


Abstract
Pyelonephritis is an infection of the kidneys that is seen more commonly in children than the adults. 99mTc-dimercaptosuccinic acid (99mTc-DMSA) scanning is a radionuclide imaging study to detect renal scarring after acute pyelonephritis (a late 99mTc-DMSA scan) and also helps to diagnose acute pyelonephritis in febrile urinary tract infections (an acute 99mTc-DMSA scan). Planar imaging in multiple views (posterior and bilateral posterior oblique) is generally used. Pinhole imaging with a high-resolution-collimator magnification of each kidney allows detection of smaller cortical defects. SPECT is optional. SPECT/CT is not recommended in children because it has a higher radiation exposure than routine 99mTc-DMSA scans. The main limitations of 99mTc-DMSA scanning include a relatively long waiting time after radiotracer injection, a long acquisition time, and a high radiation dose, which is particularly important in repeated studies on children and with the limited spatial resolution of γ-cameras. 99mTc-glucoheptonate is an alternative radiotracer when 99mTc-DMSA is not available. Radiotracers for dynamic renal functional imaging can grossly assess the renal cortex in the first few minutes of imaging. 68Ga-prostate-specific membrane antigen ligand (68Ga-PSMA ligand) PET has the ability to provide images of normal renal cortex and demonstrate renal cortical defects from cysts. In this article, we assess the current status of renal cortical imaging and present 68Ga-PSMA ligand PET images. 68Ga-PSMA ligand provides excellent renal cortical images, and studies should be done to compare 68Ga-PSMA ligand PET with 99mTc-DMSA scanning in renal diseases, particularly in pyelonephritis.
Pyelonephritis is a bacterial infection of the kidneys. The estimated annual incidence of pyelonephritis is 10.5 million to 25.9 million cases globally (1–3). It is more commonly seen in children, particularly in infants and girls. Young sexually active women, the elderly, and pregnant women are also at risk.
Pyelonephritis can be acute or chronic. In acute pyelonephritis, kidney infection is sudden, whereas in chronic pyelonephritis, kidney infection is recurrent or persistent. The main cause of acute pyelonephritis is gram-negative bacteria, the most common being Escherichia coli. Vesicoureteral reflux is the most common underlying etiology in febrile urinary tract infections or pyelonephritis in children (4). Signs and symptoms of acute pyelonephritis usually include fever, flank pain, burning on urination, increased urinary frequency, and increased urinary urgency. Patients also experience nausea and vomiting. Common symptoms of acute pyelonephritis can be absent in children (5). Early diagnosis of pyelonephritis allows early treatment with antibiotics and reduces the risk of renal and nonrenal complications. Pyelonephritis can have complications such as sepsis, septic shock, hypertension, renal scarring or failure, and death.
A detailed history and physical examination are the mainstay of evaluating patients with pyelonephritis. Laboratory studies such as urinalysis, urine culture, and blood work (complete blood cell count and complete metabolic panel) should be performed. Imaging studies such as renal ultrasound, 99mTc-dimercaptosuccinic acid (99mTc-DMSA) scanning, abdominal or pelvic CT with contrast medium, and MRI are helpful in detecting acute pyelonephritis and renal scarring. The mainstay of treatment of acute pyelonephritis includes antibiotics, analgesics, and antipyretics.
99MTC-DMSA SCANNING
99mTc-DMSA is a widely used radiotracer for renal cortical imaging. 99mTc-DMSA binds to proximal tubular cells (pars recta), with 40%–65% of the injected dose being present in the renal cortex 2 h after the injection (6,7). 99mTc-DMSA scanning is used to detect renal parenchymal defects due to acute pyelonephritis and renal sequelae (scars) 6 mo after acute infection. It also helps detect renal abnormalities such as a duplex kidney, small kidney, dysplastic or horseshoe kidney, and ectopic kidney, as well as confirming a nonfunctional multicystic kidney (6,7).
The most common clinical indication for 99mTc-DMSA scanning is pyelonephritis (8–14). 99mTc-DMSA scanning is mainly used to detect scarring after acute pyelonephritis (a late 99mTc-DMSA scan). A wait of at least 6 mo is recommended before a 99mTc-DMSA scan is performed to check for scarring (7). 99mTc-DMSA scanning is also used to diagnose acute pyelonephritis in patients with febrile urinary tract infections (an acute 99mTc-DMSA scan) (7,10,12,14). Single or multiple defects are seen in the renal cortex in pyelonephritis. In acute pyelonephritis, renal cortical defects are seen as reduced or absence of uptake and do not deform the renal contour. There may be an increase in the volume of the affected area or the whole kidney (6). Renal cortical defects cause a volume loss in the affected cortex in cases of scarring after acute pyelonephritis and of chronic pyelonephritis (6). Acute and chronic pyelonephritis cannot always be distinguished on 99mTc-DMSA scans (6).
In routine 99mTc-DMSA studies, planar images of the kidneys with high- or ultrahigh-resolution collimators are obtained in posterior and bilateral posterior oblique projections (6,7). Additional planar images from anterior, both lateral and bilateral anterior, oblique projections can also be obtained if there is no patient motion or discomfort. Pinhole imaging with high-resolution-collimator magnification of each kidney allows detection of smaller cortical defects (6). SPECT imaging is optional, and various results have been reported comparing the sensitivity of SPECT with that of planar and pinhole imaging. SPECT was reported to be superior to planar imaging for demonstrating renal cortical defects (15,16). However, Brenner et al. reported that 99mTc-DMSA SPECT using a dual-head SPECT camera offers no statistically significant advantage over planar imaging for detection of cortical defects (17). Rodriguez et al. stated that contour defects are seen more frequently on tomographic slices, whereas reduced-uptake defects are seen more frequently on planar images (18). Interpretation of tomographic slices may be difficult because of the slightly vertical tilted anatomic position of the kidneys; 3-dimensional maximum-intensity projections may better demonstrate contour defects. SPECT/CT is not recommended in children because it has a higher radiation dose than routine 99mTc-DMSA scans.
Studies have shown that a 99mTc-DMSA scan is more sensitive than renal ultrasound for detecting acute and chronic pyelonephritis (19–21). Intravenous pyelography has a low sensitivity for detecting acute pyelonephritis (22,23). 99mTc-DMSA scanning has been shown to detect more defects than ultrasound or intravenous pyelography (24,25). Of children with acute pyelonephritis, changes were seen in 92% on 99mTc-DMSA scans, as opposed to 69% on renal ultrasound examinations (24). At follow-up, 68% of the children showed changes on 99mTc-DMSA scanning, 47% on renal ultrasound, and 48% on intravenous pyelography (24). 99mTc-DMSA scanning had abnormal results for 78% of the children with acute pyelonephritis, and renal ultrasound had abnormal results for 11% (25). Parenchymal defects seen on 99mTc-DMSA scans are not specific to pyelonephritis and can also be seen for renal abscess, cysts, a duplex kidney, and hydronephrosis. Hence, a combination of ultrasound and 99mTc-DMSA scanning allows better differentiation among these clinical situations (7). Doppler sonography (color and power) and 99mTc-DMSA results were concordant in 81% of kidneys with acute pyelonephritis (26). In another study, power Doppler was superior to color Doppler in defining the extent of hypoperfusion, which is seen in most pyelonephritic lesions (27). Studies have demonstrated that CT is more accurate or has a similar sensitivity and specificity to 99mTc-DMSA scanning for the detection of acute pyelonephritis, but CT has the risks of intravenous contrast reaction and higher radiation exposure (28–30). Studies comparing MR urography/MRI with 99mTc-DMSA scanning have shown that the former is equivalent or superior to the latter in the detection of pyelonephritis and renal scarring (31–33).
Per the American College of Radiology appropriateness criteria for acute pyelonephritis, scanning with 99mTc-DMSA, color Doppler ultrasound, CT with or without contrast medium, MRI, and other radiologic studies is usually not appropriate for initial evaluation of acute pyelonephritis in uncomplicated cases (19). In complicated cases of acute pyelonephritis (diabetic or immunocompromised patients, patients with a history of stones, patients with prior renal surgery, or patients not responding to therapy), abdominal and pelvic CT with and without intravenous contrast medium is usually appropriate and 99mTc-DMSA scanning, ultrasound, and MRI may be appropriate (19).
LIMITATIONS OF 99MTC-DMSA SCANNING
One of the main limitations of 99mTc-DMSA scanning is the relatively high radiation dose, particularly when multiple studies are needed in pediatric patients with recurring urinary tract infections. The effective dose estimate ranges from 1 to 10 mSv for adults and 0.3 to 3 mSv for children (19). The radiation dose to the kidney is 0.45 mGy/MBq, and the effective dose is 0.039 mSv/MBq for children (5 y old) (6).
The other limitations of 99mTc-DMSA scanning include the relatively long, usually 2-h, waiting time after radiotracer injection and the relatively long (minimally 15–30 min) image acquisition time (5–10 min per view, with a minimum of 3 views). A long acquisition time can cause motion artifacts. Patient sedation may be needed, particularly in infants or uncooperative children, to prevent motion artifacts. The sedation procedure is inconvenient for patients and families and laborious for physicians and staff, requiring preparing the patient, performing a presedation evaluation, obtaining informed consent, performing the sedation, and assessing the patient after sedation. It also carries certain risks and side effects. Immature renal function in newborns may cause a reduced kidney-to-background ratio and reduce the detection of cortical defects (6). A smaller percentage of lesions is detected in children under 1 y old than in children older than that (34). Physicians should also be aware of normal variations in kidneys (7). A high normal level of background activity in the renal cortex may obscure small parenchymal defects.
OTHER RADIOTRACERS FOR RENAL CORTICAL IMAGING
99mTc-glucoheptonate is another radiotracer used to image the renal cortex when 99mTc-DMSA is not available. 99mTc-glucoheptonate is partially concentrated and excreted in the urine. It is partially bound to the renal tubules, with 10%–20% of the injected dose being present in the proximal convoluted tubules of the cortex 2 h after injection (6). Approximately 40%–65% of this radiopharmaceutical is handled by glomerular filtration (6).
Dynamic renal imaging tracers such as 99mTc-mercaptoacetyltriglycine and 99mTc-diethylenetriaminepentaacetate can grossly assess the renal cortex in the first few minutes of the dynamic study and can demonstrate moderate or large cortical defects. Dynamic 99mTc-mercaptoacetyltriglycine scintigraphy can, at 2 min, show a region of decreased activity that, at 10–20 min, develops into an area of focal parenchymal retention (regional parenchymal dysfunction) (35). Sfakianakis et al. also used 99mTc-mercaptoacetyltriglycine SPECT to image the renal parenchyma (36).
POTENTIAL RADIOTRACERS
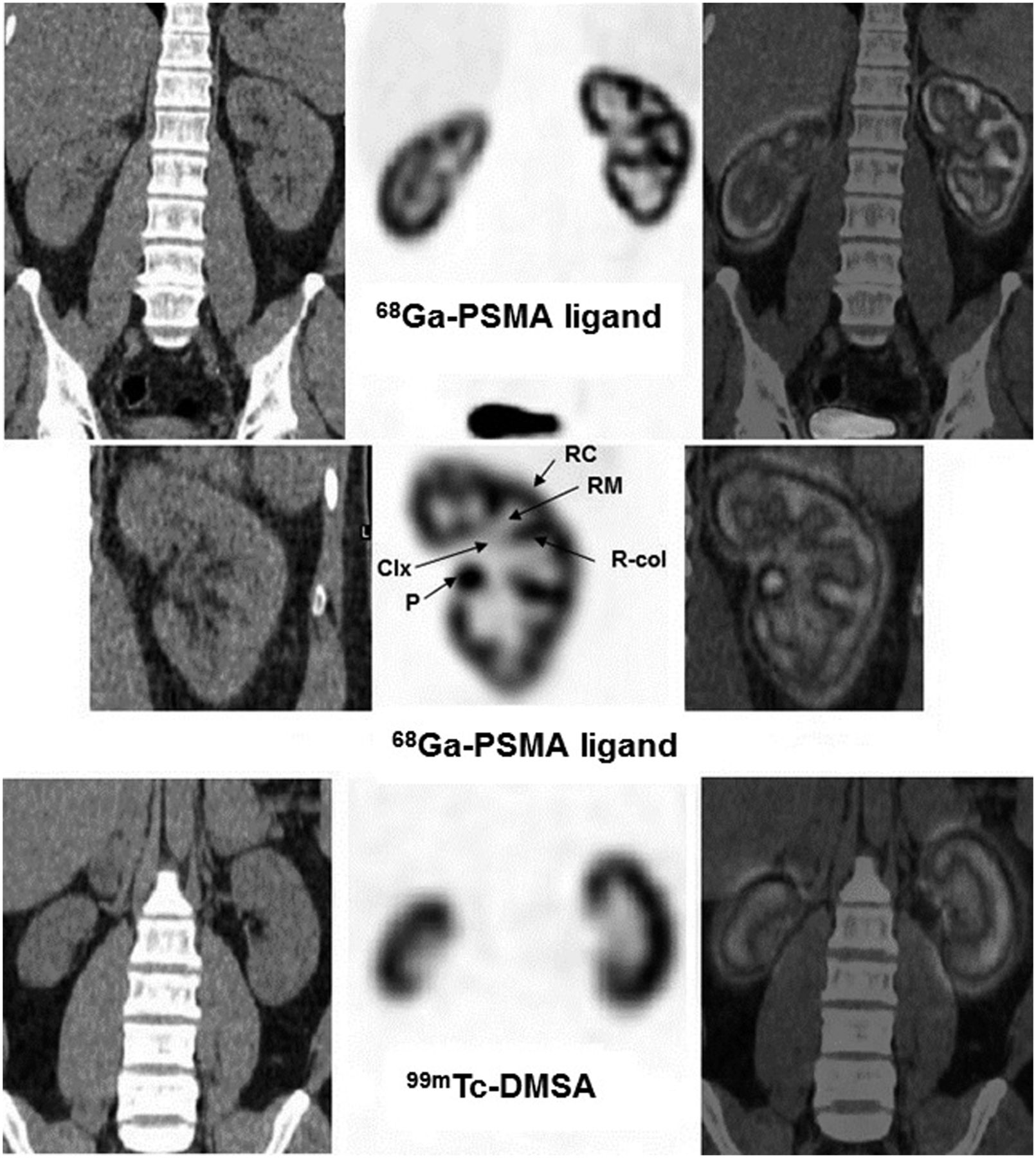
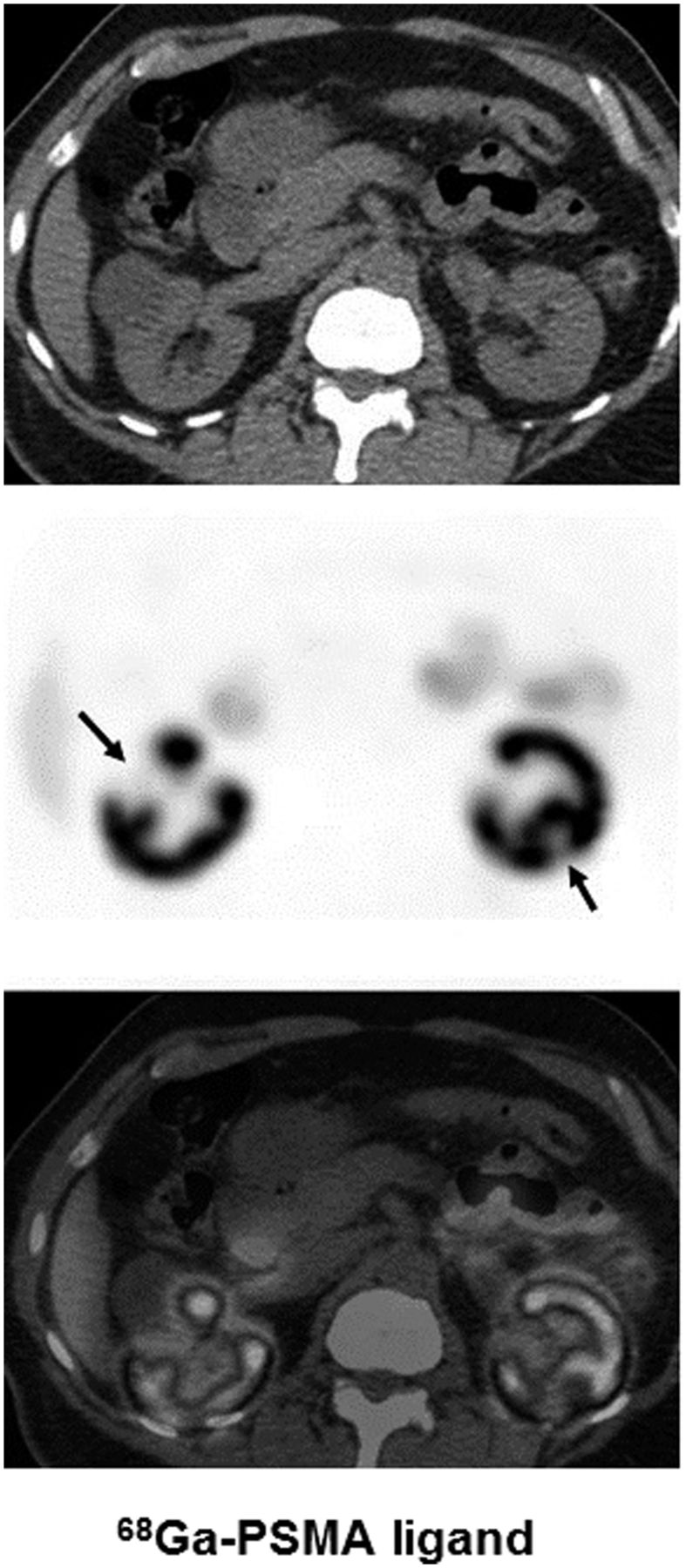
68Ga-prostate-specific membrane antigen ligands (68Ga-PSMA ligands) are relatively new PET radiotracers for prostate cancer that are used for initial staging in high-risk disease and for localization of prostate cancer in the setting of biochemical recurrence (37–40). The physiologic biodistribution of 68Ga-PSMA ligand includes uptake in various normal tissues, being highest in the kidneys. Assessing the kidneys in low-intensity settings shows that this radiotracer demonstrates high uptake in the renal cortex with high-resolution images (41). Figure 1 shows normal 68Ga-PSMA ligand PET images of the renal cortex as compared with 99mTc-DMSA scans. In Figure 2, renal cortical defects due to cysts are seen on 68Ga-PSMA ligand PET/CT images. 68Ga has a shorter half-life (68 min) than 99mTc (6 h). Effective and kidney radiation doses with 68Ga-PSMA ligand appear to be comparable to those with 99mTc-DMSA, but this comparison should be studied further (6,40,42). The CT part of PET/CT imaging further increases the radiation dose, but CT images may not be needed because non–attenuation-corrected PET also provides good-quality images of the kidneys due to high renal cortical uptake (41). The waiting time after radiotracer injection (30–60 min vs. 2–3 h) and the image acquisition time (2–6 min vs. 15–30 min) is less with 68Ga-PSMA ligand PET than with 99mTc-DMSA scanning. PET scanners offer higher efficiency for detecting γ-photons and higher spatial resolution than γ-cameras (43). Although 68Ga-PSMA ligand is costlier than 99mTc-DMSA and not available at every institute, it would be worthwhile to compare 68Ga-PSMA ligand PET with 99mTc-DMSA scanning in various renal diseases, particularly in pyelonephritis, to understand whether this PET radiotracer may be used to image the renal cortex.
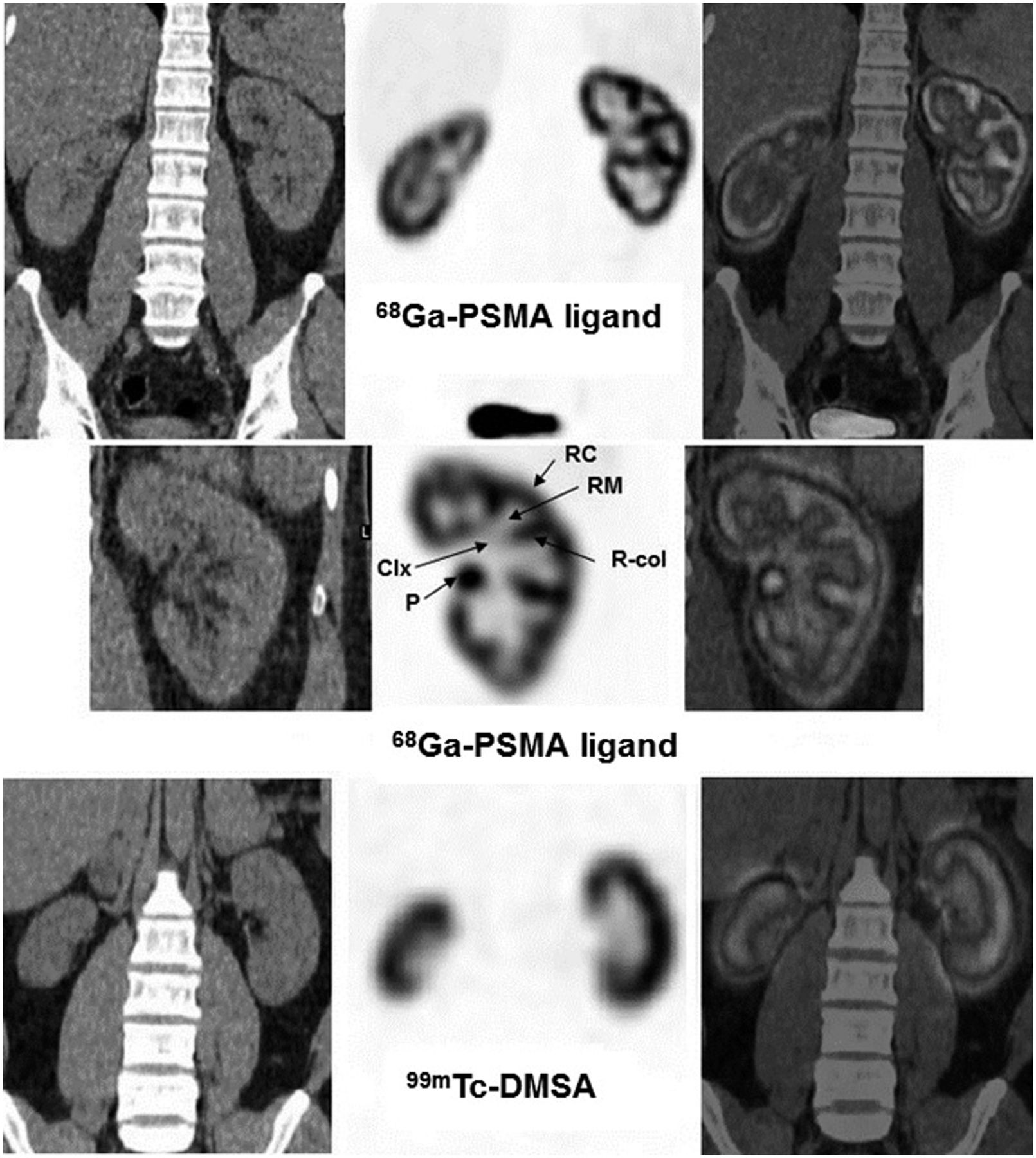
Coronal CT (left), PET (middle), and PET/CT (right) images of 68Ga-PSMA ligand (first 2 rows) and coronal CT (left), SPECT (middle), and SPECT/CT (right) images of 99mTc-DMSA (bottom row) in 2 different patients with normal renal profile. 99mTc-DMSA images are from 32-y-old average-sized man with microscopic hematuria and CT showing small right kidney and no parenchymal abnormalities in either kidney. Scan was performed 3 h after intravenous injection of 185 MBq (5 mCi) of 99mTc-DMSA using Discovery 670 16-slice SPECT/CT camera (GE Healthcare) equipped with high-resolution parallel-hole collimator (imaging parameters: low-dose CT; SPECT using 20 s per view, 60 views in 360° rotation, 128 × 128 matrix, no zoom, 20% window centered at 140 keV, and iterative reconstruction with 2 iterations and 10 subsets). 68Ga-PSMA ligand PET/CT images are from 59-y-old average-sized man with prostate cancer. Scan was performed 60 min after intravenous injection of 185 MBq (5 mCi) of 68Ga-PSMA ligand using Philips Gemini Time of Flight PET/CT camera (Philips Medical Systems) (imaging parameters: low-dose CT using 120 kVp and 40 mAs; PET using 3 min/bed position from skull base to mid thighs). 68Ga-PSMA ligand PET produced high-resolution images of kidneys with high uptake (SUVmax in left renal cortex, 50.7) and excellent separation of renal columns as compared with 99mTc-DMSA scanning. Clx = calyceal structures; P = pelvis (with mild pelvic activity); RC = renal cortex; R-col = renal column; RM = renal medulla.
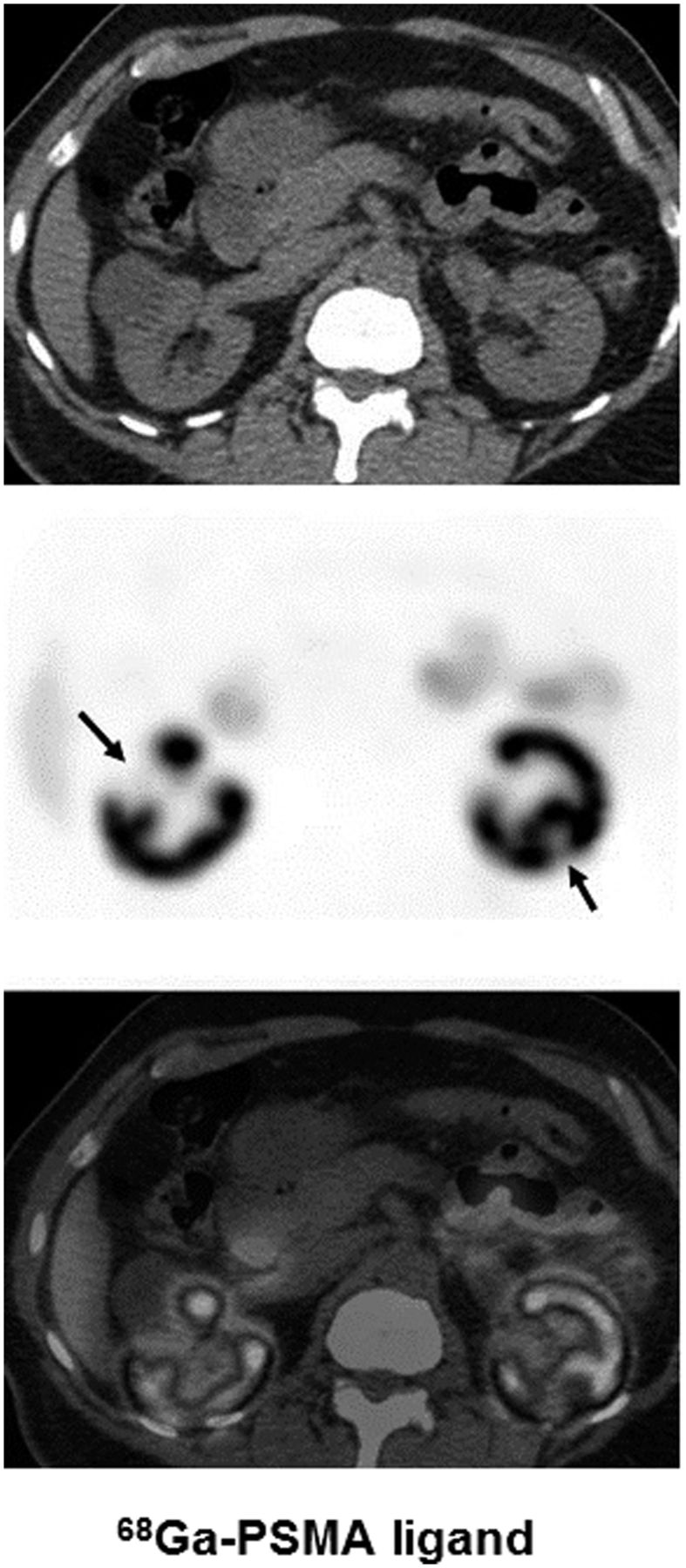
Transaxial CT (top), PET (middle), and PET/CT (bottom) images of 68Ga-PSMA ligand in 67-y-old man with prostate cancer and normal renal profile. Equipment and parameters are same as for Figure 1. PET image shows cortical defects in both kidneys corresponding to low-attenuation areas/cysts (arrows) measuring 32 × 34 mm on right and 8 × 10 mm on left. SUVmax was 74.7 in right renal cortex and 67.4 in right renal column.
CONCLUSION
Pyelonephritis is a common infection of the kidneys, particularly in children. Early diagnosis and treatment are important to avoid complications. Currently, 99mTc-DMSA scanning is a commonly used radionuclide renal cortical imaging study with certain limitations. 68Ga-PSMA PET shows excellent images of normal renal cortex and demonstrates renal cortical defects from cysts. In this article, we wanted to assess the current status of renal cortical imaging and present renal cortical PET images obtained with the 68Ga-PSMA ligand. 68Ga-PSMA ligand provides excellent renal cortical images, and further studies should be done to compare 68Ga-PSMA ligand PET with 99mTc-DMSA scanning in renal diseases, particularly pyelonephritis.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jun. 10, 2019.
REFERENCES
- Received for publication February 27, 2019.
- Accepted for publication April 23, 2019.





{kind=link}
{kind=link}