


Abstract
The breast is an unusual site for metastasis from malignant tumors, although it may be the first manifestation of an extramammary primary malignancy typically arising in the lung, skin (melanoma), ovary, or lymph nodes (lymphoma). Breast metastasis from thyroid carcinoma is extremely rare and may take years to develop, as differentiated thyroid carcinoma is usually indolent and slow-growing and metastasizes to the lymph nodes, lungs, and bones. Here, we present the case of a middle-aged woman (after subtotal thyroidectomy for multinodular goiter 24 y previously) showing discordant 18F-FDG and iodine avidity in proven metastatic disease involving the lymph nodes, bones, spleen, and breast on whole-body 131I and 18F-FDG scans due to tumor heterogeneity.
Metastatic involvement of the breast is unusual, with an incidence of 0.5%–2.0%, when the primary tumor is a lung malignancy, a melanoma, or a hematologic malignancy, apart from the contralateral breast (a primary tumor in one breast that metastasizes to the other breast) (1). Separate primary malignancies may occur in thyroid and breast in a synchronous or metachronus fashion (2). However, breast metastasis arising from a thyroid primary is very uncommon.
CASE REPORT
A 55-y-old woman, who 24 y previously had undergone subtotal thyroidectomy for multinodular goiter and had been on levothyroxine replacement treatment since that time, presented with a low backache of 10-mo duration. MRI of the spine showed a large soft-tissue mass at the level of the L5–S1 vertebrae, and the histopathologic diagnosis on a fine-needle aspiration sample was metastatic follicular thyroid carcinoma. The biochemical profile showed a normal serum level of thyroid-stimulating hormone (0.9 μIU/mL; reference range, 0.5–4.5 μIU/mL) and elevated levels of thyroglobulin (>1,000 ng/mL; reference range, 0–55 ng/mL) and antithyroglobulin (938.6 IU/mL; reference range, 0–125 IU/mL). A diagnostic radioiodine planar scan of the whole body and a SPECT/CT scan of the neck and thorax were done after administration of an oral dose of 74 MBq (∼2 mCi) of 131I. Iodine-avid widespread metastatic disease and a non–iodine-avid right-breast lesion were seen on the planar, SPECT/CT, and CT images (Fig. 1).
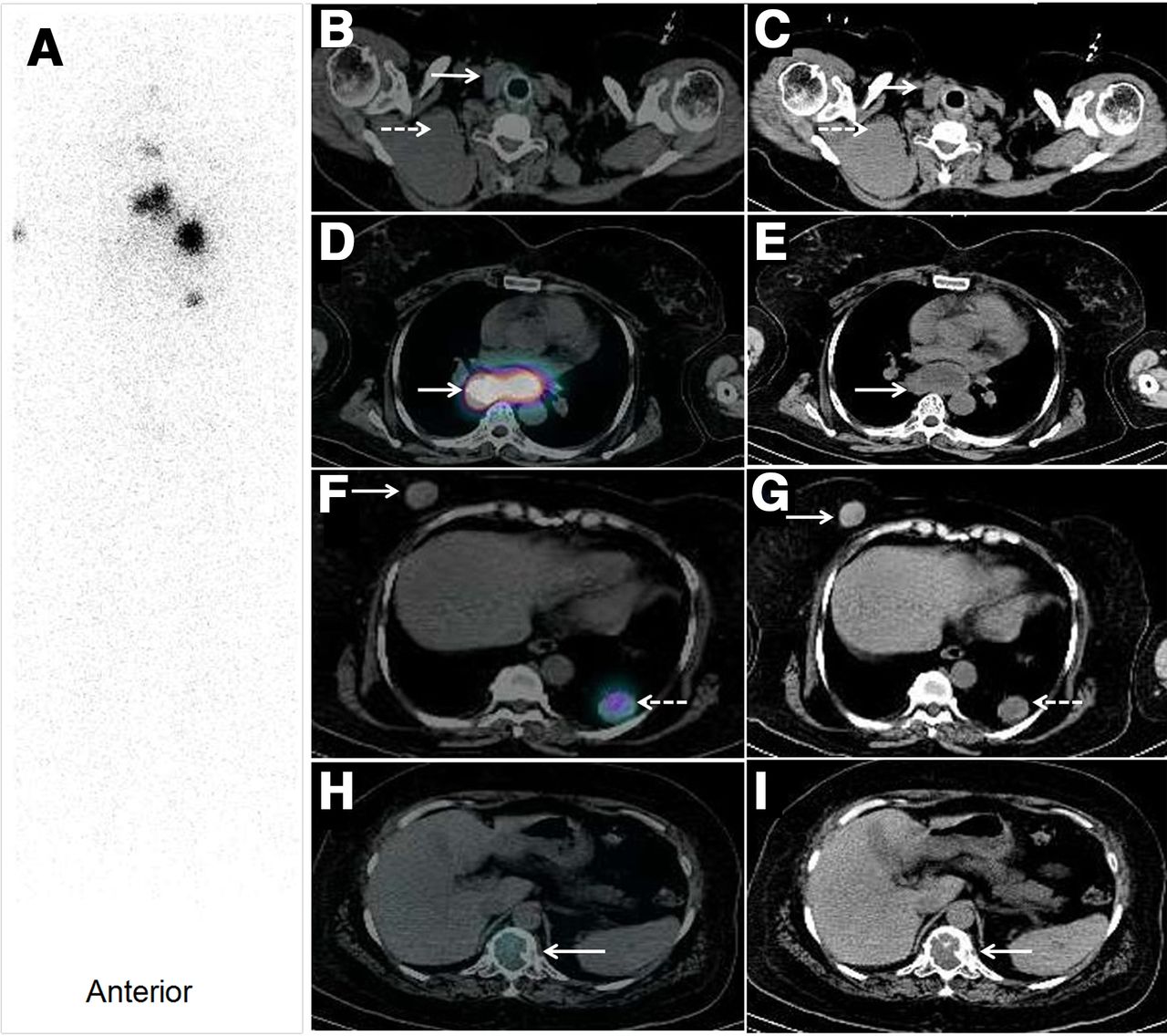
Whole-body radioiodine planar (A), transaxial SPECT/CT (B, D, F, and H), and CT (C, E, G, and I) images showing iodine-avid residual tissue in thyroid bed (B and C, solid arrows), multiple cervical and mediastinal lymph nodes (D and E, arrows), bilateral lung nodules (F and G, dashed arrows), and a few non–tracer-avid cervical lymph nodes (B and C, dashed arrows), right-breast lesions (F and G, solid arrows), and skeletal lesions (H and I, arrows).
In view of the presence of both iodine-avid and non–iodine-avid lesions and the markedly elevated thyroglobulin levels, 18F-FDG whole-body PET/CT (Fig. 2) was done to identify the disease extent and characterize the lesions. This scan showed—in the right breast, the spleen, the skeleton, and the cervical lymph nodes—18F-FDG–avid lesions that were nonavid on the iodine scan. Mammography revealed a lesion in the parenchyma of the right breast (category 4 in the Breast Imaging Reporting and Data System), without involvement of the contralateral breast. A fine-needle aspiration sample from the breast lesion revealed metastatic follicular carcinoma of the thyroid based on cytopathologic features and thyroglobulin levels from the washout sample (Fig. 3). The patient received 7,400 MBq (∼200 mCi) of radioiodine therapy in view of the iodine-avid widespread metastatic disease, though the breast lesion remained non–tracer-avid on the posttherapy iodine scan, confirming its radioiodine-refractory nature.

Maximum-intensity-projection PET image (A) and transaxial PET/CT images (B, C, and D) showing 18F-FDG–avid lesions in right breast (B, arrow; SUVmax, 3.6), spleen (C, arrow), and D12 vertebra (D, arrow) (nonavid on whole-body iodine scan).
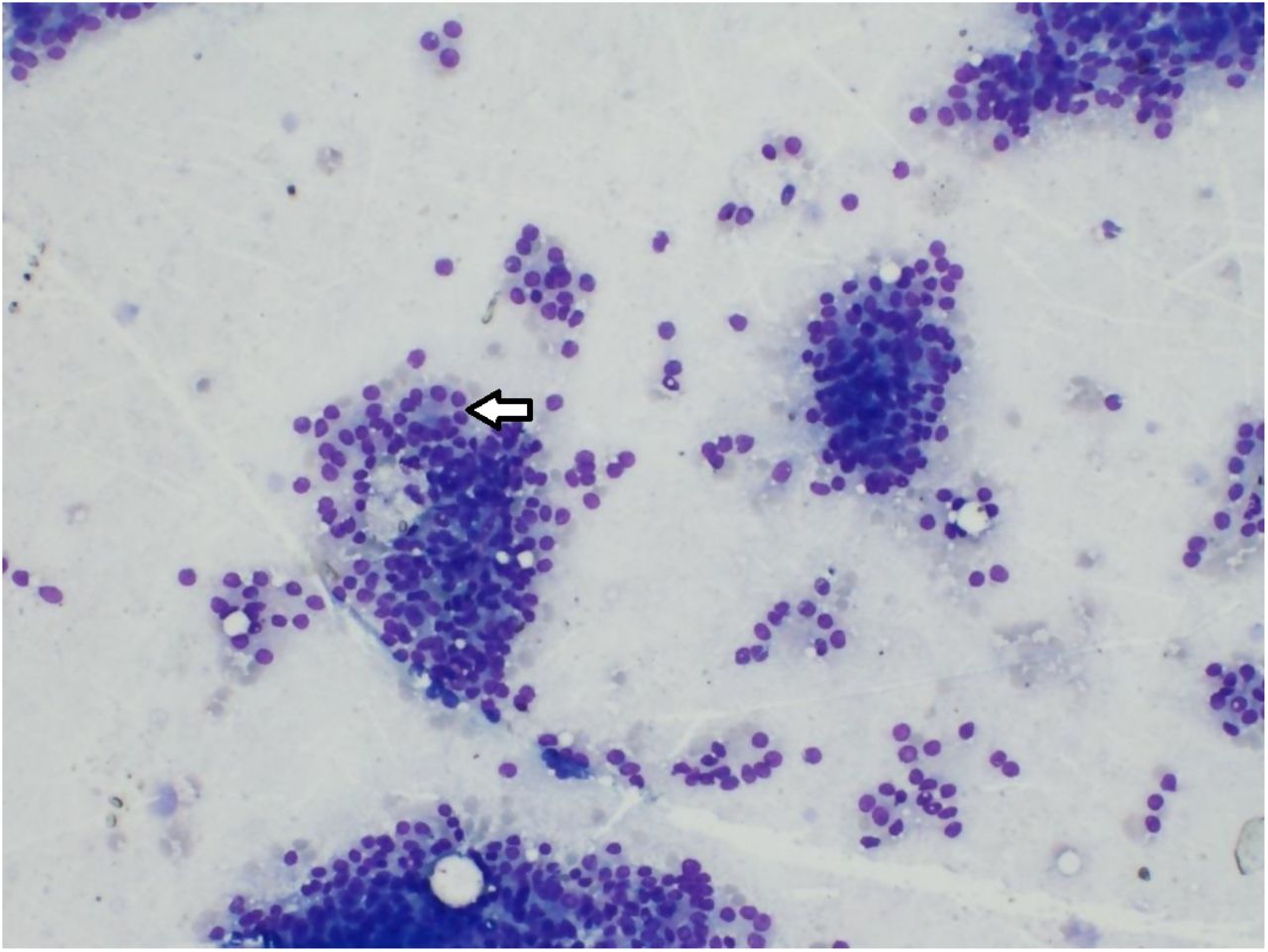
Photomicrograph of sample from fine-needle aspiration of right-breast lesion showing monomorphic tumor cells arranged in microfollicles (May-Grünwald-Giemsa stain, ×100; arrow), suggestive of metastatic follicular carcinoma from thyroid.
DISCUSSION
Metastasis of differentiated thyroid cancer to the breast is extremely rare, with only a few isolated cases being reported in the literature (3,4). There are no clinical or mammographic parameters that can indicate whether a malignant breast lesion is a secondary manifestation of a separate primary tumor. As in our patient, heterogeneity in iodine and 18F-FDG uptake may correspond to varied degrees of differentiation, as glucose metabolism is inversely related to iodine uptake, and 18F-FDG PET/CT has an established role in the detection of iodine-negative recurrent or metastatic disease. Cytologic or histopathologic examination of fine-needle aspiration samples of the breast lesion after immunohistochemistry is the mainstay for diagnosis and for differentiating primary from secondary lesions (5).
CONCLUSION
Management of primary breast lesions is entirely different from that of secondary breast lesions arising from thyroid carcinoma. The widespread disease with tumor heterogeneity in this index case was appreciated on 2 different functional imaging modalities, though precise sampling was essential for diagnosis and appropriate therapy.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online March 15, 2021.
REFERENCES
- Received for publication October 26, 2020.
- Accepted for publication January 27, 2021.
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.