


Visual Abstract

Abstract
We aimed to show that the acquisition time of a conventional bone scan could be reduced by half without losing the diagnostic value of the scan. Methods: Fifty adult patients (37 male and 13 female; mean age, 62.5 y; SD, 8.7 y) were enrolled. The patients were injected with 925–1,110 MBq (25–30 mCi) of 99mTc-methylene diphosphonate intravenously. The standard-protocol whole-body planar images were acquired first (scan speed, 10 cm/min; acquisition time, ∼20 min) and were followed immediately by the half-time protocol whole-body planar images (scan speed, 20 cm/min; acquisition time, ∼10 min). Both sets of images were interpreted by 2 nuclear medicine physicians. Each reviewer, when reviewing the standard-protocol images, was self-masked to the result he or she had obtained when reviewing the half-time images, and vice versa. This self-masking was accomplished by allowing a minimum of 2 wk to elapse between the 2 interpretations. We used the κ-coefficient to compare agreement between the standard-protocol results and the half-time results. Results: There was no difference in clinically significant diagnostic information between the half-time and standard protocols. The diagnostic quality of half-time and standard-protocol images did not significantly differ (0.86 < κ < 1.0). Conclusion: Our data suggest that if we reduce the 99mTc-methylene diphosphonate dose by half and keep the acquisition time at its standard value, we gain the benefit of reduced dose without loss of diagnostic value.
Medical imaging is a major source of the radiation dose to humans (1). The dose delivered by the injected radiopharmaceuticals used in medical imaging is second only to the dose given by CT. Many of the radiopharmaceutical dose recommendations were formulated in the 1970s and early 1980s, and although there has been a significant improvement in γ-camera technology since then, many of those recommended radiopharmaceutical doses have remained unchanged. With the increase in the use of medical imaging that applies ionizing radiation, the dose delivered to human populations has been increasing, and there is a concerted effort to reduce this radiation burden. For example, in nuclear cardiology, the initial attempt to reduce the radiation dose in myocardial perfusion imaging was to use a protocol in which the first image obtained was a low-dose stress image (2). Furthermore, the radiopharmaceutical dose has been reduced in the last 10 y by using advanced processing software such as Astonish (Philips) (3,4). Radiation dose reduction has also been possible through the use of solid-state detectors with better sensitivity, such as cadmium-zinc-telluride detectors (5).
As another example, the Society of Nuclear Medicine and Molecular Imaging and other societies have introduced the Image Wisely initiative to clinical practice (1). This initiative has resulted in studies demonstrating that images obtained with a decreased dose of a radiopharmaceutical can provide diagnostic information comparable to that from a full dose, such as 99mTc-mertiatide imaging for assessment of renal function and obstruction (6,7). The Image Wisely campaign was initially launched by the American College of Radiology and the Radiological Society of North America (1).
Decreasing the injected dose of radiopharmaceuticals will decrease not only the radiation dose delivered to the patient but also the dose received by the technologist who performs the study. In times of technetium shortage, which has been a recurrent problem in recent years, reducing the radiotracer dose may result in greater patient throughput (8).
99mTc-methylene diphosphonate (99mTc-MDP) planar bone scintigraphy is commonly used to evaluate malignant and benign conditions of the bone (9–11). Other bisphosphonate-derived radiotracers are used in other continents, although 99mTc-MDP is the most widely used in the United States. In the United States, the usual administered activity of 99mTc-MDP for bone scintigraphy in adults is 500–1,110 MBq (∼13–30 mCi) (12); in Europe, a weight-based activity is customary and varies from 8 to 10 MBq/kg (11). In markedly obese adults, the administered activity could be increased to 11–13 MBq/kg (300–350 μCi/kg) (12).
In attempts to follow current optimal practices of patient-centered care by reducing the radiation dose in routine nuclear medicine examinations, our study aimed to prospectively evaluate the diagnostic value of half-time bone scans compared with standard-time scans. We obtained a full-dose scan in half the normal acquisition time, after obtaining a scan using the normal acquisition time. This stratagem allowed us to determine the clinical value of the standard-protocol scan while simultaneously obtaining a half-time scan for comparison, without the need to scan on different days and without increasing the radiation dose to the subjects.
MATERIALS AND METHODS
This was an institutional review board–approved prospective study. Adult patients scheduled to receive an 99mTc-MDP bone scan, who were over the age of 18 y and gave written informed consent, participated in this research study from May 2016 to December 2017. Fifty patients (37 male and 13 female; mean age, 62.5 y; SD, 8.7 y) were enrolled; their findings before this study were as follows: 47 had a malignancy (32 prostate cancer, 9 breast cancer, 1 thyroid cancer, 2 rectal cancer, 2 lung cancer, and 1 esophageal cancer) and 3 had benign bone lesions (2 Paget and 1 benign spinal lesion on MRI). The body mass index ranged from 17.5 to 43.2, with a mean of 28.2 and an SD of 7.9.
The patients were injected with 925–1,110 MBq (25–30 mCi) of 99mTc-MDP intravenously, which is the standard for adults in the United States (12). Images were acquired after approximately 180–240 min. The standard-protocol whole-body planar images were acquired first (scan speed, 10 cm/min; acquisition time, ∼20 min) and were followed immediately by the half-time protocol total-body planar images (scan speed, 20 cm/min; acquisition time, ∼10 min). Philips γ-cameras (Bright View and Precedence) with low-energy high-resolution collimators were used.
Standard-protocol and half-time images were independently interpreted by 2 experienced nuclear medicine physicians, who were masked to the results of the other reviewer. The image interpretation was subjective as well as objective. Reviewer A had more than 30 y of experience, and reviewer B had 10 y of experience. Each reviewer, when reviewing the standard-protocol images, was self-masked to the result he or she had obtained when reviewing the half-time images, and vice versa. This self-masking was accomplished by allowing sufficient time (a minimum of 2 wk) to elapse between the 2 interpretations. The order in which the standard-protocol and half-time images were interpreted was random. The time of injection to the time of imaging was recorded for all patients in both protocols.
After this analysis, 1 reviewer then looked at the standard-protocol and half-time images side by side to assess whether there were any artifacts, noise, patient motion, or change in positioning between the two.
The reviewers used the following objective scoring scale for each lesion identified on the standard-protocol and half-time studies: 1, intensity hotter than background; 2, moderate intensity; 3, intensity similar to bladder or kidney; and 4, photopenic. In addition, the following lesion characterizations were used: D, degenerative; M, metastases; C, contamination; P, primary bone tumor; and O, other. To minimize bias, clinical information, results of the prior bone scans, or reports from other imaging modalities were not made available to the reviewers while they were interpreting for this study. The usual artifacts such as urine contamination, minor dose infiltration, or photopenic artifacts due to prostheses did not pose problems for either of the experienced readers.
RESULTS
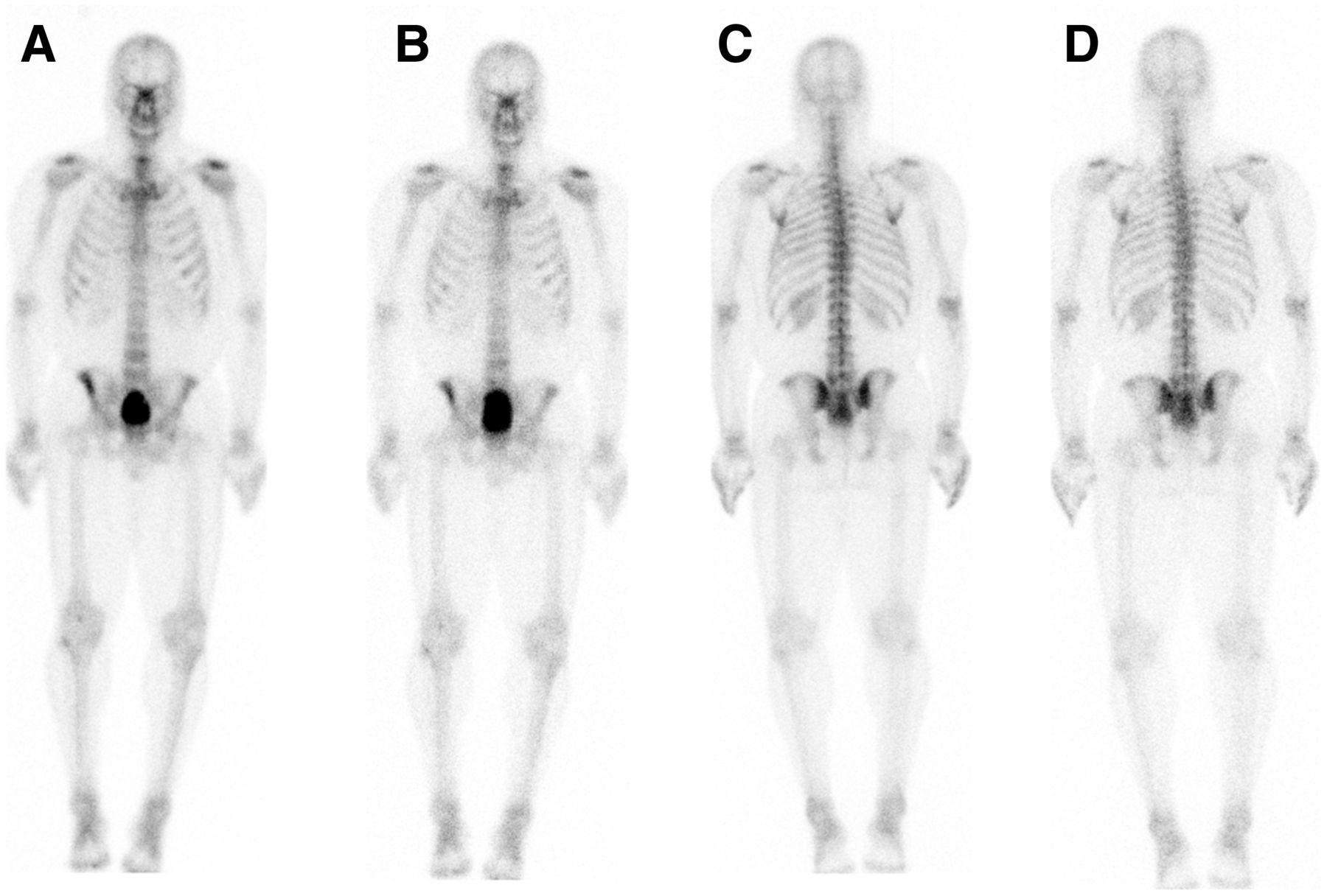
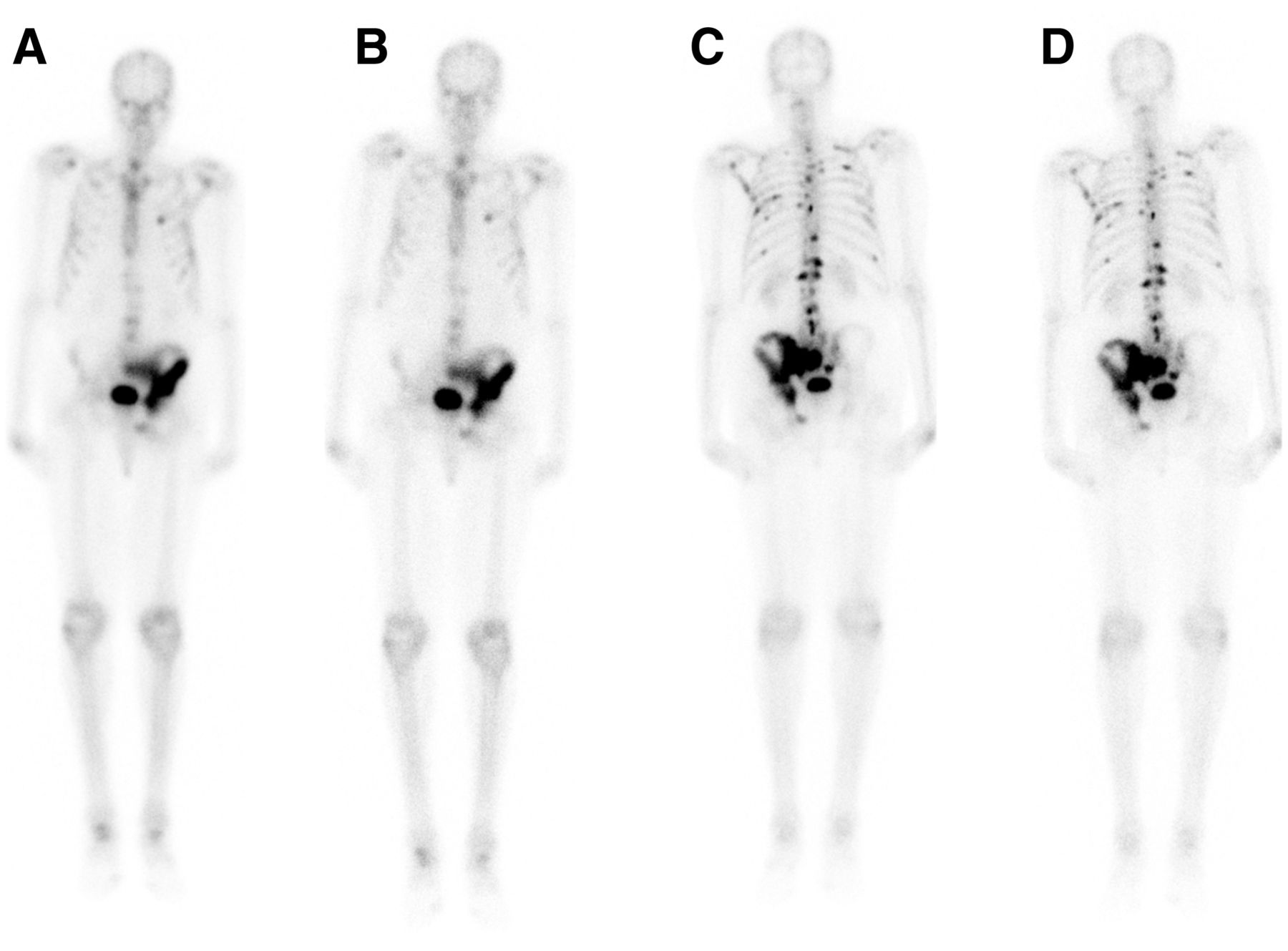
Figure 1 shows images for a subject with negative findings, with a comparison being made between the standard-protocol and half-time protocol anterior images and between the standard-protocol and half-time protocol posterior images. Figure 2 shows a similar comparison for a subject with extensive metastases.

Planar anterior (A and B) and posterior (C and D) scintigraphic images of skeleton of patient being evaluated for prostate cancer metastasis. Images were obtained using standard (A and C) and half-time (B and D) protocols. Bladder is larger in B than in A because of time lapse between standard and half-time acquisitions. There were no findings suggestive of metastasis on this scan.
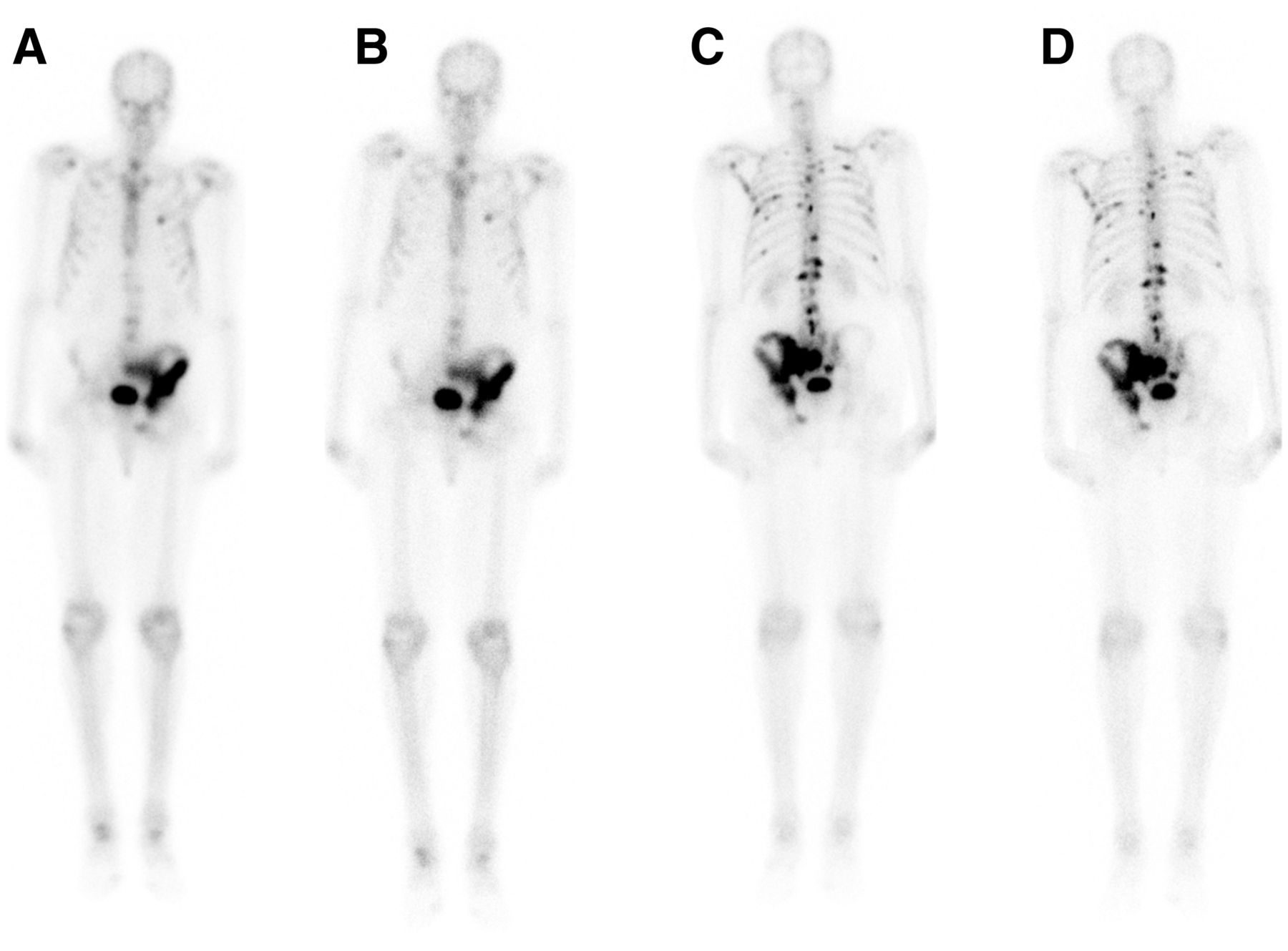
Planar scintigraphic images of skeleton of patient different from that in Figure 1, also being evaluated for prostate cancer metastasis. Planar anterior (A and B) and posterior (C and D) images were obtained using standard (A and C) and half-time (B and D) protocols. There is uptake throughout left iliac bone and within multiple ribs and vertebral bodies, better seen on posterior views, in pattern likely representing osseous metastasis. Degenerative uptake is noted in shoulders, ankles, and knees.
Although our aim was to compare the results of the standard protocol with the half-time protocol, we also checked interobserver variability between the 2 reviewers. There was complete concordance between the 2 reviewers on the standard-protocol images; that is, both reviewers found the same 21 patients to have metastatic lesions and the same 29 patients to be without metastatic lesions. When the results of half-time images were compared between the 2 reviewers, the reviewers had different interpretations for only 1 patient, for whom reviewer A interpreted the foci to be degenerative and reviewer B did not mention the metastatic lesion. Except for this 1 lesion, all lesions were identified by both reviewers in the standard-protocol and half-time images. There were a few discordant interpretations between the 2 reviewers in categorizing degenerative versus metastatic disease; however, this discordance was similar between the standard and half-time protocols.
We used the κ-coefficient (13) to compare agreement between the standard-protocol results and the half-time results for the same reviewer. That is, the standard protocol and the half-time protocol were treated as separate reviewers. The comparison used 6 categories: D, one or more degenerate lesions found; M, one or more metastatic lesions found; T, trauma; D and M; T and M; and none, no lesion. For example, for 1 patient, the half-time review found only degenerative lesions whereas the standard-protocol review found both degenerative and metastatic lesions, and for 6 patients, both the standard-protocol review and the half-time review found both degenerative and metastatic lesions. For both reviewers, κ was 0.9390, the calculated SD was 0.0421, and the 95% CI was 0.86 < κ < 1.0.
DISCUSSION
Bone scintigraphy is one of the most common studies performed daily in nuclear medicine departments that have a high volume of oncologic patients. Although bone scintigraphy is considered to expose patients to only a modest amount of radiation, that amount is not to be underestimated. Bone scintigraphy is also done to evaluate for benign conditions, such as osteomyelitis, stress fractures, Paget disease, pain, fractures, and suspected infection of prosthetics (11).
Reducing radiation dose is important in all groups of patients, including those with cancer and those without cancer. Efforts in radiation dose reduction have been more intense in the area of nuclear cardiology.
This prospective study consisting of 50 adults found no statistical difference in diagnostic information between half-time and standard acquisitions.
Factors such as poor renal function, poor hydration, dose infiltration, large body habitus, and patient motion can affect the quality of bone scintigraphy images. Poor renal function, poor hydration, and dose infiltration will have the same effect on both half-time and standard acquisitions.
A large body habitus can increase attenuation of photons and adversely affect the quality of the scan. Body mass index is a good indicator of body habitus, and the patient population we studied had a wide range of body mass index. There were no differences in quality or accuracy between the standard and half-time studies for the body mass index range of this study.
There were no large infiltrations of the injected dose in our study. However, the side-by-side comparison of the standard and half-time images, performed after the separate readings, showed 1 patient with head and pelvis motion between the 2 scans; this was the patient for whom the half-time protocol found only degenerative lesions but the standard protocol found both degenerative and metastatic lesions.
Some limitations of this study are that it used a relatively small number (50) of only adult subjects, all from a single institution, and that it used γ-cameras from a single vendor (Philips). No camera-specific analysis was done to see whether the camera type influenced the results in some way, and this lack is also considered a limitation. The particulars of our patient population also led to some biases. Prostate cancer metastases are typically osteoblastic and show an increased tracer concentration, whereas multiple myeloma, renal disease, and thyroid disease usually demonstrate osteolytic lesions and avascular necrosis of the bone—conditions that present as photopenic defects on bone scintigraphy images. Since most patients in this study had prostate cancer, there were more instances of intense foci of uptake and very few of photopenic regions, and thus our study could not satisfactorily test the detection rates of osteolytic lesions presenting as photopenic lesions. Because we did not use weight-based doses, our results may not be applicable in countries—such as those in Europe—that do use weight-based doses. Finally, our time from injection to imaging was 2 h 30 min for standard-protocol images and 2 h 55 min for the half-time images. Although this 25-min difference would not be expected to cause a significant change in the biodistribution of the isotope, an ideal research study might have acquired the half-time images first for 25 of our 50 patients. However, since the standard-protocol images were part of the standard clinical protocol for these patients, good clinical practices required that we obtain them first.
CONCLUSION
We compared the diagnostic accuracy of our half-time image protocol with that of our standard-time image protocol, using the standard recommended radiation dose. We found that the diagnostic quality of half-time and standard-time images did not significantly differ. Since the half-time images have, on average, half the counts of the standard-time images, a reasonable assumption from these results is that by halving the original dose but maintaining the standard acquisition time (a procedure that would also result in half the counts), a clinically useful image will result. A multicenter, multivendor camera study is needed to determine whether our result would be true for patient populations different from the one in this study.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online July 30, 2021.
REFERENCES
- Received for publication February 21, 2021.
- Revision received May 10, 2021.





{kind=link}
{kind=link}
{kind=link}