


Abstract
Immune checkpoint inhibitor (ICI) treatments activate T cells against tumors. Activated T cells attack not only the tumor but also healthy cells, causing an autoimmune reaction in various tissues. These immune-related adverse effects (IRAEs) cause 18F-FDG uptake in various tissues due to inflammation. It is important to recognize and report these findings on 18F-FDG PET/CT studies. 18F-FDG PET helps to determine the presence, location, and severity of IRAEs. In severe cases, ICI treatments are interrupted or suspended and antiinflammatory treatments are started. 18F-FDG uptake due to IRAEs may mimic metastases or disease progression. Their presence may also help in predicting response to treatment and have prognostic implications. In this review article, we provide basic information about ICI treatments, IRAEs, and 18F-FDG PET/CT findings.
Immune checkpoint inhibitor (ICI) treatments have been increasingly used in oncology in the last 10 years. ICI treatments activate T cells against tumors by blocking inhibitory ICI immunoreceptors or their ligands. Activated T cells attack not only the tumor but also healthy and normal cells, causing an autoimmune reaction in various tissues. These immune-related adverse effects (IRAEs) cause increased uptake on 18F-FDG PET/CT studies due to inflammation in various tissues. 18F-FDG PET has high sensitivity in detecting inflammation and determining its severity and extent. It is important to recognize and report IRAE-related findings on PET images. On the basis of the severity and extent of IRAEs, physicians interrupt or suspend ICI treatment and start steroid or immunosuppressive treatments. The presence and severity of IRAEs may help to predict response to ICI treatment and may have prognostic value, indicating a more favorable prognosis (1–3). Depending on the location, particularly in lymph nodes, IRAE-related uptake may mimic metastases or disease progression, and therefore it is important to be aware of these immune-related side effects. In this review article, we will describe first the ICIs, then the mechanism of autoimmune reactions in patients receiving ICI treatment, and finally the 18F-FDG PET/CT findings.
IMMUNE CHECKPOINT INHIBITORS
Immune checkpoints play an important role in immune regulation. There are various checkpoint molecules (immunoreceptors) on T cells, some of them being inhibitory (suppressing the T cells) and some stimulatory (activating the T cells) (4,5). Tumors or antigen-presenting cells (e.g., macrophages or dendritic cells) have various ligands on their surfaces that bind to inhibitory or stimulatory checkpoint receptors on T cells, resulting in activation or suppression of T cells (5). Activated T cells subsequently kill the microorganisms (viruses, bacteria, fungi, and parasites) and tumors but then can also attack healthy cells, resulting in autoimmune diseases. Suppression of T cells prevents autoimmune diseases but results in reduced protection against microorganisms. The tumor microenvironment can also suppress T cells. In normal conditions, inhibitory immune checkpoint immunoreceptors are activated to prevent T cells from attacking normal tissues.
In the last 10 years, various medications (antibodies) have been developed to block (inhibit) inhibitory checkpoint molecules (immunoreceptors or their ligands) in the treatment of tumors and infection. These medications are called immune checkpoint inhibitors (ICIs). Currently approved ICI medications block cytotoxic T-lymphocyte– associated protein 4 (ipilimumab), programmed death receptor 1 (pembrolizumab, nivolumab), or its ligand (atezolizumab, avelumab, durvalumab, and cemiplimab) (4,6). These medications are approved to be used in the treatment of various cancers such as melanoma (ipilimumab, nivolumab, pembrolizumab), non–small cell lung cancer (pembrolizumab, nivolumab), renal cancer (nivolumab, ipilimumab), and bladder cancer (atezolizumab) (4,6).
Inhibition of cytotoxic T-lymphocyte–associated protein 4 and programmed death receptor 1 or its ligand through ICI treatment activates T cells to kill tumor cells but also causes T cells to target healthy tissues, resulting in IRAEs (autoimmune manifestations). They can also cause a flare of prior autoimmune disease. IRAEs are commonly seen in patients receiving ICI treatments and are dependent on dose and type of ICI treatment and various other factors. IRAEs can be clinically evident or silent and can involve any tissues, resulting in such conditions as encephalitis, hypophysitis, thyroiditis, sarcoidlike reactions, pneumonitis, hepatitis, pancreatitis, adrenalitis, colitis, nephritis, arthritis, and skin manifestations. Most fatalities are seen in cases of encephalitis, myocarditis, pneumonitis, and hepatitis (7). IRAEs can be seen a few weeks to months after starting ICI treatment. Clinical, laboratory, radiologic, and 18F-FDG PET/CT imaging findings can help to diagnose IRAEs. Optimal management of IRAEs varies according to the organ involved and the severity or grade of involvement and includes close monitoring, treatment interruption or suspension, and corticosteroid administration (prednisone or methylprednisolone) (8).
18F-FDG PET/CT IMAGING
18F-FDG PET/CT imaging is used to assess the response to ICI treatment in various tumors, particularly melanoma and non–small cell lung cancer. 18F-FDG PET response patterns in ICI treatment show some atypical patterns different from those seen with other treatments, such as chemotherapy or radiotherapy. This difference occurs because ICI treatments induce an influx of T lymphocytes into the tumor, and these T lymphocytes take up 18F-FDG and subsequently further increase the metabolic activity of the tumor environment (9,10). Immune-related response criteria such as PERCIST or immune RECIST have been established to better assess the response in patients receiving ICI treatments (11,12).
18F-FDG PET–positive IRAEs, such as sarcoidlike syndrome, thyroiditis, hypophysitis, enterocolitis, pancreatitis, hepatitis, pneumonitis, arthritis, enthesitis, and myositis, have been reported in various articles (13,14).
18F-FDG PET is sensitive in detecting early inflammation even before clinical symptoms start and radiologic changes develop (15,16). Cells involved in inflammation actively use glucose, which is the main reason for increased 18F-FDG uptake at inflammatory sites. In addition, increased blood flow and capillary permeability also contribute to increased 18F-FDG activity at inflammation sites; this activity is nonspecific and can be seen with any kind of radiotracer. It has been reported that a significant number of patients with PET-detectable IRAEs are asymptomatic (1,17). Early detection of IRAEs allows early management. Their presence may help predict the response to treatment and indicate a more favorable prognosis (1–3). In a study by Sachpekidis et al., in 10% of patients PET/CT showed sarcoidlike lymphadenopathy as a response to treatment, and these patients showed disease control (2). In another study, 9 patients with IRAE findings on PET had a complete response at the final evaluation (1). Patients with PET-detectable IRAEs had a significantly longer progression-free survival than did those without IRAEs on PET (3).
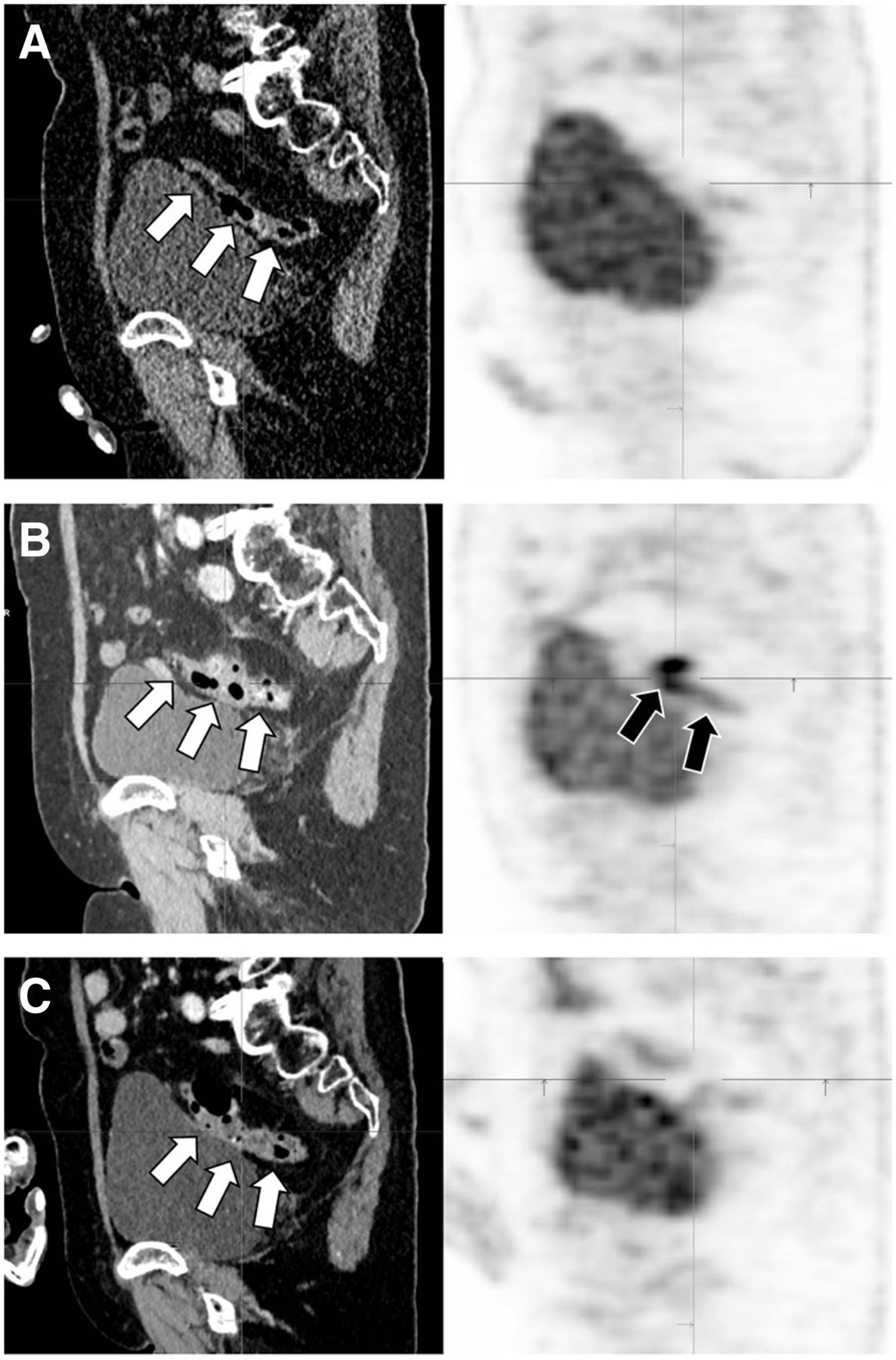
Colitis is one of the most common manifestations of IRAEs. On unenhanced CT as a part of PET/CT, colonic wall thickening and pericolic fat stranding may be seen in association with diffuse or segmental increased 18F-FDG uptake. 18F-FDG PET/CT imaging was reported to be more sensitive than CT in the early detection of colitis as a result of ICI treatment (6,17,18). However, 18F-FDG PET has a low specificity for colitis due to physiologic mucosal, muscular, and luminal activity. In addition, metformin use can induce high bowel activity, and it is recommended that metformin be stopped for 48 h before the 18F-FDG PET study. Figure 1 shows sagittal 18F-FDG PET/CT images of a 71-y-old patient with a history of melanoma. PET/CT before treatment did not show abnormal findings in the sigmoid colon, but PET/CT 4 mo after nivolumab treatment showed thickening in the sigmoid wall, with inflamed diverticula and increased uptake without clinical symptoms. PET 6 mo after discontinuation of nivolumab (treatment change to dabrafenib and trametinib because of disease progression) showed only mild thickening in the sigmoid wall as a late inflammatory residue (fatty infiltration) and only mild uptake.

Selected sagittal 18F-FDG PET/CT images of pelvis. Initial scan before treatment shows normal findings in colon (arrows, A), PET/CT scan 4 mo after nivolumab treatment shows colitis in sigmoid colon (arrows, B), and PET/CT scan 6 mo after discontinuation of nivolumab shows significant reduction in sigmoid activity (arrows, C).
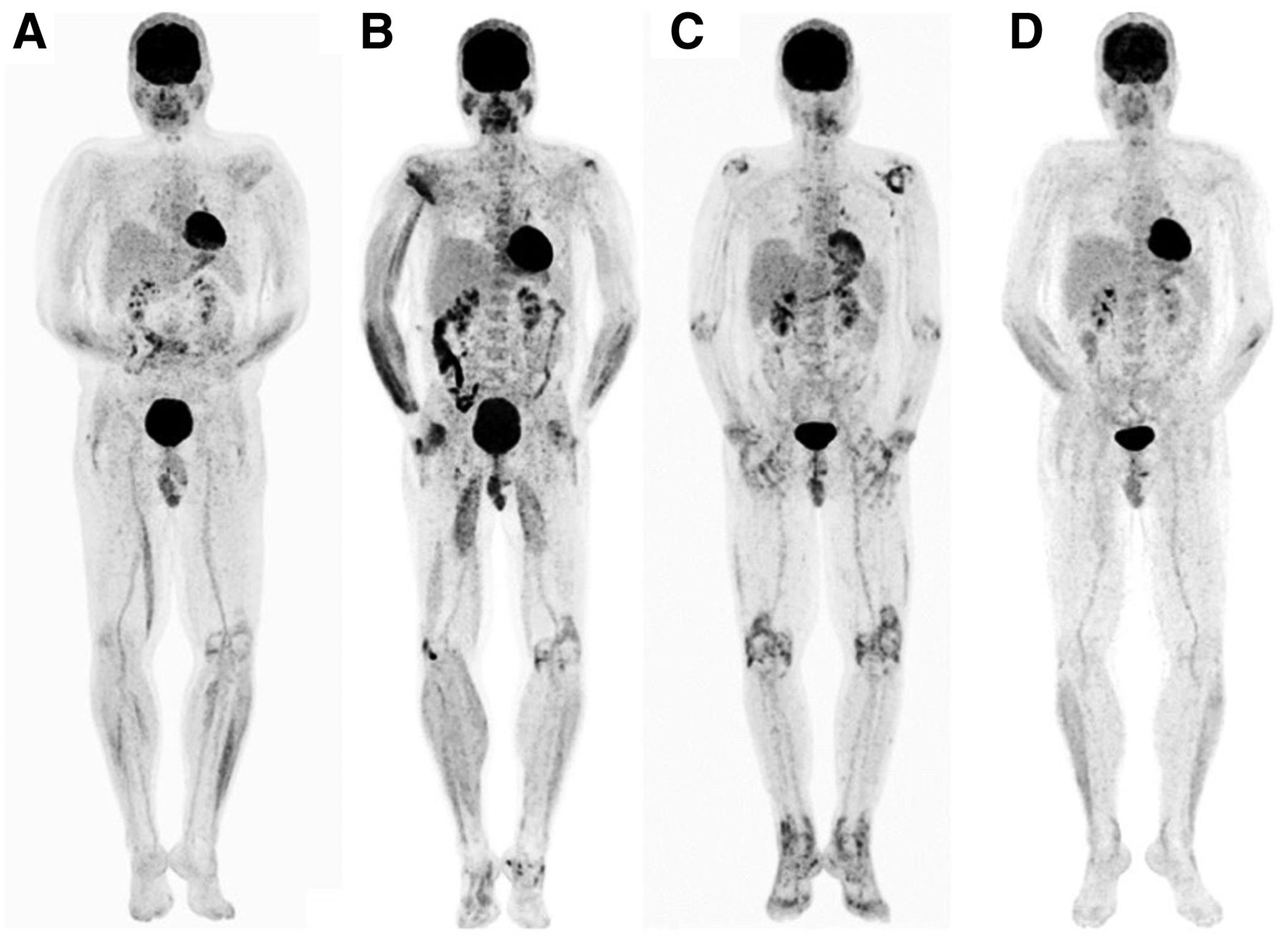
18F-FDG PET has high sensitivity in detecting rheumatologic manifestations of IRAEs such as arthritis, myositis, tenosynovitis, and polymyalgia rheumatica and in determining their extent and severity. Figure 2 shows serial 18F-FDG PET total-body images of a 48-y-old patient with a history of melanoma who received various ICI treatments. A PET image after 22 mo of nivolumab treatment showed mildly increased uptake in the left knee and, bilaterally, in the mediastinal and hilar lymph nodes (sarcoidlike). The patient had no clinical symptoms related to these findings. A PET image after 3 mo of treatment with pembrolizumab (change in therapy due to persistent metastasis in the 12th rib) showed diffusely increased metabolic activity in the muscles of the upper and lower extremities, a finding that indicated myositis because it correlated with clinical findings of swollen arms and legs. The PET image also showed interval slight progression in left knee uptake, mildly increased uptake in the right knee and left ankle, and bowel activity, without clinical signs. A PET image after 2 mo of nivolumab treatment showed markedly and diffusely increased bilateral uptake in all joints of upper and lower extremities. Antibody treatment was stopped, and prednisolone treatment was started by the clinician because of the PET image findings and laboratory and clinical correlation. A PET image 12 mo after stopping nivolumab treatment (steroid treatment stopped 6 mo before PET) showed complete resolution of inflammatory uptake in the joints. No evidence of tumor was seen (complete metabolic response), and the mild sarcoidlike uptake was stable. Figure 3 shows 18F-FDG PET images after 1 mo and 1 y of nivolumab treatment in a 40-y-old patient with a history of melanoma. Before treatment, there was increased uptake in the bone marrow and mild, diffusely increased uptake in the knees. After treatment, there was increased uptake in the interspinous bursae of the lumbar spine, which was highly suggestive of polymyalgia rheumatica, and there was a further increase in uptake in the knees.
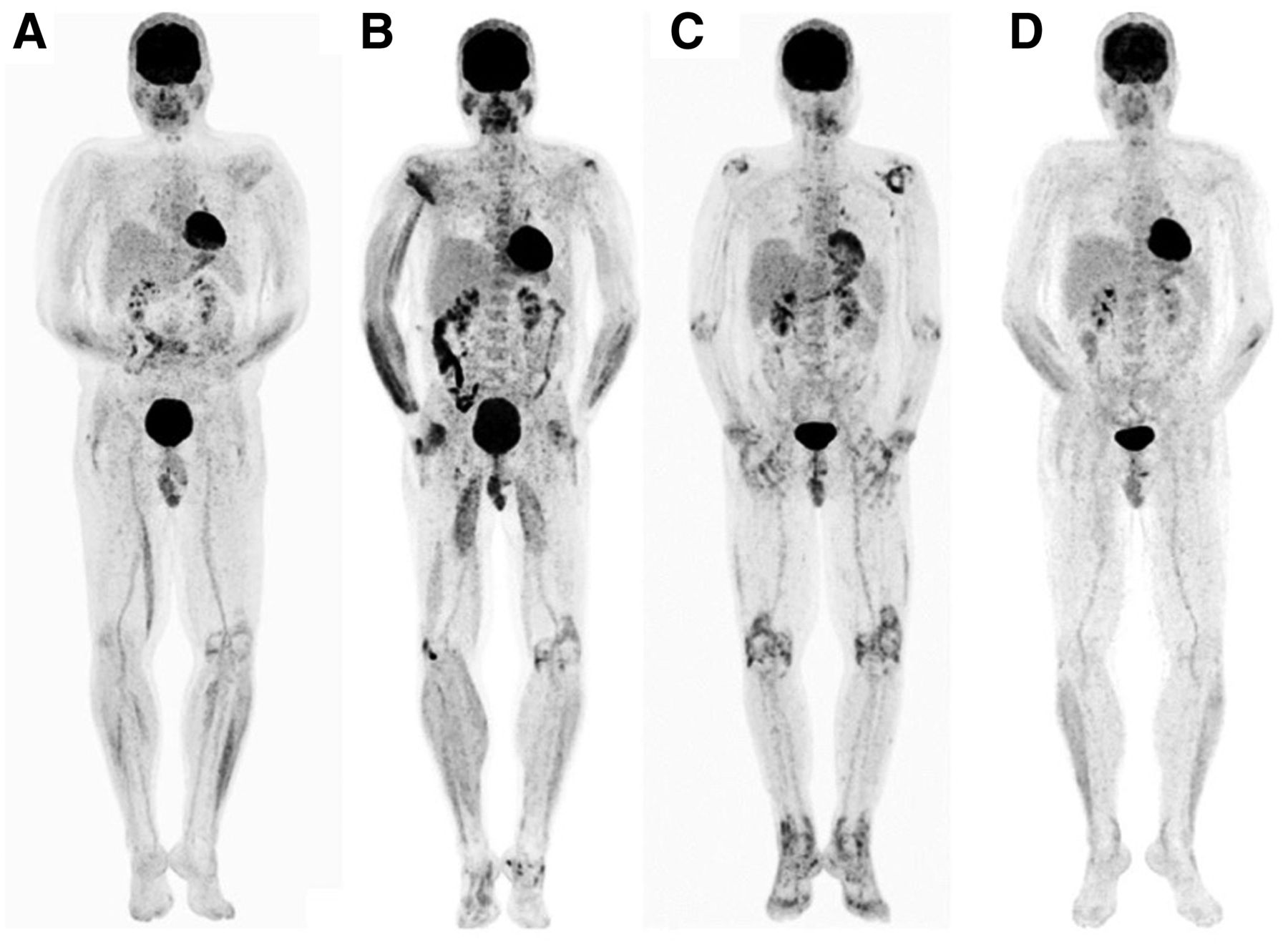
Serial total-body 18F-FDG PET maximum-intensity projections of patient with history of melanoma after treatment with nivolumab (A), pembrolizumab (B), nivolumab (C), and steroids (D). Development, progression, and regression of arthritis are seen, as well as mild sarcoidlike uptake in chest and myositis.

Sagittal total-body maximum-intensity-projection 18F-FDG PET images before (A) and after (B) nivolumab treatment. Increased uptake in lumbar spine is due to bursitis (arrows).
IRAE-related focal areas of uptake or uptake in lymph nodes can mimic metastatic disease or disease progression (19,20). Sarcoidlike reactions may mimic lymph node, lung, and skin metastases. Sarcoidlike reactions are characterized by the presence of noncaseating granulomas. In sarcoidlike reactions, 18F-FDG PET/CT usually shows bilateral symmetric hypermetabolic mediastinal and hilar lymphadenopathy with or without hypermetabolic focal nodular opacities or consolidations in the lungs. Uptake in the portocaval lymph nodes and subcutaneous hypermetabolic nodules due to noncaseating granulomas may also be seen in sarcoidlike reactions (10,21). Figure 4 shows 18F-FDG PET images of a 60-y-old patient with melanoma. A PET image for initial staging showed metastatic disease in the lungs, liver, left adrenal, and mesenteric lymph nodes and diffuse uptake in the stomach due to gastritis from Helicobacter pylori. A PET scan 6 mo after nivolumab treatment showed complete metabolic resolution of most lesions, with some residual tumor in the liver and progression of a left adrenal metastasis. New symmetric hypermetabolic lymph nodes in both hila and mediastinum were likely due to a sarcoidlike reaction. A nivolumab-induced flare in gastric uptake was also seen.
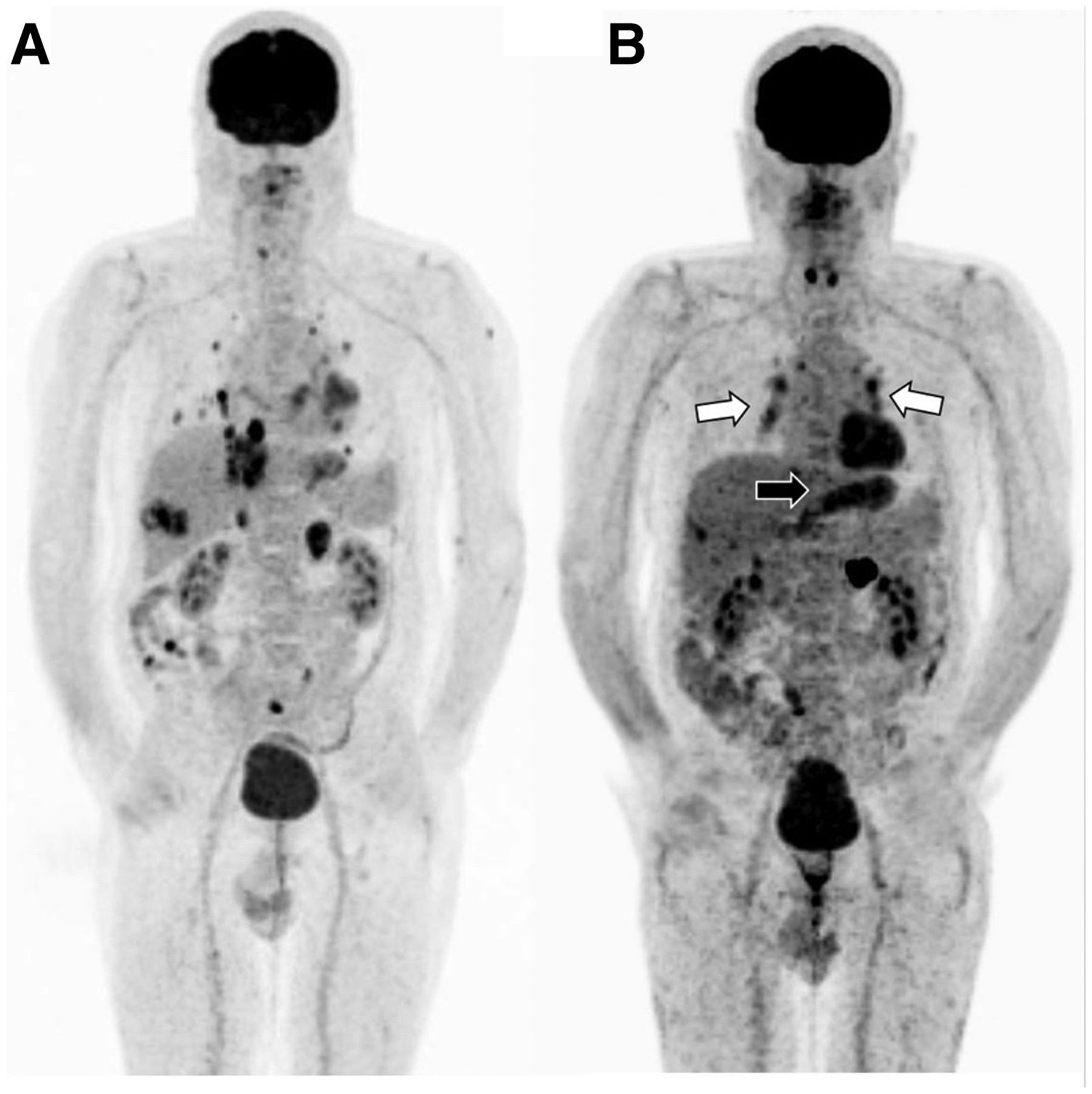
Total-body 18F-FDG PET maximum-intensity-projection images before (A) and after (B) nivolumab treatment in a melanoma case with multiple metastases. Increased bilateral uptake in hilar and mediastinal lymph nodes is due to sarcoidlike reaction (white arrows) and diffuse uptake in the stomach is due to gastritis (black arrow).
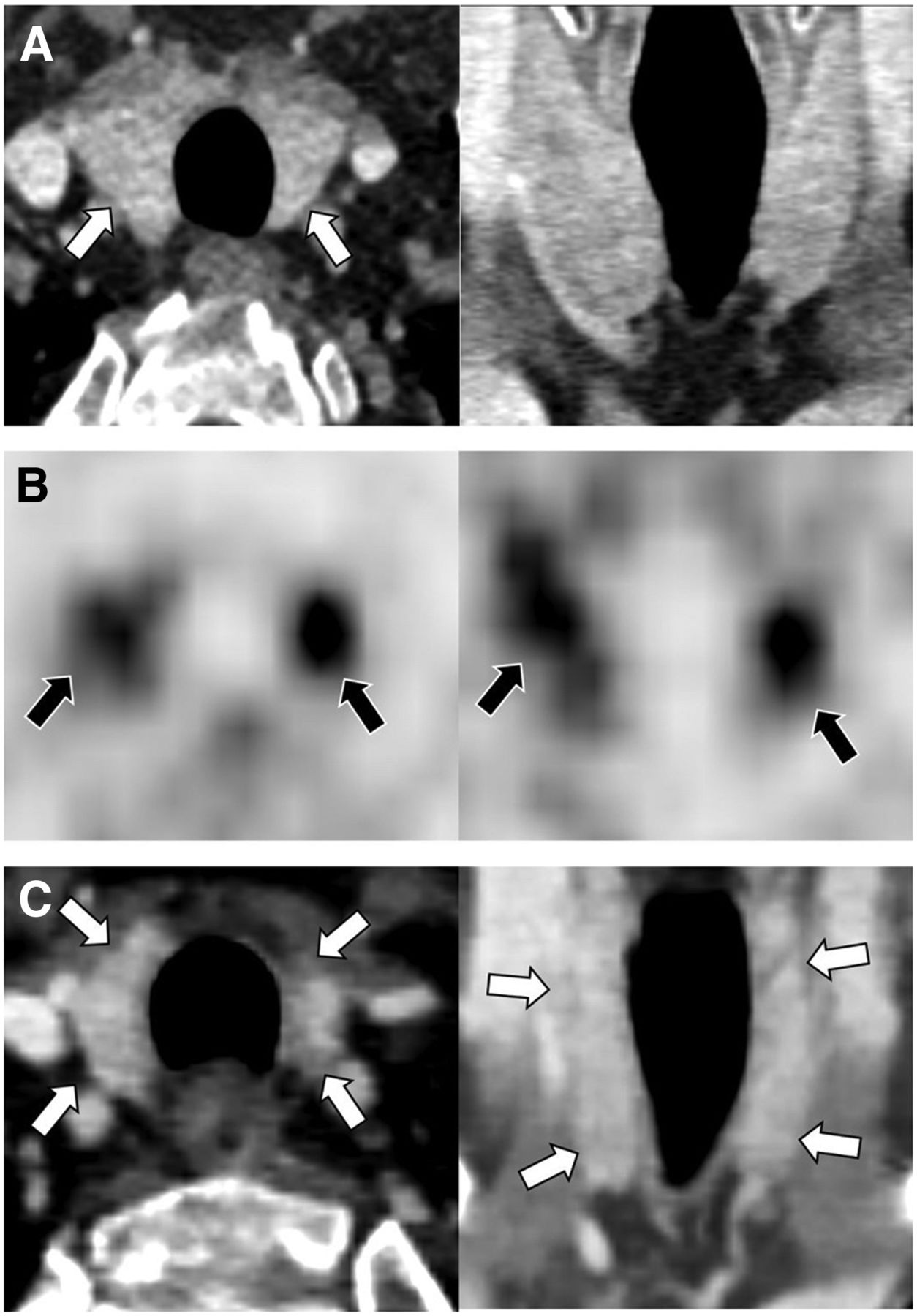
IRAE-related thyroiditis might be acute and transient, with biochemically and clinically accompanying thyrotoxicosis, or progressing to hypothyroidism (22). Selected CT images of a 61-y-old patient with melanoma showed reduction in thyroid size 1 y after treatment with nivolumab, as compared with baseline image (Figs. 5A and 5C). A PET image after the start of nivolumab showed diffusely increased uptake in the thyroid gland, with a cold defect in the lower pole of the right lobe corresponding to a nodule seen on CT. The thyroid-stimulating hormone level was 43 mU/L. Figure 6 shows diffusely increased uptake in the thyroid gland in a 65-y-old patient with a history of melanoma who was treated with nivolumab for 20 mo (whole body). Thyroiditis and hypothyroidism were confirmed by laboratory findings, and patient began taking thyroxine. There was also mild diffusely increased uptake in the liver (SUVmean, 3; SUVmax, 5.2; liver–to–blood-pool SUVmean ratio,1.6) and elevated glutamate dehydrogenase and γ-glutamyl transferase levels, indicating hepatitis. Colonic uptake was due to metformin use. Because of physiologic uptake in the liver, 18F-FDG PET may not show early hepatitis; however, in more severe cases it is possible to see diffusely increased hepatic uptake. ICI treatment–related T-cell activation can induce increased uptake in the spleen (reversal in liver-to-spleen uptake ratio), which may interfere with detection of hepatitis on PET images (10). However, careful visual assessment and obtaining a liver–to–blood-pool SUVmean ratio can help detect hepatitis in such cases. A normal liver–to–blood-pool SUVmean ratio ranges from 1.3 to 1.4 in various reports (23–25). Because the SUVs are affected by body weight and various other factors, the liver–to–blood-pool SUVmean ratio is more accurate than SUVmean alone when assessing the metabolic activity of the liver (25).

Selected transaxial and coronal contrast-enhanced CT images (A and C, before and 1 year after nivolumab treatment, respectively) and PET images (B, with start of nivolumab) in a case with history of melanoma. PET shows diffusely increased uptake in the thyroid due to thyroiditis (arrows), CT shows decrease in thyroid size 1 year after treatment as compared with pretreatment size (arrows pointing to the thyroid gland). Nodule in the right lower lobe is causing cold area on PET.

Total-body 18F-FDG PET image after nivolumab treatment shows diffuse uptake in thyroid gland due to thyroiditis (arrows), mild diffuse uptake in liver due to hepatitis (arrow), and diffuse colonic uptake due to metformin use (arrows) in a case with history of melanoma.
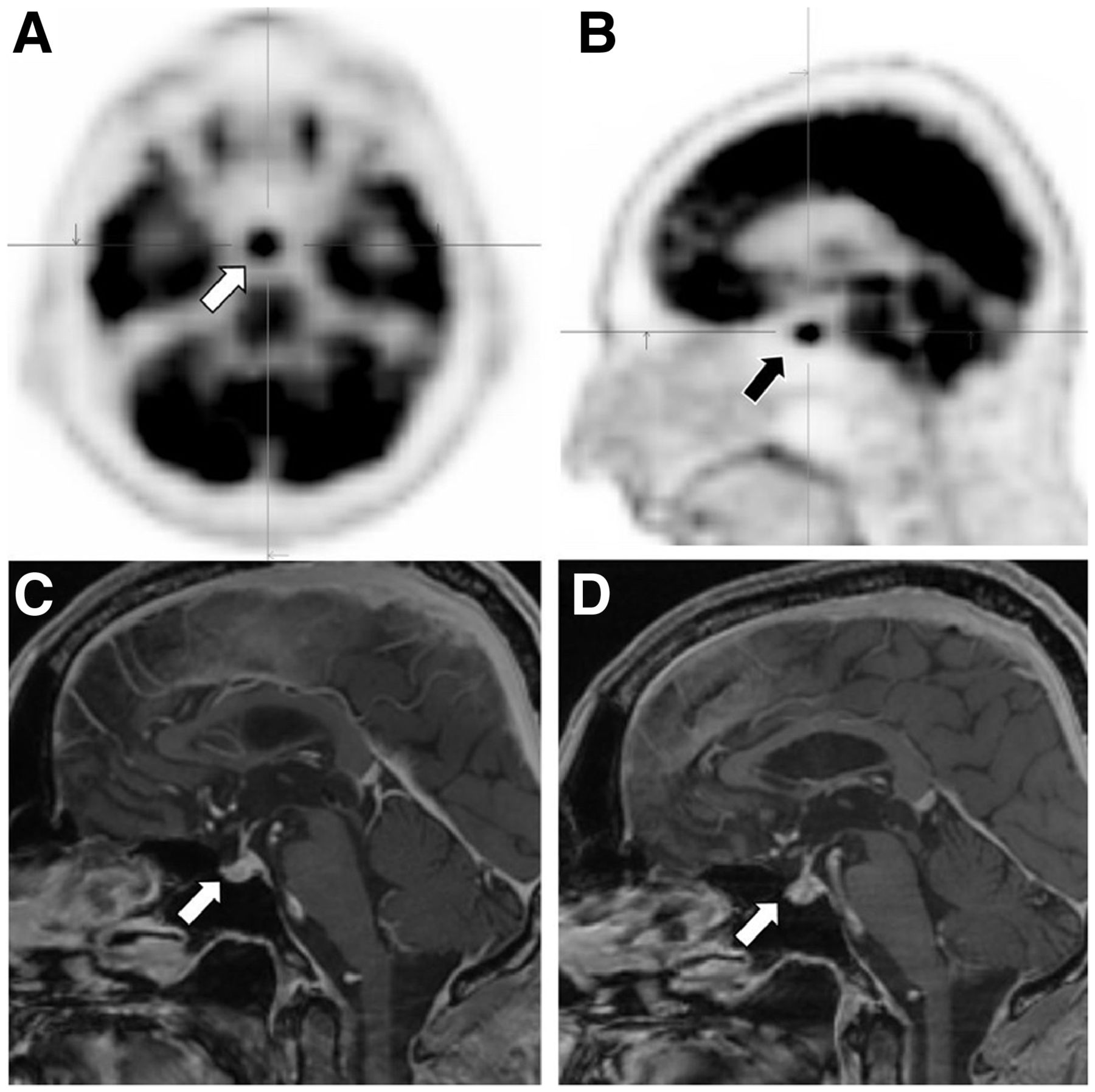
On 18F-FDG PET scans, the normal pituitary gland may show mild uptake. Prominent uptake in the pituitary gland could be from hypophysitis, but pituitary adenomas or metastasis should be ruled out by a clinical, laboratory, and radiologic assessment. Figure 7 shows increased uptake in the pituitary gland in a 61-y-old patient with a history of melanoma who was treated with nivolumab (pituitary-to-frontal SUVmax ratio was 1, as compared with 0.3 in a patient with normal uptake in the pituitary gland). Laboratory values did not show pituitary insufficiency, but MRI after 3 mo of therapy showed a swollen, inhomogeneously enhancing hypophysis with a thickened hypophyseal stalk, indicative of hypophysitis, as compared with pretreatment MRI, which showed a typical flat, homogeneously enhancing hypophysis after contrast administration (26).

Selected transaxial and sagittal 18F-FDG PET images (A and B) and sagittal MR images (C and D, before and after treatment, respectively) show findings consistent with hypophysitis (arrows).
18F-FDG PET/CT has a high sensitivity in determining the severity (grade) and extent of inflammation in certain tissues such as joints and colon—information that is important in the management of patients starting steroid treatment and interrupting or suspending ICI treatment. However, care should be taken when assessing inflammation or tumors in patients who are receiving or recently received high-dose steroid treatment, as such treatment may cause a false-negative 18F-FDG PET result or may underestimate the metabolic activity of inflammation or tumors (27,28).
In routine oncologic studies, 18F-FDG PET imaging cannot accurately assess myocardial inflammation because of various degrees of physiologic myocardial uptake. If there is clinical concern about myocarditis, a cardiac 18F-FDG PET imaging protocol or cardiac MRI is used to demonstrate myocardial involvement (29,30).
Pelvicalyceal excreted activity may limit evaluation of the kidneys, but in renal involvement, focal or diffuse renal parenchymal 18F-FDG uptake may be seen in a careful assessment of images (31). In addition, delayed PET imaging can help to better assess renal parenchymal involvement.
18F-FDG PET is also limited in assessing the brain because of physiologic high uptake in the gray matter. In encephalitis, diffusely decreased and heterogeneous uptake may be seen. In limbic encephalitis, increased uptake may be seen in one or both mesial temporal lobes. PET/MRI or MRI of the brain can further help identify brain involvement; in particular, MRI T2-weighted fluid-attenuated inversion recovery sequences are very sensitive in inflammation (32,33).
Potential skeletal adverse effects related to immune checkpoint inhibitors have been reported as bone fractures and resorptive or destructive bone lesions due to localized inflammation, such as sterile osteitis, leading to osteoclast activation and bone resorption (34). These changes can cause increased uptake in the bones on 18F-FDG PET, but no cases have yet been reported.
CONCLUSION
ICI treatment–related autoimmune adverse effects are common. It is important to recognize and report findings of IRAE-related adverse effects on 18F-FDG PET scans.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: What is the importance of recognizing findings of ICI treatment–related adverse effects on 18F-FDG PET scans?
PERTINENT FINDINGS: IRAEs are commonly seen in patients receiving ICI treatments and cause increased uptake in various tissues on 18F-FDG PET studies.
IMPLICATIONS FOR PATIENT CARE: Recognizing IRAEs on PET scan is important, as their presence and severity alert physicians to the need to interrupt or suspend ICI treatment and start antiinflammatory treatment. Their presence may also help in predicting the response to treatment. Being aware of IRAE-related uptake on 18F-FDG PET scans also prevents false-positive results for metastasis or disease progression.
Footnotes
Published online July 30, 2021.
REFERENCES
- Received for publication February 17, 2021.
- Revision received May 20, 2021.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}