


Abstract
The ALSYMPCA trial of the α-emitter 223Ra in symptomatic bone-predominant metastatic castration-resistant prostate cancer (mCRPC) reported a median overall survival (OS) of 14.9 mo, versus 11.3 mo for placebo. However, subsequently reported real-world experience with 223Ra in smaller mCRPC patient cohorts has appeared less successful. We performed a retrospective observational study to review our own 223Ra experience at West Virginia University (WVU). Methods: Demographic, clinical, laboratory, and imaging data were reviewed in all bone-predominant mCRPC patients treated with 223Ra at WVU from 2014 to 2019. The number of bone metastases per patient at the start of treatment with 223Ra was quantified via nuclear bone scans (12 scans, 5 of which also included SPECT/CT), body CT scans (8 scans), and PET/CT scans (4 scans). Standard descriptive statistics were used to study institutional review board–exempted, deidentified patient data. Median survival in ALSYMPCA and WVU patients was compared using a 2-sided, 1-sample log-rank test based on the exponential distributions. The primary endpoint was patient OS after initiating 223Ra. Results: Twenty-four patients received 98 infusions of 223Ra; 83% of these patients were referred from outside WVU. Before the first infusion, all 24 had received androgen deprivation therapy. In total, 73 sequential combinations of androgen deprivation therapy were used, 68 of which (93%) preceded the first 223Ra infusion. Also, before 223Ra, 19 (79%) patients had received docetaxel and 19 (79%) had received 33 courses of radiation, 24 of which targeted nonprostatic sites. Eleven patients (46%) completed all 6 planned 223Ra infusions; 13 (54%) stopped early because of clinical deterioration. As of August 2020, only 1 patient remained alive after completing 6 cycles of 223Ra. Median OS from the first 223Ra infusion to the last follow-up or death was 8.3 mo (range, 0–44 mo)—nearly 50% less than the ALSYMPCA median survival of 14.9 mo (P = 0.01). Compared with ALSYMPCA, more WVU patients received bisphosphonates and docetaxel, more had an Eastern Cooperative Oncology Group performance status of at least 2, more used opiates for pain, more had a greater bone metastasis burden by imaging, and more had lower hemoglobin, albumin, alkaline phosphatase, and prostate-specific antigen levels. Conclusion: Although the science supporting the development and clinical use of 223Ra is compelling, optimal clinical benefit will likely require earlier referral for 223Ra, before patients have exhausted most conventional therapies. At WVU, we found that practically all our referred patients had androgen deprivation therapy, radiation, and cytotoxic therapy before starting 223Ra. We continue to offer 223Ra therapy to patients with symptomatic bone-predominant mCRPC but are encouraging earlier patient referral.
Prostate cancer is the second commonest cancer in men, with an estimated 174,650 new cases and 31,620 deaths in 2019 in the United States (1). Prostate cancer patients with bone metastasis frequently experience skeleton-related events, including pathologic fractures, hypercalcemia, spinal cord compromise, and pain requiring surgery, radiotherapy, and other interventions (2).
A large multicenter, randomized, placebo-controlled phase 3 trial of 223Ra in metastatic castration-resistant prostate cancer (mCRPC) (ALSYMPCA trial) with positive results led to subsequent approval of 223Ra by the U.S. Food and Drug Administration to treat symptomatic bone metastasis in patients with mCRPC with no known visceral metastasis (3). The median overall survival (OS) was 14.9 mo in patients who received 223Ra, versus 11.3 mo in those receiving placebo, a 30% reduction in the risk of death in 223Ra patients versus placebo. Also, the time to the first symptomatic skeleton-related event was significantly prolonged in patients receiving 223Ra (3).
However, postapproval real-world experience with 223Ra in mCRPC has often found shorter median survival and greater complication rates than reported by the ALSYMPCA trial (4–19).
We decided to perform our own retrospective observational study of our clinical experience with 223Ra in mCRPC patients referred to the WVU Cancer Center.
MATERIALS AND METHODS
Demographic, clinical, and laboratory data were collected from electronic medical records (Epic) for every patient with prostate cancer who received 223Ra during a 5-y period beginning in 2014. No patient who received any 223Ra at West Virginia University (WVU) during this period was excluded. Because we could not retrieve several outside-laboratory results for one of the patients, laboratory data from that patient were not analyzed. A nuclear radiologist who administered the 223Ra reviewed nuclear bone scans, nuclear SPECT/CT scans, and PET scans to quantify the number of bone metastases in each patient at the start of 223Ra. Imaging included 12 nuclear bone scans (5 of which also included SPECT/CT), 8 body CT scans, and 4 PET/CT scans. Patient parameters were compared with those published from the ALSYMPCA trial patients who received 223Ra (Tables 1–3) (3).
Baseline Patient Characteristics
Baseline Laboratory Data
Baseline Bone Metastasis and Radiation Data
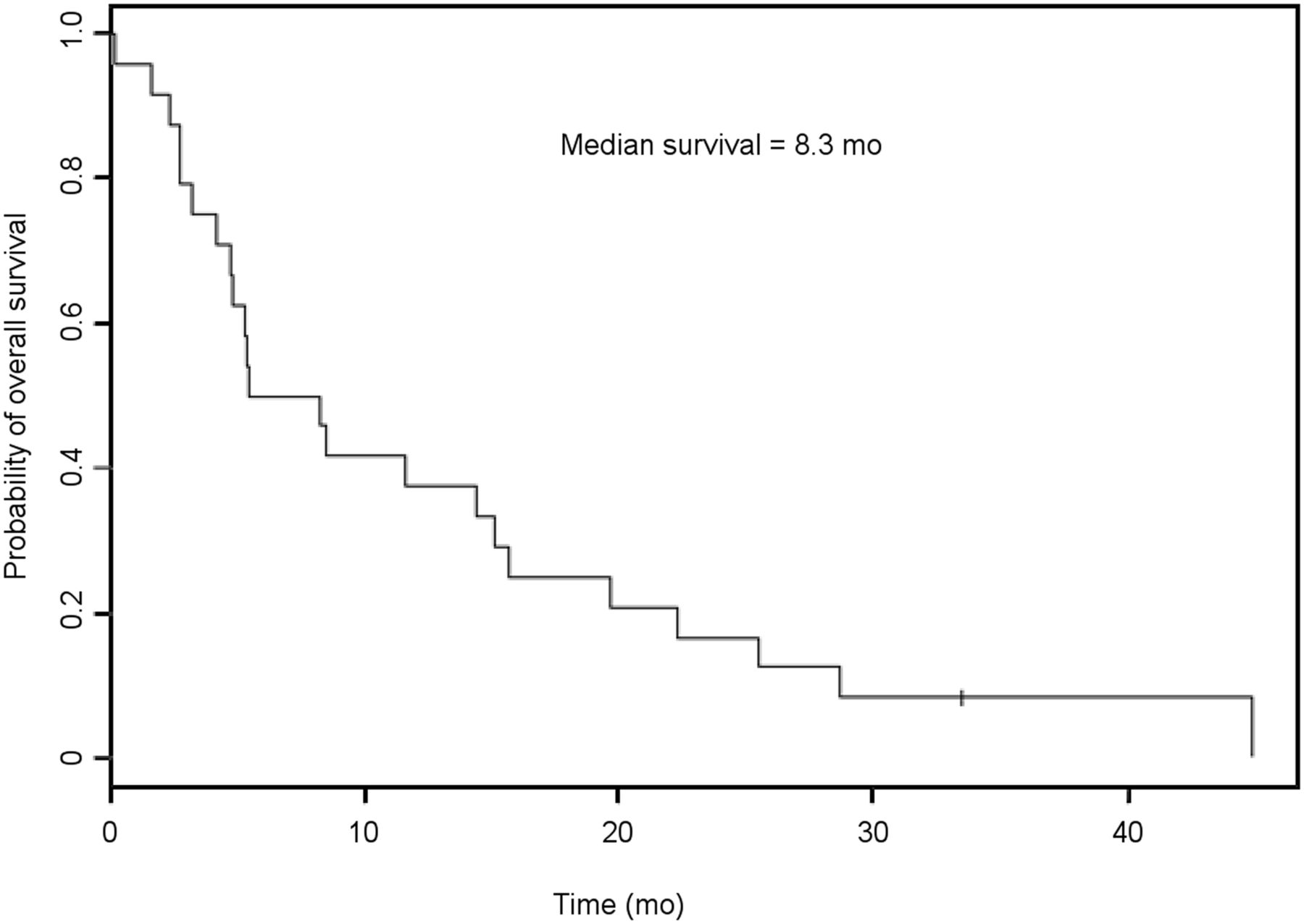
Standard descriptive statistics (mean, median, minimum, maximum, and range) were used to study institutional review board–exempted, deidentified patient data. Median survival in ALSYMPCA and WVU patients was compared using a 2-sided, 1-sample log-rank test based on exponential distributions. The primary endpoint was WVU patient survival from the start of the 223Ra infusions, calculated using the Kaplan–Meier method (Fig. 1).
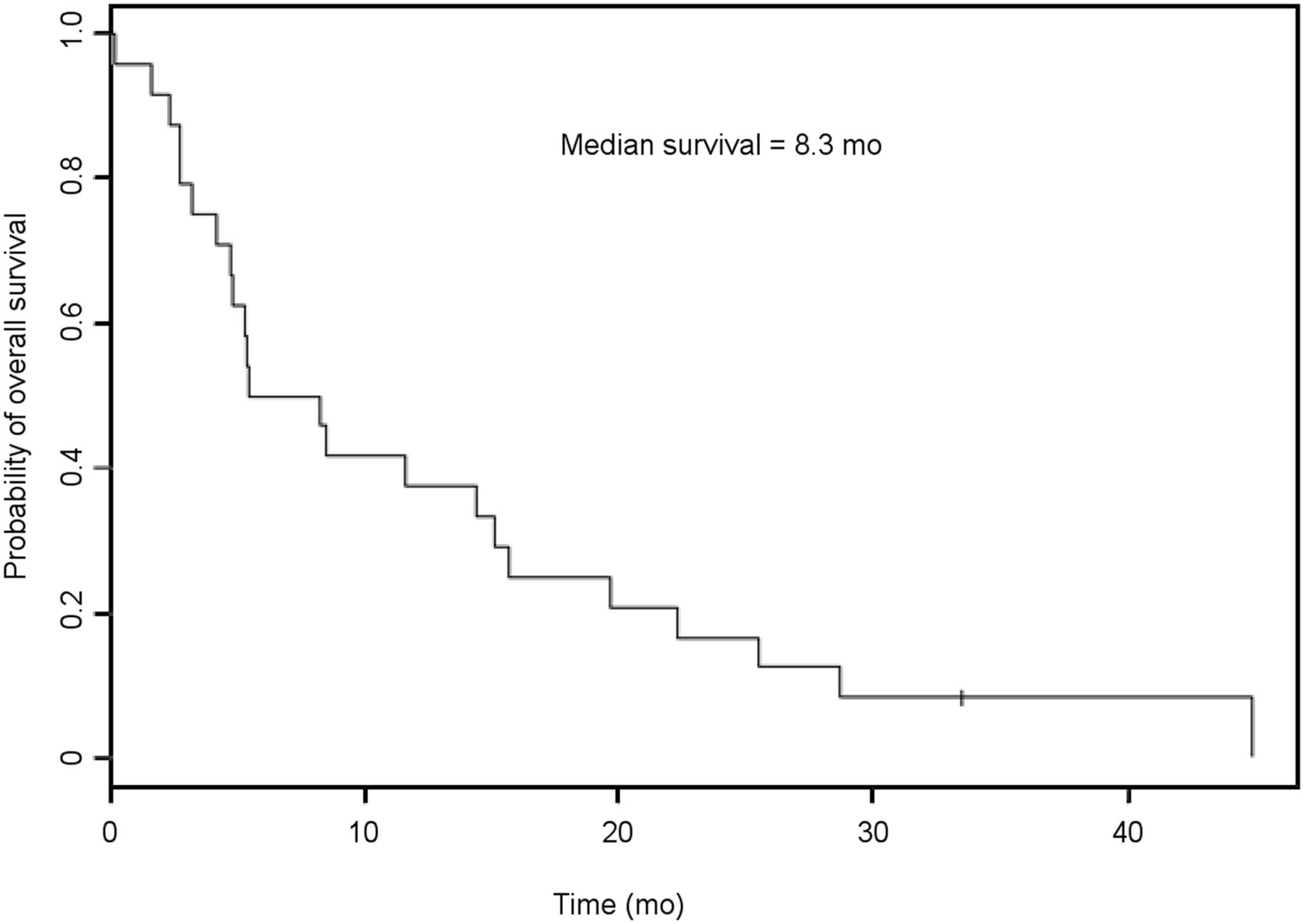
Kaplan–Meier OS of 24 prostate cancer patients at WVU hospital from time of first 223Ra isotope infusion.
RESULTS
Over a 5-y period, 24 patients received 98 total monthly infusions of 223Ra. All patients resided in West Virginia, and 83% were referred from oncology practices outside WVU.
At the initial cancer diagnosis, before 223Ra, only 4 patients (17%) had disease localized to the prostate and 12 (50%) were TNM classification M1/stage 4. At the time of the first 223Ra infusion, the median age was 68 y (range, 54–89 y), and the median prostate-specific antigen value was 75.4 ng/mL (range, 1.5–928.1 ng/mL).
The 24 mCRPC patients received, in total, 73 sequential combinations of androgen deprivation therapy, including abiraterone (with prednisone), bicalutamide, degarelix, finasteride, leuprolide, megestrol, enzalutamide, or estrogen patches. All 24 patients received 1 or more trials of various androgen deprivation therapies (100%), 22 received 2 or more (92%), 17 received 3 or more (71%), and 10 received 4 or more (42%). Ninety-three percent of all the different types of androgen deprivation therapy administered preceded the first infusion of 223Ra.
Eighteen patients (75%) received docetaxel chemotherapy before 223Ra, and 8 of these had 2 or more chemotherapy agents before 223Ra. Nineteen patients (79%) received a total of 33 courses of radiation therapy; 9 courses targeted the prostate, and 24 courses targeted other palliative sites. For 18 of the 19 radiation therapy patients (95%), radiation preceded the first infusion of 223Ra.
All 24 patients (100%) received a first infusion of 223Ra; 21 (88%), a second; 16 (67%), a third; 13 (54%), a fourth; 13 (54%), a fifth; and 11(46%), all 6 that were planned. Thus, 13 patients (54%) did not complete all 6 planned infusions of 223Ra, stopping because of clinical deterioration. The median OS in the 24 patients, from the first 223Ra infusion to the last follow-up (August 2020), was 8.3 mo (range, 0–44 mo; P = 0.01 vs. the ALSYMPCA median survival) (Tables 1–3). One of the 24 patients currently remains alive with disease, having completed 6 cycles of 223Ra.
DISCUSSION
The science supporting the development and clinical use of 223Ra is compelling. An α-emitter, 223Ra dichloride (223Ra) is bone-seeking and complexes with hydroxyapatite, releasing short-range (<100 μm), high-energy particles that exert a selective antitumor effect (20). Areas of active bone remodeling and bone vascular supply are the main target sites for 223Ra localization (21). In mouse models, 223Ra inhibits tumor-induced pathologic bone formation in the tumor microenvironment adjacent to tumor foci (22).
Preclinical work with mice confirmed that 223Ra selectively accumulates in the bone, with only minute amounts of daughter radionuclides released from skeletal sites of 223Ra decay (23). Moreover, dosimetry studies showed that short-range α-radiation from 223Ra substantially spares bone marrow, with relatively less toxicity than is caused by β-emitting 89Sr (23).
A phase 1 clinical trial demonstrated that 223Ra preferentially targets bone metastases rather than diffusely targeting healthy bone tissue (24). A randomized, multicenter, placebo-controlled phase 2 trial assigned patients receiving external-beam radiation therapy for pain control to receive either 4 223Ra injections (50 kBq kg−1) at 4-wk intervals or placebo on the same schedule. The group receiving 223Ra demonstrated a significant decline in alkaline phosphatase levels, a delay in the time to prostate-specific antigen progression, and a trend toward reduced skeleton-related events and improved OS. The safety profile was acceptable, hematologic toxicity did not significantly differ between the 2 groups, and no patient discontinued 223Ra because of treatment-related toxicity (25).
Parker et al. reported the pivotal phase III study of 223Ra, involving 614 223Ra-treated patients versus 307 in a placebo group, treated at 136 centers in 19 countries (3). At the time of publication, 532 of 921 patients (58%) had received all 6 injections of 223Ra. The median OS was 14.9 mo in the 223Ra group and 11.3 mo in the placebo group. 223Ra was associated with a 30% reduction in the risk of death versus placebo. The effect of 223Ra on OS was consistent across all subgroups, and 223Ra was not associated with significantly more grade 3 or 4 toxic effects than placebo.
However, subsequent to 223Ra approval and widespread use in the United States, multiple reports raised caveats concerning patient selection for 223Ra, finding shorter OS and more adverse events than reported by ALSYMPCA. Most of these have been smaller cohorts in single institutions, and there have also been a few multicenter experiences. Stolten et al. and Vogelzang et al. both looked at outcomes of patients receiving the full 6 cycles versus those who could not complete treatment. The cohorts had 55–184 patients, and OS favored those who completed all 6 cycles of therapy (16 mo vs. 4 mo in the Stolten et al. cohort, and 17 mo in the Vogelzang cohort) (4,5).
Etchebehere et al. reported 41 patients with metastatic prostate cancer treated at M.D. Anderson Cancer Center who had undergone fluoride PET/CT before 223Ra (26). They defined bone marrow failure as World Health Organization grade 3 hematologic toxicity with no recovery after 6 wk, or recorded death due to bone marrow failure. Bone marrow failure correlated with tumor burden on imaging, which, by multivariable analysis, was the only independent predictor for bone marrow failure. Another report by Etchebehere et al. on 110 223Ra-treated patients noted that improved alkaline phosphatase levels and pain scores were associated with improved outcomes (6).
Additionally, there have also been multiple reports showing better outcomes when using 223Ra earlier in the course of disease. Hague et al., Saad et al., Baldari et al., Wong et al., and Sartor et al. all found this to be the case within their respective studies (8,12,27–29). Specifically, Saad et al. had the largest cohort of these and reported on the early-access program after the ALSYMPCA study and before regulatory approval of 223Ra in 2013. In total, 839 patients were enrolled from 113 sites in 14 countries; 696 patients received one or more doses of 223Ra; 403 (58%) had all 6 planned injections (28). Sartor et al. reported the U.S. experience from the expanded-access phase II open-label, single-arm multicenter trial. Those with more advanced disease were less likely to benefit from the isotope. The median OS in those receiving 5–6 injections was not reached, whereas the median survival in those with fewer than 5 injections was 7.5 mo (12).
Of interest, one study has looked at possible predictive measures of survival in patients receiving 223Ra. Dittman et al. used quantitative bone SPECT/CT before 223Ra in 60 patients with mCRPC and found that isotope uptake in the central skeleton varied from 11% to 56% of the injected dose. After 223Ra, median OS in all 60 patients was 15.2 mo. When skeletal uptake was 26% or more, median OS was 7.3 mo; when skeletal uptake was less than 26%, median OS was 30.8 mo (17). The authors concluded that initial quantitative SPECT/CT bone scanning could predict subsequent patient survival after treatment with 223Ra. This finding may be of future interest once more data become available.
After reviewing our own patient experience, we identified certain factors likely contributing to our patients’ shorter-than-expected median OS. Practically all androgen deprivation, radiation, and cytotoxic therapy was given before referral to WVU for 223Ra. Although most referred patients initially seemed eligible for 223Ra on the basis of Eastern Cooperative Oncology Group performance status and the usual laboratory parameters, many appeared to receive only minor benefit from 223Ra as administered. When compared with the original ALSYMPCA prostate cancer patients, more patients at WVU received bisphosphonates and docetaxel, had a performance status of more than 2, took more opiates for cancer pain, had a greater bone metastasis burden, and had lower hemoglobin, albumin, alkaline phosphatase, and prostate-specific antigen levels (Tables 1–3).
Potential limitations of our study are that it was observational and retrospective, and our Appalachian referral-patient results may be hard to extrapolate to other practice settings. The ALSYMPCA trial was multicenter, multinational, and prospective, whereas our WVU data were from a single referral center. The number of 223Ra-treated patients studied in the 2 trials differed by over 25-fold, as we had a relatively small number of patients in our dataset (the last patient reported here started 223Ra in October 2018). Also, the data-collection time frames of the 2 studies differed by more than 5 y. Imaging in our patients included 12 nuclear bone scans (5 of which also included SPECT/CT), 8 body CT scans, and 4 PET/CT scans. Thus, only 7 patients had a nuclear bone scan, and use of higher-resolution imaging in the other 17 might have increased our detection of the number of bone lesions versus earlier studies using only conventional nuclear bone scans (17). Despite these issues, our report adds to the growing amount of real-world data concerning use of 223Ra, which will hopefully guide the future clinical application of this promising isotope.
CONCLUSION
We think that our initial referral pattern resulted in more heavily pretreated cancer patients receiving 223Ra, with suboptimal results versus ALSYMPCA. Hopefully, the referral pattern will improve as patients become more aware of 223Ra availability and use, with earlier patient demand and earlier referral for 223Ra. Currently, 223Ra appears to be an evolving and promising treatment for bone-predominant metastatic prostate cancer and potentially for other osteoblastic tumors, including metastatic breast cancer, differentiated thyroid cancer, and renal cell carcinoma (32). However, treatment benefit will likely be optimal when 223Ra is given earlier, targeted to patients who have not already exhausted most conventional therapies. Going forward, we continue to offer 223Ra isotope therapy for patients with symptomatic bone-predominant mCRPC but are emphasizing earlier referral to our center.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Nov. 20, 2020.
REFERENCES
- Received for publication July 28, 2020.
- Accepted for publication October 19, 2020.





{kind=link}