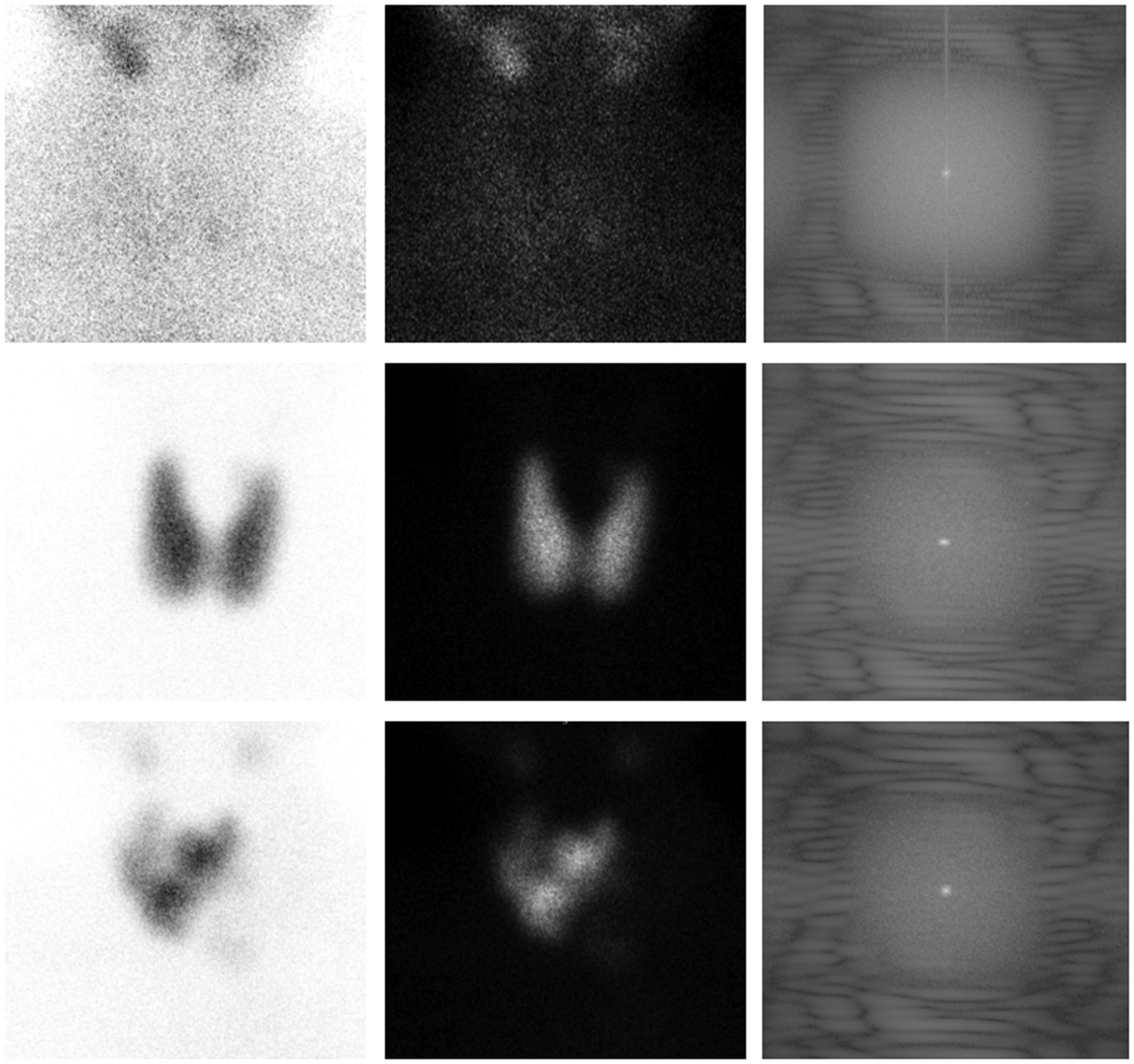
- FIGURE 3.
Three example patients (top, middle, and bottom) with black on white (left), white on black (center), and magnitude spectrum from Fourier transformation (right) used as inputs for CNN.
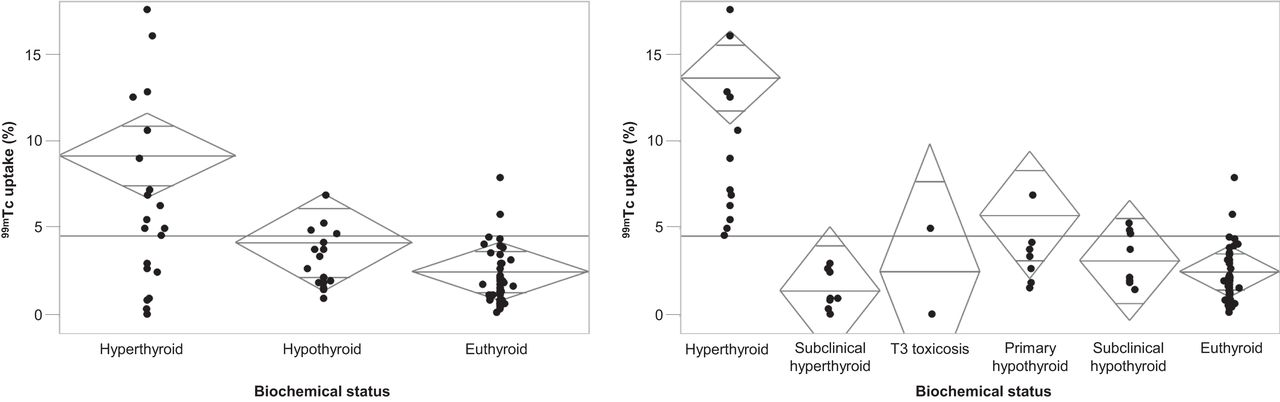
- FIGURE 4.
(Left) Ternary biochemical status classification against thyroid uptake. (Right) Broader biochemical status classification against thyroid uptake. Horizontal line represents overall mean, and diamonds represent class mean and 95% CIs.
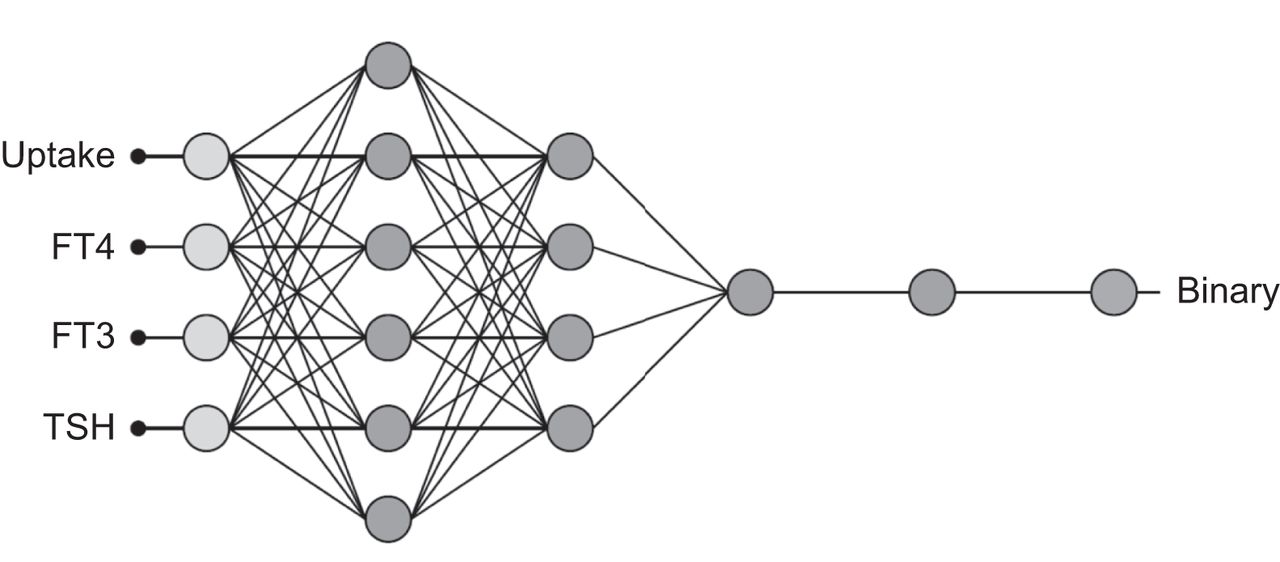
- FIGURE 5.
Final architecture of trained and validated neural network. TSH = thyroid-stimulating hormone.
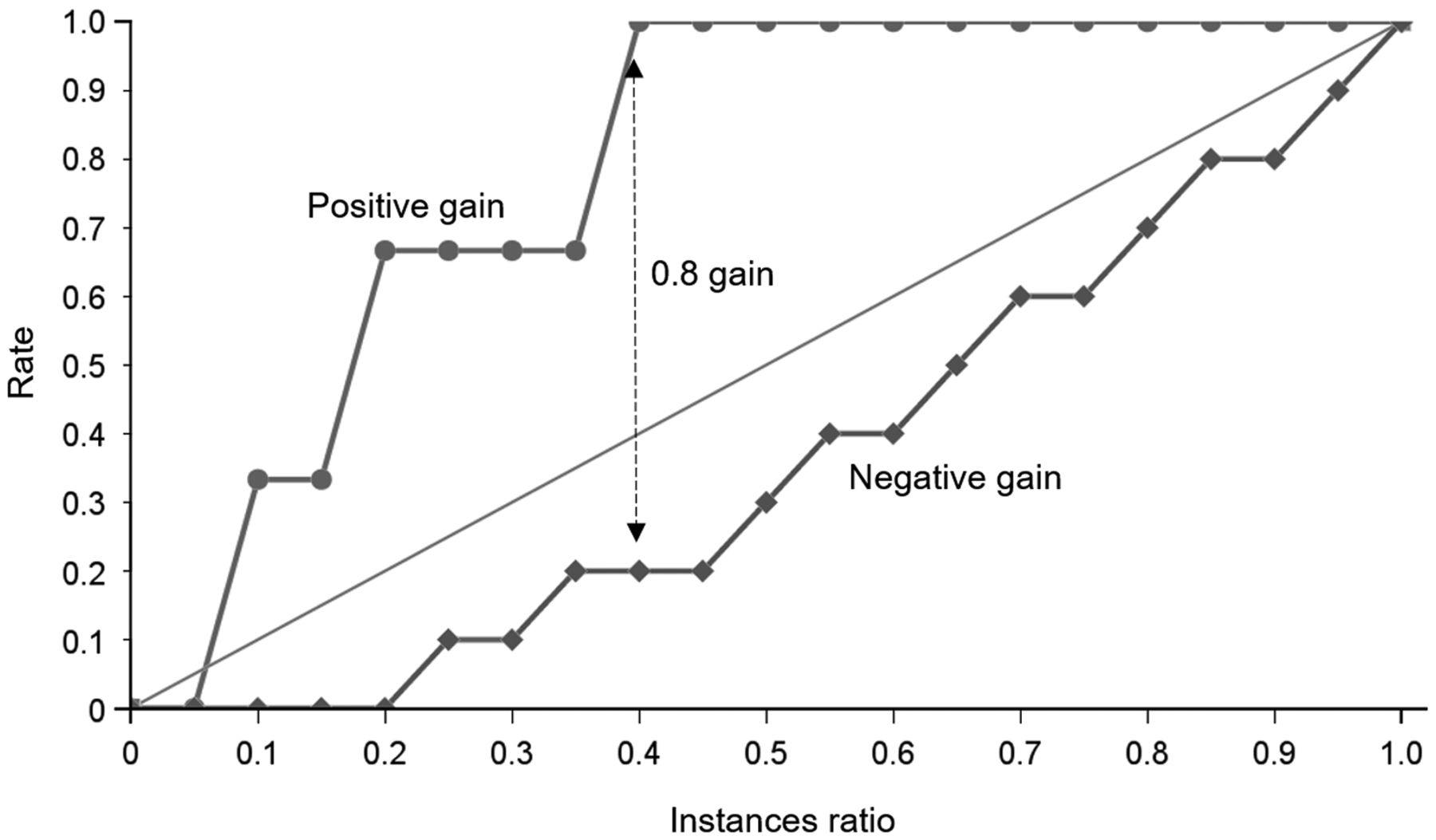
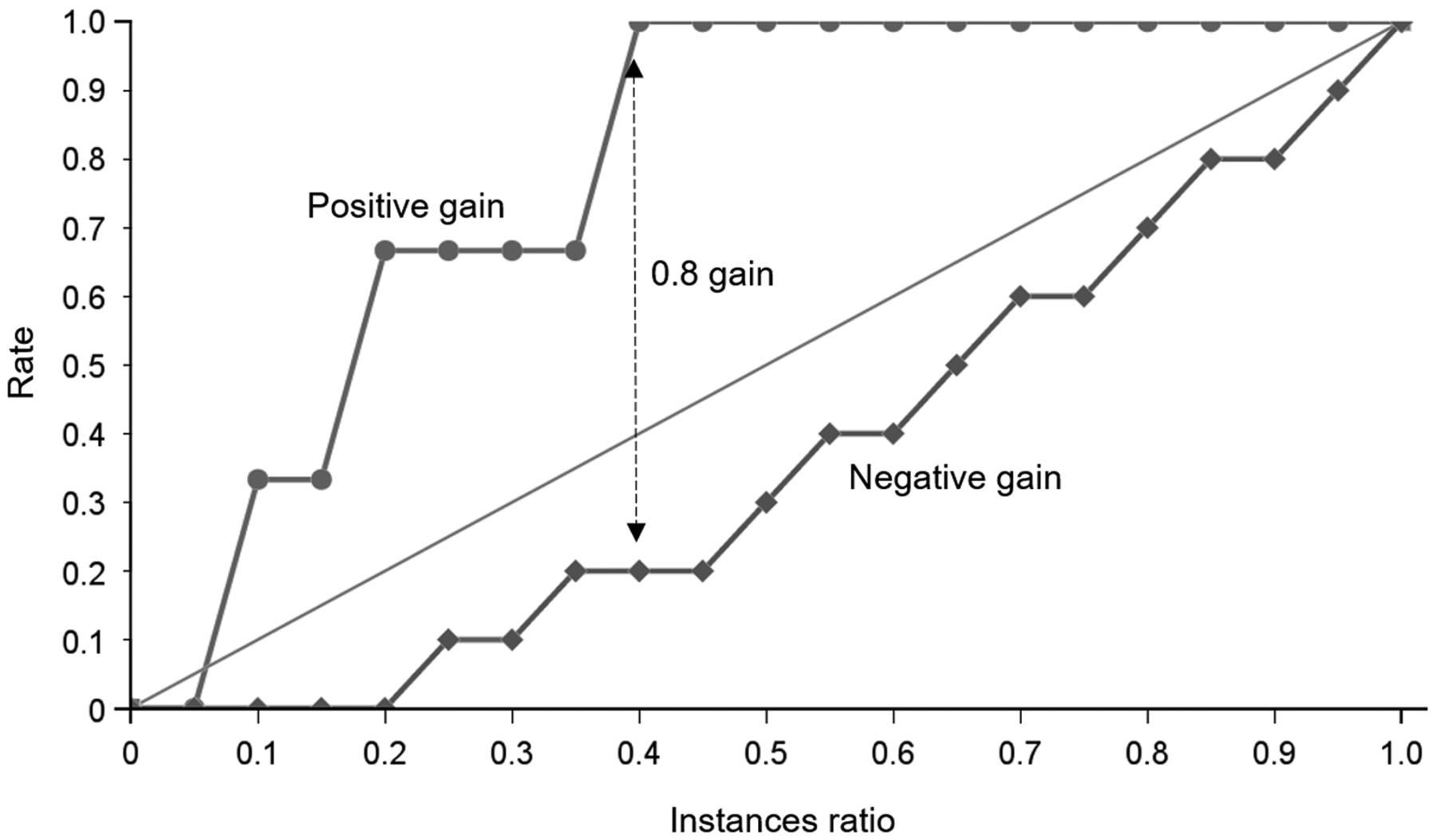
- FIGURE 6.
Cumulative gain chart demonstrating maximum separation of positive and negative curves to provide cumulative gain score of 0.8 and instances ratio of 0.4 (arrow).
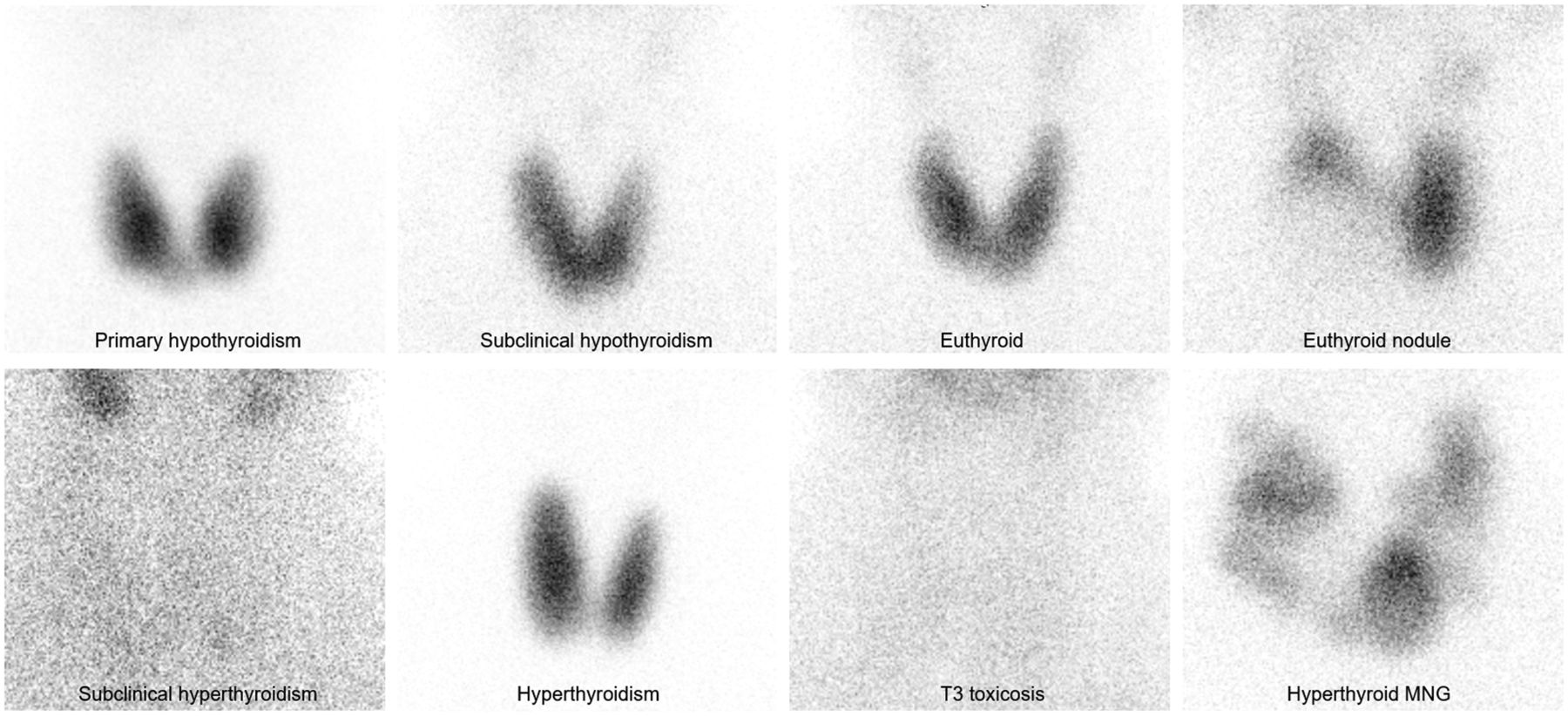
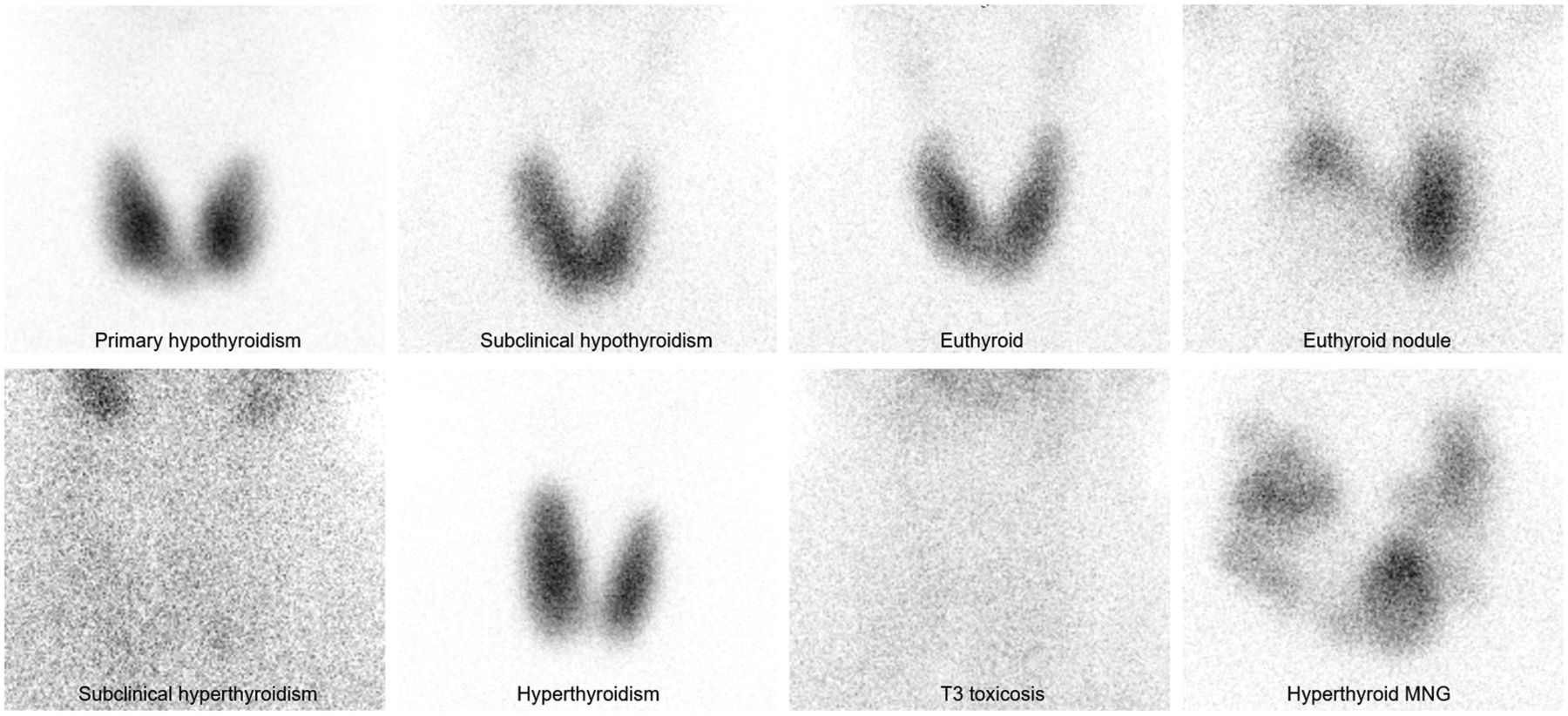
- FIGURE 7.
Various scintigraphic appearances of thyroid pathology using parallel-hole (high-resolution) collimation and 99mTc-pertechnetate. MNG = multinodular goiter.



Tables
Free T3 (2–7 pmol/L*) Free T4 (12–30 pmol/L*) Thyroid-stimulating hormone (0.45–4.5 μIU/mL*) Biochemical status 99mTc uptake (%) Comment on uptake reference range High High Low Hyperthyroidism >4.5 0% FN rate Normal Normal Low Subclinical hyperthyroidism <4.5 including <0.45 or absent 0% TP, comprised FN or FP hypothyroidism High Normal Low T3 toxicosis >4.5 or <0.45 FP hypothyroidism Normal High Low Thyroiditis No cases Low Low Low Secondary hypothyroidism No cases Normal Normal High Subclinical hypothyroidism >0.45 but <4.5 100% FN Low or normal Low High Primary hypothyroidism >0.45 and in over 50% of cases >4.5 100% FN Normal Normal Normal Euthyroid <4.5% 9% FP rate (6% hyperthyroid, 3% hypothyroid) * Reference range.
Layer Name Activations Parameters 1 Tensor input layer [725,725,3] 2 2D convolution layer [239,239,64] Weights [11,11,3,64], bias [1,1,64] 3 Batch normalization [239,239,64] Offset and scale [1,1,64] 4 ReLU layer [239,239,64] 5 Max pooling layer [119,119,64] Size [3,3], stride [2,2], padding [0,0,0,0] 6 2D convolution layer [40,40,128] Weights 5,5,64,128], bias [1,1,128] 7 Batch normalization [40,40,128] Offset and scale [1,1,128] 8 ReLU layer [40,40,128] 9 Max pooling layer [19,19,128] Size [3,3], stride [2,2], padding [0,0,0,0] 10 2D convolution layer [19,19,256] Weights [3,3,128,256], bias [1,1,256] 11 Batch normalization [19,19,256] Offset and scale [1,1,256] 12 ReLU layer [19,19,256] 13 Max pooling layer [9,9,256] Size [3,3], stride [2,2], padding [0,0,0,0] 14 2D convolution layer [9,9,192] Weights [3,3,256,192], Bias [1,1,192] 15 Batch normalization [9,9,192] Offset and scale [1,1,192] 16 ReLU layer [9,9,192] 17 Max pooling layer [4,4,192] Size [3,3], stride [2,2], padding [0,0,0,0] 18 2D convolution layer [4,4,192] Weights [3,3,256,192], bias [1,1,192] 19 Batch normalization [4,4,192] Offset and scale [1,1,192] 20 ReLU layer [4,4,192] 21 Max pooling layer [1,1,192] Size [3,3], stride [2,2], padding [0,0,0,0] 22 Fully connected layer [1,1,192] Weights [192,192], bias [192,1] 23 ReLU layer [1,1,192] 24 Dropout layer [1,1,192] 0.5 25 Fully connected layer [1,1,86] Weights [86,192], bias [86,1] 26 ReLU layer [1,1,86] 27 Dropout layer [1,1,86] 0.5 28 Fully connected layer [1,1,2] Weights [2,86], bias [2,1] 29 Softmax layer [1,1,2] 30 Classification layer Cross entropy loss function 2D = 2-dimensional; ReLU = rectified linear unit.
- TABLE 3.
Ternary Classification of Thyroid Function Based on Various Published Reference Ranges
Reference range Euthyroid Hyperthyroid Hypothyroid Reference 0.45%–4.5% 67.5% 26.8% 7.7% 6 0.4%–1.7% 35.0% 61.0% 4.0% 3 0.4%–4.0% 65.0% 31.0% 4.0% 4 0.3%–3.4% 57.7% 38.2% 4.1% 2 0.2%–2.0% 43.1% 52.8% 4.1% 5 Biochemical status 53.1% 27.1% 19.8%* 11 Salivary classification 44.8% 50.0% 5.2% — Physician visual rating 51.0% 43.8% 5.2% — Physician rating with uptake value 64.6% 29.2% 6.3% — *15.6% were hypothyroid without suppression of uptake (2.1% autonomous, 2.1% secondary hypothyroidism, 11.5% primary hypothyroidism, and 4.2% subclinical hypothyroidism).
Variable Mean 95% CI Total count ratio of right-lobe activity to left-lobe activity 1.5 1.03–2.02 CPP ratio of right-lobe activity to left-lobe activity 1.29 0.98–1.60 Area 33.8 cm2 31.1–36.5 Size, right 3092 pixels 2,848–3,340 Size, left 2937 pixels 2,662–3,212 Ratio of thyroid to background 4.06 3.43–4.69 Right 4.01 CPP 3.49–4.52 Left 4.08 CPP 3.28–4.89 Ratio of dose to total counts 4.85 3.44–6.26 FT4 21.1 pmol/L 18.1–24.2 FT3 7.1 pmol/L 5.1–9.1 Thyroid-stimulating hormone 4.2 pmol/L 2.3–6.1 - TABLE 5.
Ternary Classification of Thyroid Function Based on Recall Against Biochemical Status
Reference range Euthyroid Hyperthyroid* Hypothyroid Accuracy† 0.45%–4.5% 71.4% 66.6% (100%) 0% 82.6% 0.4%–1.7% 49.0% 74.1% (94.1%) 0% 51.0% 0.4%–4.0% 86.3% 63.0% (94.1%) 0% 77.1% 0.3%–3.4% 74.5% 63.0% (94.1%) 0% 68.8% 0.2%–2.0% 58.8% 74.1% (94.1%) 0% 59.4% Salivary classification 62.7% 70.3% (94.1%) 0% 61.4% Physician rating 72.5% 63.0% (89.5%) 0% 61.0% Physician rating with uptake 88.2% 70.3% (100%) 0% 82.3% * Data in parentheses exclude subclinical hyperthyroidism and T3 toxicosis.
↵†Binary accuracy for reference to Table 6.
Accuracy is also provided for binary classification.
- TABLE 6.
Triplicate Training and Validation Binary Results (Hyperthyroid or Not Hyperthyroid) for 30-Layer CNN Architecture
Input tensor Training accuracy Training loss Validation accuracy Validation loss Mean validation accuracy Binary accuracy White on black 82.1% 0.420 75.9% 0.536 80.5% 94.0% 0.225 79.3% 0.602 91.0% 0.218 86.2% 0.414 Black on white 83.6% 0.383 82.8% 0.405 78.2% 80.6% 0.452 72.4% 0.544 91.0% 0.232 79.3% 0.690 Magnitude spectrum 76.1% 0.459 75.9% 0.530 75.9% 74.6% 0.508 72.4% 0.542 85.1% 0.306 79.3% 0.380 Mean 84.2% 0.356 78.2% 0.516 Initial 25-layer CNN 69.0% Conventional metrics Normal cutoff, 4.5% 82.6% Normal cutoff, 4.0% 77.1% Salivary classification 61.5% Physician rating 61.0% Physician rating with uptake 82.3% Corresponding binary accuracies of best-performing thyroid uptake cutoffs, visual classification against salivary activity relative to thyroid activity, and physician rating are included for comparison.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}