


Abstract
Altered biodistribution can be a source of diagnostic error in the interpretation of nuclear medicine studies. This case reports an instance of increased liver and spleen uptake with 99mTc-dimercaptosuccinic acid believed to be a result of chlorhexidine-mediated colloid labeling. This finding underscores the principle that certain constituents of antiseptics may adversely affect the purity of radiopharmaceuticals during their preparation.
99mTc-dimercaptosuccinic acid (DMSA) is a renal cortical binding agent used for the evaluation of renal parenchymal abnormalities such as renal cortical scarring. It has been suggested that certain constituents of antiseptics used during preparation of 99mTc-DMSA, including chlorhexidine, may interact with the DMSA molecules to form 99mTc-labeled colloid particles (1). The colloid particles are subsequently extracted by the reticuloendothelial system, leading to increased hepatic and splenic uptake. Yet, to our knowledge, there has been only a single case report illustrating this phenomenon since it was first described over 2 decades ago (2). Herein, this case presents diffusely increased liver and spleen 99mTc-DMSA uptake likely secondary to chlorhexidine-mediated colloid labeling. Recognition of this pattern of activity with 99mTc-DMSA is important not only to provide an accurate clinical impression but also to emphasize that improper technique with antiseptics may be a source of radiochemical impurity.
CASE REPORT
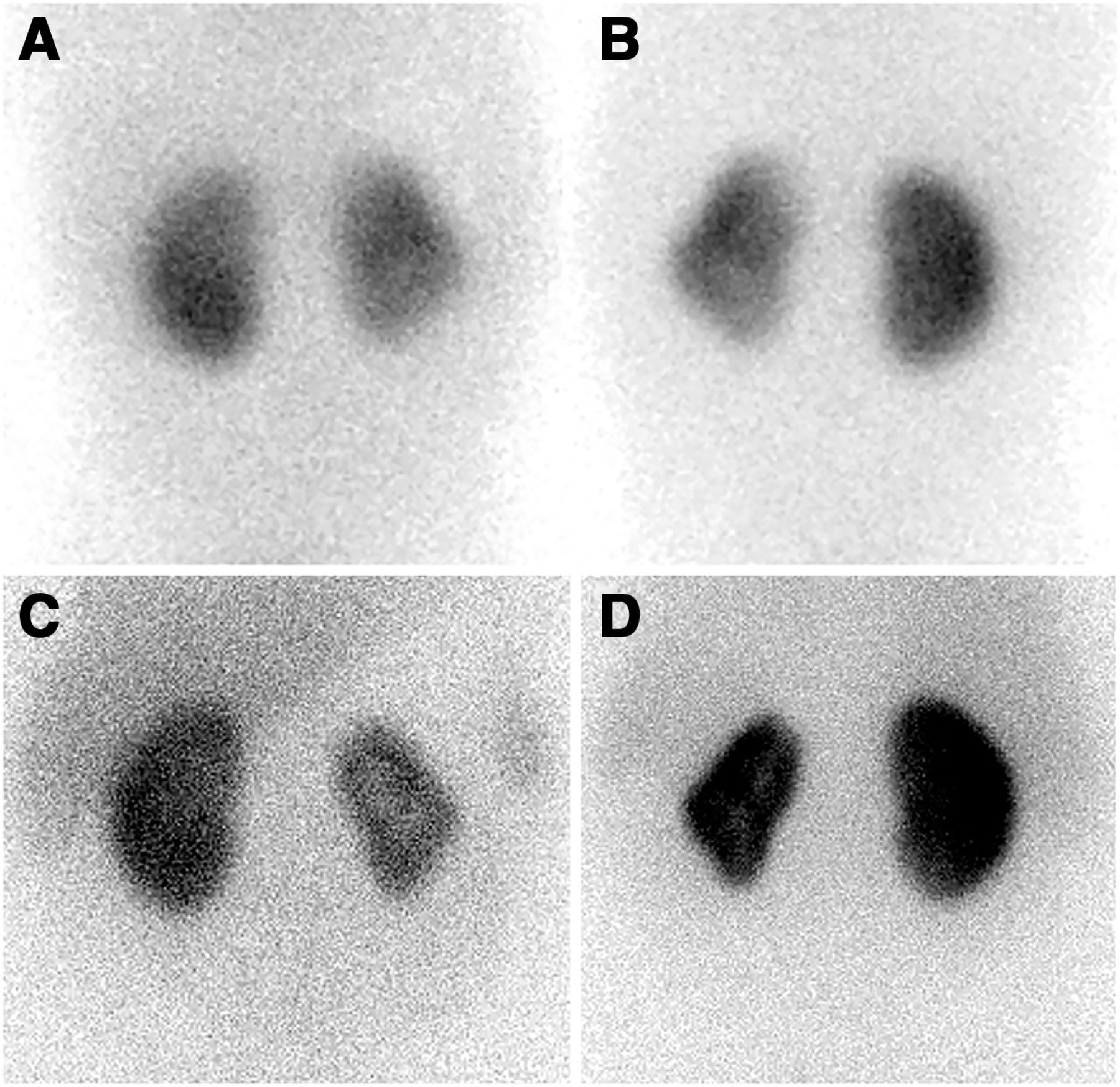
The patient was initially diagnosed with grade II left vesicoureteral reflux via a fluoroscopic voiding cystourethrogram at 5 mo old after multiple renal cysts were incidentally noted on spine MRI. There was no reported history of urinary tract infections, and laboratory values at the time were within normal limits. One year later, a follow-up voiding cystourethrogram showed resolution of the vesicoureteral reflux. A subsequent 99mTc-DMSA scan showed a small left kidney with multiple areas of probable renal cortical scarring (Figs. 1A and 1B). Annual ultrasounds continued to show a size discrepancy between the kidneys. When the patient was 13 y old, a repeat 99mTc-DMSA scan was ordered because of a transfer of care to reevaluate this size discrepancy. The repeat scan showed a similar pattern of renal cortical uptake in the small left kidney; however, mild diffuse activity throughout the liver and spleen was also observed (Figs. 1C and 1D). At the time of the scan, the patient was asymptomatic; laboratory values were normal, with a creatinine of 0.7 mg/dL; and the only reported medication was polyethylene glycol (GlycoLax; SRZ Properties, Inc.), as needed, which prompted us to further investigate the etiology of abnormal uptake. The institutional review board approved this study, and the requirement for informed consent was waived.

(A and B) Anterior (A) and posterior (B) 99mTc-DMSA images obtained in a 20-mo-old child showing a small left kidney with probable areas of superior and inferior pole scarring. A dromedary hump is also seen on the left kidney, and is most consistent with an anatomic variant based on correlation with ultrasound. (C and D) Anterior (C) and posterior (D) scintigraphic images obtained in the same patient at 13 y old, showing a similar appearing small left kidney, but now with mild diffuse radiotracer activity throughout the liver and spleen.
DISCUSSION
Increased hepatic and splenic activity with 99mTc-DMSA has been shown to occur in the setting of several disease processes, including acute renal failure, mononucleosis, and hepatic steatosis (3). Impurities should also be considered a potential source of altered biodistribution, particularly when the patient is otherwise healthy and laboratory values are normal (2,4). While investigating the source of altered biodistribution in this case, we discovered that the technologist failed to let the antiseptic used to sterilize the rubber stopper on the supplied DMSA vial dry completely before reconstituting it with 99mTc. We believed contamination with chlorhexidine was the likely source of altered distribution when considering the constellation of otherwise normal clinical findings, medication review, and lot verification of DMSA with the manufacturer.
CONCLUSION
As new antiseptic formulations are introduced for clinical use, it is important for technologists and nuclear medicine practitioners to be aware that certain constituents may adversely affect the purity of radiopharmaceuticals and, subsequently, result in an atypical biodistribution of the radiotracer. When preparing DMSA, ethanol could be considered an alternative antiseptic if not routinely used in a clinical practice.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online March 15, 2021.
- Received for publication October 4, 2020.
- Accepted for publication January 27, 2021.
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.