


Abstract
The objective of the study was to calculate neck uptake by γ-camera–based and uptake-probe–based methods and compare it with uptake by diagnostic whole-body and neck radioiodine scanning in thyroid carcinoma patients. Methods: Of the 46 patients, 14 were male (average age, 47.5 y) and 32 female (average age, 38 y). All had already undergone thyroidectomy followed by 131I treatment at least once and came to the institute after 6 mo for follow-up. As per the institutional protocol, they underwent scanning 72 h after administration of a low-dose capsule (111–148 MBq) of 131I, and the uptake was calculated by both probe- and camera-based methods using medium-energy parallel-hole collimators. Results: The neck was negative for uptake in 24 patients by both the probe-based method (with 0.1% as the cutoff) and the camera-based method, as well as by the scan. The neck was positive for uptake in 10 patients by both methods and by the scan. In 10 patients, the neck was positive for uptake by the probe-based method but negative by the camera-based method and the scan; in most of these cases, nontarget counts contributed to high scatter radiation. In 2 patients, the neck was negative for uptake by the probe-based method but positive by the camera-based method and the scan. Thus, the two methods were concordant in 34 of the 46 patients (74%) but discordant in 12 (26%). On the basis of these results, we propose that 0.03% be the cutoff for positivity for the camera-based method. In 85.7% of patients with negative scan results and systemic metastases near the neck (n = 7), an uptake cutoff of 0.1% resulted in positive results. All patients had true-negative results with a camera-based cutoff of 0.03%. In view of this discordance between the probe-based method and the scan, we further propose that 0.2%, rather than 0.1%, be the cutoff for positivity for the probe-based method in order to reduce false positivity. Conclusion: In thyroid carcinoma patients undergoing 131I low-dose scans, camera-based uptake is as reliable as, and can substitute for, probe-based uptake in evaluating functioning metastases near the neck or nonspecific high physiologic accumulation.
The use of 131I in patients with differentiated thyroid carcinoma is well established for both diagnosis and therapy. In postthyroidectomy patients with differentiated thyroid carcinoma, it is common practice to give a low diagnostic dose of 131I for qualitative and quantitative evaluation of residual thyroid tissue. Although 123I is a better agent for diagnostic scanning, 131I continues to be used in several developing nations where 123I is not available (1). Quantitative evaluation is usually done using a thyroid uptake probe, whereas γ-cameras give qualitative imaging information. A γ-camera–based method for evaluating 131I uptake in the neck has been reported for benign and other noncancerous clinical conditions (2). On the basis of the diagnostic scan, neck uptake value, pathology reports, and disease burden, patients are planned for radioiodine ablation or therapeutic doses of 131I. Six months after the first therapy, it is customary in our institute to have the patients return for a follow-up examination. In this study, we calculated the percentage of neck uptake by the probe-based and camera-based methods and compared it with the diagnostic radioiodine scan and with the level of serum stimulated thyroglobulin (in all cases) and clinical and ultrasound findings (when appropriate).
MATERIALS AND METHODS
Study Population
Forty-six patients undergoing 131I scanning between 2014 and 2015 were included in this Institutional Review Board–approved study. Fourteen were male (average age, 47.5 y) and 32 female (average age, 38 y). All were postthyroidectomy differentiated thyroid carcinoma patients who had undergone one 131I treatment in the past and had returned after 6 mo for a follow-up scan. Standard precautions for radioiodine scanning had been undertaken (regarding avoidance of iodine-containing substances and thyroid medications and exclusion of pregnant or lactating women). A 111- to 148-MBq 131I capsule was orally administered, and neck uptake was evaluated 72 h later by both the probe-based and the camera-based methods.
Probe-Based Method
An uptake probe (Nuclear Chicago) loaded with a flat-field collimator was used to estimate the neck count. A 0.925-MBq standard 131I capsule was kept in a clear acrylic neck phantom and counted for 100 s. A neck shield was added over the phantom, and the background count was measured. The counts were taken 30 cm from the crystal, where the probe gives isoresponse. This count was further extrapolated for the low-dose radioactivity administered to the patient after decay correction (3).
The patient was positioned 30 cm from the probe 72 h after receiving the capsule, and the count was taken for 100 s. The neck was shielded, and the background count was taken for 100 s. Percentage uptake was calculated using the following formula (2): % uptake = (neck count − patient background count)/(standard phantom count extrapolated for patient-administered radioactivity − phantom background count).
Camera-Based Method
In the same group of patients, the camera-based method was then adopted to calculate the 72-h neck uptake (Table 1). To obtain a standard count, the 131I capsule in the neck clear acrylic phantom was scanned with a speed of 4 cm/min and a matrix size of 1,024 × 512, and the counts were calculated by drawing a region of interest around the capsule and extrapolating for the patient’s administered radioactivity to get the net standard counts equivalent to the administered large dose of radioactivity.
κ-Test Statistics Obtained Between Performance of Camera-Based Method, Probe-Based Method, and Scan Finding (Reference) in Patients with Thyroid Carcinoma
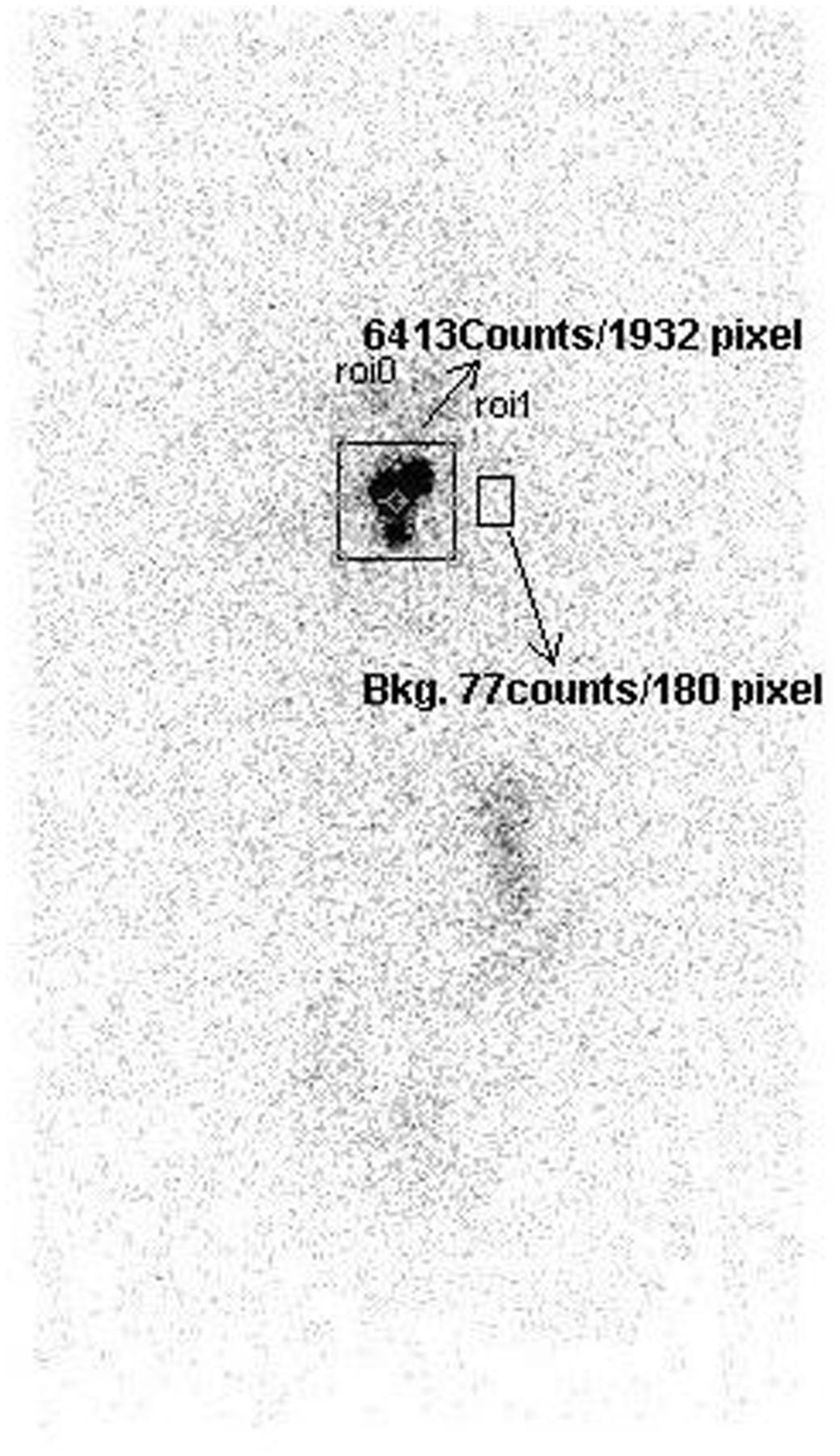
The neck scan was obtained by positioning the patient supine with neck extended. A γ-camera with a medium-energy collimator (Symbia; Siemens) was used for scanning and for the camera-based method. The scan was acquired with a speed of 4 cm/min and the energy window centered on 364 keV, with a 15% window and a matrix size of 1,024 × 512. A region of interest was then drawn on the neck to obtain the neck counts, and the total pixel area was noted. A background region of interest was drawn near the thyroid to obtain the average background count per pixel (Fig. 1). Percentage neck uptake was calculated using the following formula (3): % uptake = (background-corrected neck count/standard count) × 100.
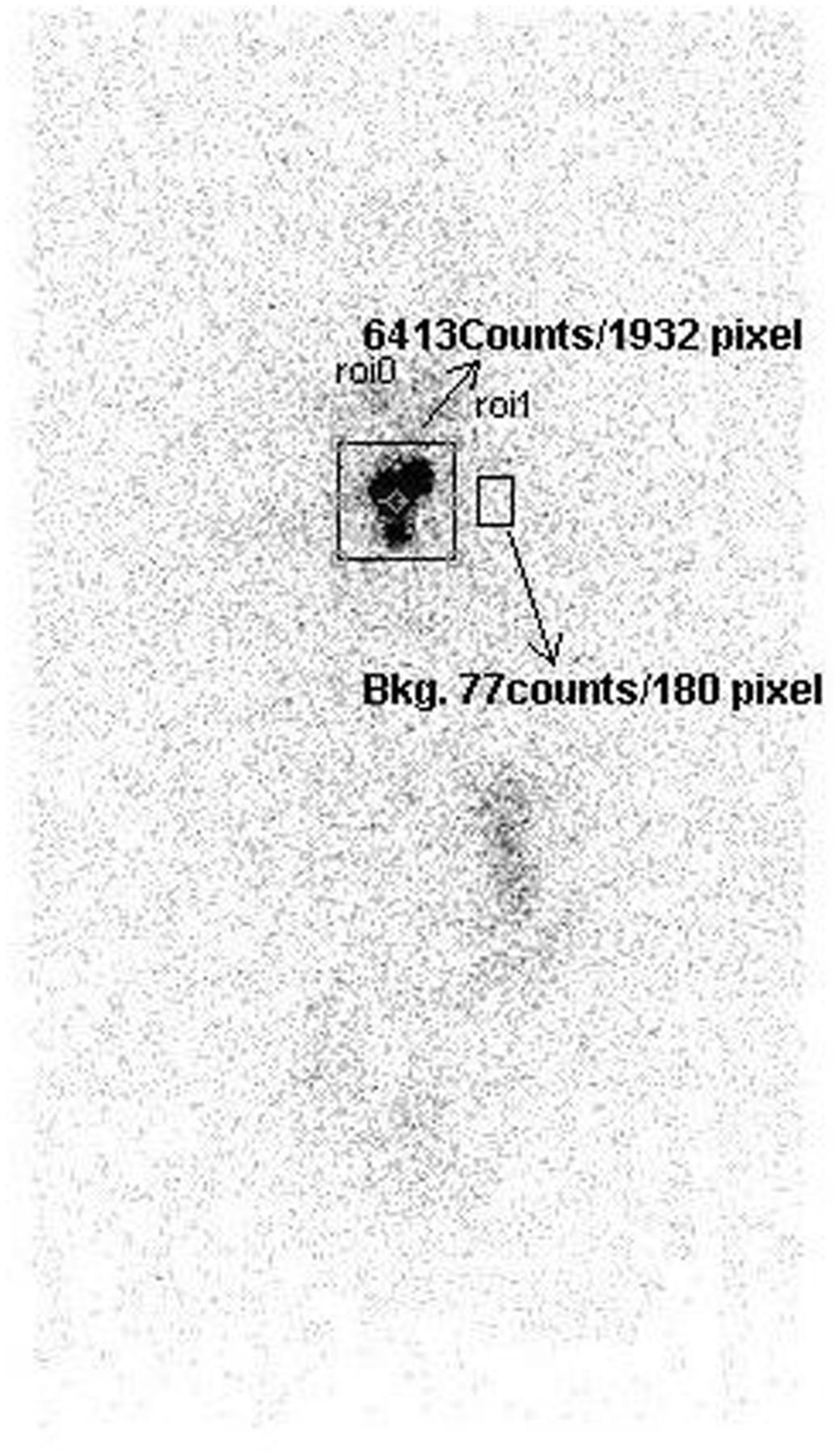
Neck and background count estimation by camera-based method. Bkg = background; roi = region of interest.
The serum thyroglobulin value was available for 39 patients to correlate with the clinical findings. As per our institutional protocol, a stimulated thyroglobulin value of 5 ng/mL or less was considered to be insignificant.
RESULTS
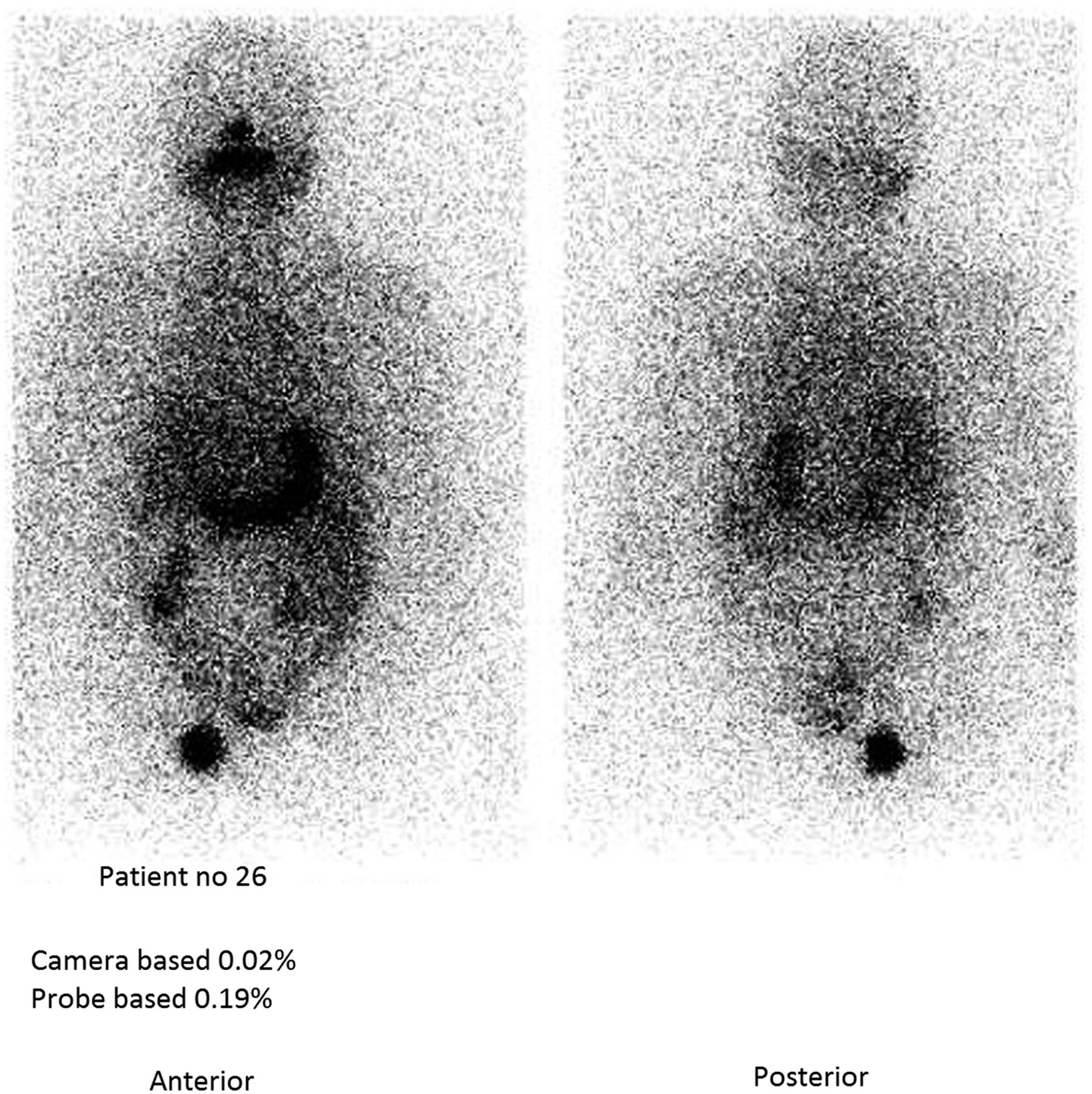
Probe-based neck uptake was compared with camera-based neck uptake, using the neck scan finding as the reference standard. In accord with our institutional protocol, any uptake less than 0.1% by the probe-based method was considered negative. A cutoff of 0.03% for camera-based uptake correlated well with the scan findings. The serum thyroglobulin value was available for 39 patients to correlate with clinical findings. On this basis, the neck was negative for uptake in 24 patients and positive for uptake in 10 patients by both probe-based and camera-based methods, and these findings were supported by the scan finding. Thus, the methods were concordant in 34 of 46 patients (74%) and discordant in 12 (26%). In 10 patients, the probe-based method was positive for uptake but the camera-based method and scan were negative (Figs. 2 and 3). In most of these cases, there was a high contribution of scatter radiation from the lungs, stomach, and salivary glands. The individual values are compared in Supplemental Tables 1 and 2 (supplemental materials are available at http://jnmt.snmjournals.org), and uptake by the camera-based and probe-based methods is graphed in Figure 4. The Pearson correlation coefficient between the camera-based and probe-based methods was measured to be 0.97, which indicates high concordance. The independent performance of these methods is presented as mosaic plots in Figure 5. Sensitivity, specificity, and agreement analysis was performed to compare pairwise diagnostic performance between the camera-based method, probe-based method, and scan. A cutoff of 0.03% for the camera-based method was arbitrarily selected on the basis of our observations. Similarly, 2 cutoff detection points—0.1 and 0.2—for the probe-based method were selected on the basis of routine practice evidence (Supplemental Table 3). Agreement between the methods in detecting true-positive and true-negative findings was tested with κ-statistics (Table 1), with a value of 0.69 obtained between the camera-based method and the scan and values of 0.52 (with a probe-based cutoff of 0.1%) and 0.64 (with a probe-based cutoff of 0.2%) obtained between the camera-based and probe-based methods. The corresponding sensitivity and specificity were 95% and 74.28% (with a probe cutoff of 0.1%) and 54.54% and 100% (with a probe cutoff of 0.2%). Also, interestingly, in patients with a negative scan result and systemic metastases near the neck (n = 7, Supplemental Table 2), an uptake cutoff of 0.1% resulted in positive results in 85.7% but an uptake cutoff of 0.2% resulted in no positive results. All patients had true-negative results with a camera-based cutoff of 0.03%.

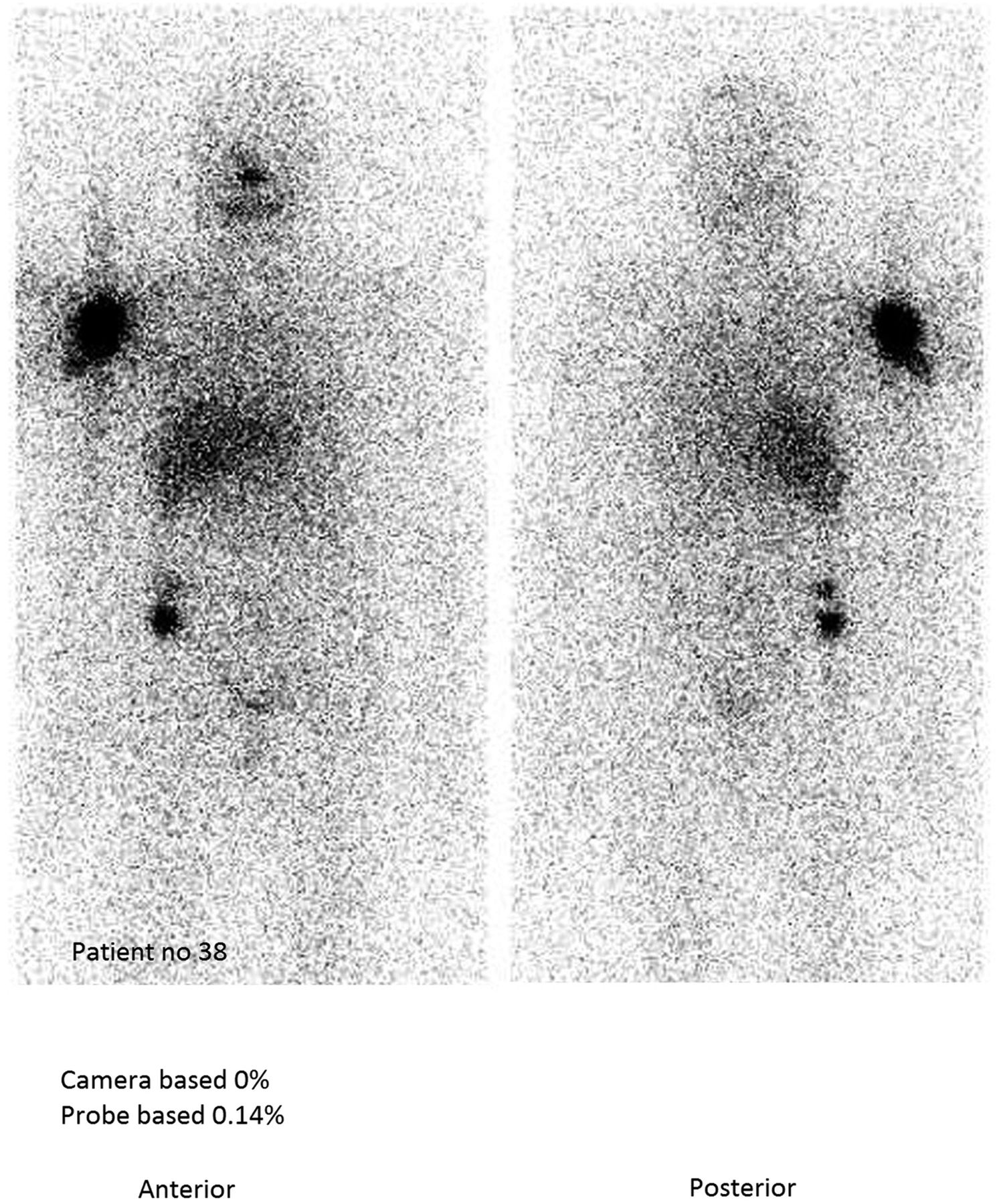
A 57-y-old woman who had differentiated thyroid carcinoma and skeletal metastasis (after one previous therapy). Increased stomach and salivary gland uptake is seen. Probe-based method is positive for neck uptake, but camera-based method and scan are negative.

A 67-y-old woman who had differentiated thyroid carcinoma and shoulder metastasis. Probe-based method is positive for neck uptake, whereas scan and camera-based methods are negative.
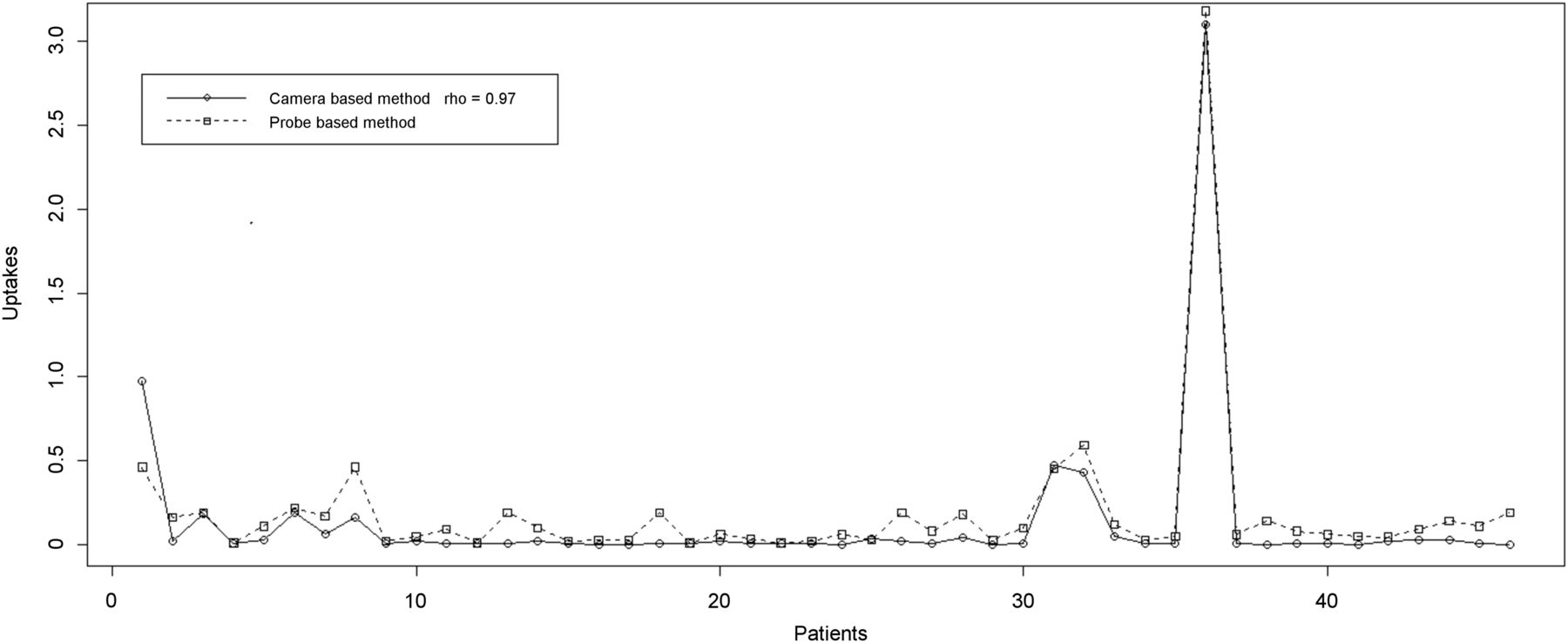
Measurements obtained through camera-based and probe-based methods are highly concordant, with Pearson correlation coefficient of 0.97.

Pairwise comparison between camera-based, probe-based, and scan findings to detect positive and negative cases.
DISCUSSION
Radioiodine scanning with 131I is well established and has been in routine use for evaluating thyroid uptake and scans (for both malignant and benign conditions) in several countries where 123I is not available. Qualitative evaluation is done by γ-camera scanning, and quantitative evaluation is done using an uptake probe. Since the 2 procedures are done separately, use of an alternate camera-based method for quantitative and qualitative evaluation in a single procedure has been reported for low-dose scans of, mainly, benign thyroid disorders (primarily thyrotoxicosis) (2). In the present study, the utility of the camera-based method in postthyroidectomy patients was evaluated and compared with the probe-based method, which is the methodologic standard for measuring thyroid uptake. Furthermore, we sought to evaluate cases of discordance and explore the clinical correlate and advantages for either of the methodologies.
According to our institutional protocol, neck uptake is correlated with scan findings and thyroglobulin level in all patients. Any neck uptake greater than 0.1%, which is considered positive by the probe-based method, is reevaluated by performing a high-count scan to confirm persistence or recurrence. It has been observed in all the population of the present study that camera-based uptake of less than 0.03% is neck scan–negative (as confirmed by a high-count scan and serum thyroglobulin level in patients who show no metastasis by scanning), and the corresponding values for the probe-based method are high. In the present study, a camera-based uptake cutoff of 0.03% was found to be a useful diagnostic parameter when compared with a probe-based uptake cutoff of more than 0.1% and comparable to a probe cutoff of 0.2%, especially when the patients had metastatic disease near the neck. When camera-based uptake was less than 0.03%, the opinion of expert nuclear medicine physicians was taken, and on the basis of the final scan findings and clinical evaluation all scans were found to be negative (all were negative when 0.2% was considered the cutoff by the probe-based method), suggesting the camera-based method to be an alternative to the probe-based method (Supplemental Table 3). Our proposed 0.2% cutoff is commensurate with the cutoff proposed by Bal et al. in 1996 (4).
Multiple factors could contribute to the higher uptake obtained by the probe-based method than the camera-based method: use of a parallel-hole versus a flat-field collimator, inclusion of nontarget counts such as salivary glands in the probe-based method, and the difference in thickness between the probe and camera scintillation crystals (2.54 cm [1 in] for the probe vs. 1.59 cm [5/8 in] for the camera). Other, less probable, factors could be measurement during scanning versus at a single location and the use of a medium-energy collimator for a high-energy radionuclide in the camera-based method. In all cases of discordance, the fact that nontarget counts were high contributed to the counting uncertainty in the probe-based method, which uses a flat-field collimator rather than the parallel-hole collimator of the camera-based method; in the latter, the neck region of interest can minimize nontarget counts.
CONCLUSION
Calculation of 131I neck uptake after administration of 0.925 MBq to patients with benign thyroid disorders (thyrotoxicosis and nonthyrotoxic multinodular goiter) correlates well between the camera-based and probe-based methods. In such patients, the camera-based method is a good substitute for the probe-based method. In this study, we evaluated and compared a different group of patients—those being followed up for differentiated thyroid carcinoma—using an activity of 111−148 MBq and an uptake period of 72 h. The comparability of neck uptake when a cutoff of 0.2% was used for the probe-based method and 0.03% for the camera-based method makes the latter a good substitute for the former, as, in a single procedure, both qualitative and quantitative information are achievable. To reduce false positivity, we also propose that a 0.2% cutoff be preferred over 0.1% for the probe-based method, on the basis of comparison with the camera-based method.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Nov. 9, 2018.
- Received for publication January 4, 2018.
- Accepted for publication October 9, 2018.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.