


Abstract
Our purpose was to determine whether there is a clinical benefit to add lower-limb imaging in 68Ga-labeled prostate-specific membrane antigen (PSMA) PET/CT scans for patients with prostate cancer. Methods: In total, 701 patients with prostate cancer who underwent 68Ga-PSMA PET/CT were evaluated retrospectively. All patients underwent additional lower-limb imaging. Images were reanalyzed by experienced nuclear medicine physicians, and metastatic sites were documented. The prostate-specific antigen (PSA) level and Gleason score were also compared with 68Ga-PSMA PET/CT findings. Results: In 601 patients (85.7%), at least 1 tumoral lesion was observed on 68Ga-PSMA PET/CT. The number of patients with bone metastasis in 2 forms was 278 patients (39.6%); 108 (15.4%) were oligometastatic (<4 metastases) and 170 (24.2%) were multimetastatic (≥4 metastases). In lower-limb imaging, bone metastasis was detected in 61 patients (8.7%), the specific locations of which were as follows: middle–distal femur (n = 54), tibia (n = 19), fibula (n = 24), and calcaneus (n = 1). Lower-limb metastasis was detected mostly in symptom-positive patients (70.1%) but in only 4% of the symptom-negative group. All patients with lower-extremity metastasis also had multiple bone metastases shown on limited whole-body 68Ga-PSMA PET/CT. The median PSA level was significantly higher in multimetastatic patients with lower-limb metastasis than in those without lower-limb metastasis (P < 0.001, Mann–Whitney U test), but no statistical differences was found in terms of Gleason score (χ2 = 0.042, P = 0.837). According to receiver-operating-characteristic analysis, PSA has a good predictive value for detecting lower-limb metastasis, with 76.6% sensitivity and 72% specificity (using a reference cutoff PSA level of 24 ng/mL [area under the curve, 0.81; 95% confidence interval, 0.74–0.87]). Conclusion: Lower-limb imaging did not change the metastatic status of disease or significantly affect the therapeutic approach. However, if multimetastatic patients present relevant symptoms for lower-limb metastasis, it could be beneficial to consider including lower-limb imaging for possible palliative therapies.
Prostate cancer (PC) is one of the most common cancers seen in men across the world. The incidence of PC has been increasing in recent years; it alone now accounts for almost 1 in 5 new cancer diagnoses (1). Although most patients have localized disease at initial diagnosis, distant metastasis can occur in 35% of cases during follow-up (2). Bone is the most common site of metastasis, accounting for more than 80% of all cases, and is associated with a high risk of morbidity (3). Detection of bone metastasis with conventional imaging modalities is limited, with bone scintigraphy being most commonly used for the assessment of skeletal metastasis in PC (4,5). Recently, the use of several PET radiotracers has been proposed for PC imaging, including a prostate-specific membrane antigen (PSMA) that is a transmembranous enzyme significantly overexpressed in most PC cases (6–9). We and others have previously shown the diagnostic power of 68Ga-PSMA PET/CT in the assessment of bone metastasis (6,7,10). However, the scanning area in 68Ga-PSMA PET/CT is generally limited to the area from the base of the skull to the upper thigh to decrease scanning time, in contrast to whole-body bone scintigraphy (11). Thus, metastasis of the lower limbs can be missed in 68Ga-PSMA PET/CT because this area is beyond its range. In our clinic, lower-limb imaging is performed on all patients with PC, in addition to the limited whole-body 68Ga-PSMA PET/CT imaging. Within this study, we intended to determine whether there is a clinical benefit to additional lower-limb imaging in 68Ga-PSMA PET/CT scans for patients with PC.
MATERIALS AND METHODS
Patients
In total, 735 patients who underwent a 68Ga-PSMA PET/CT scan at our clinic between January 2015 and December 2017 were reviewed, and 701 patients with histologically confirmed PC were included in this retrospective study (mean age, 62 y; range, 50–92 y). 68Ga-PSMA PET/CT scans were performed for staging (n = 249), restaging (n = 376), and therapy response (n = 76). Patients with bone pain in the distal extremities and numbness or weakness in the legs were categorized as symptom-positive. The median serum free prostate-specific antigen (PSA) level was 9.3 ng/mL (range, 0.003–4,227 ng/mL). The initial median Gleason score (GS) was 7 (range, 5–10). Details of the patients’ characteristics are given in Table 1. This retrospective study was approved by our institutional review board, and written informed consent was obtained from all patients.
Demographic and Clinical Characteristics of Patients
68Ga-PSMA Synthesis and PET/CT Acquisition
We applied 68Ga-PSMA labeling according to a protocol described in the literature (12). 68Ga-PSMA PET/CT was performed on a dedicated PET/CT scanner (Biograph TruePoint PET/CT; Siemens Healthcare) at 45–60 min after the intravenous injection of approximately 185 MBq of 68Ga-PSMA. An iodine-based oral contrast agent was administered to all patients. The whole body of all patients was scanned in 2 steps. A scan was acquired from the top of the head through the upper thigh, and a separate scan was acquired of the rest of the lower limbs. The CT acquisition was performed on a spiral CT scanner, with a slice thickness of 4 mm and a pitch of 1. After the CT scan, 3-dimensional PET images were acquired for 3 min per bed position for limited whole-body imaging and 2 min per bed position for lower-limb imaging. CT-based attenuation correction of the emission images was used. PET images were reconstructed by the iterative method using ordered-subset expectation maximization (2 iterations and 8 subsets). After completion of the PET acquisition, the reconstructed attenuation-corrected PET images, CT images, and fused PET/CT images were reviewed. The effective doses for additional lower-limb CT examinations were calculated by summing the tissue-weighted equivalent doses for all tissues irradiated based on ICRP-103 weighting factors (13)
Image Analysis
The images were visually evaluated by a minimum of 2 experienced nuclear medicine physicians. Areas of abnormally increased tracer uptake in relation to PC metastasis were documented. Bone metastasis was listed as lower-extremity metastasis when detected on additional lower-limb imaging. Patients with bone metastasis were also categorized as having either oligometastatic disease (<4 metastases) or multimetastatic disease (≥4 metastases) (based on data from a previously published study) (14). All suspected lesions were also evaluated with other imaging, including CT, MRI, multiparametric MRI, bone scintigraphy, 18F-NaF-PET/CT, and histopathologic results (if present). The effect of clinical management was evaluated by the diagnostic information from the limited whole-body and lower-limb 68Ga-PSMA PET/CT scans and surveillance of disease with a minimum 6 mo of follow-up.
Statistical Analysis
The Mann–Whitney U test was used to compare serum PSA levels, and the χ2 test was used to compare the following: GS (5–7 vs. 8–10) in both positive and negative 68Ga-PSMA PET/CT scans, multimetastatic versus oligometastatic patients, and multimetastatic patients with lower-limb metastasis versus patients without lower-limb metastasis according to 68Ga-PSMA PET/CT findings. Statistical significance was assumed for P values of less than 0.05. Receiver-operating-characteristic curves were plotted to evaluate the utility of serum PSA in detecting patients with lower-limb metastasis. The area under the curves, with corresponding 95% confidence intervals, were calculated. Optimal serum PSA cutoffs were then determined by taking the left upper point in the receiver-operating-characteristic curve and the corresponding sensitivity and specificity. Statistical analyses were performed using IBM SPSS statistics, version 24.
RESULTS
In 601 patients (85.7%), at least 1 positive tumoral lesion was detected on 68Ga-PSMA PET/CT. In the remaining 100 patients (14.3%), 68Ga-PSMA PET/CT images were negative. The prostate or prostatic bed was the most common site, with the presence of a tumor observed in 400 patients. Seminal vesicle invasion was detected in 58 patients (8.2%), and gross invasion to the bladder or rectum was observed in 29 patients (4.1%). At least one lymph node metastasis was detected in 300 patients (42.7%). This was localized in the pelvic region of 272 patients (38.8%), was in the abdomen of 128 patients (18.2%), and was supradiaphragmatic in 91 patients (12.9%). Thirty-six patients (5.1%) had lung metastasis, and 24 patients (3.4%) had liver metastasis. Least commonly, metastasis to either the brain, adrenal gland, or peritoneum was observed in 15 patients (2.1%). Lastly, bone metastasis was detected in 278 patients (39.6%). Suggestive 68Ga-PSMA PET/CT findings were correlated with other scans, including MRI (n = 56), multiparametric MRI (n = 14), and 18F-NaF PET/CT (n = 3). Histopathologic correlation was performed for final diagnosis (n = 4).
On the basis of the previously described criteria, of the 278 patients with bone metastasis, 108 (15.4%) had oligometastatic disease and 170 (24.2%) had multimetastatic disease. In lower-limb imaging, at least 1 bone metastasis was detected in 61 patients (8.7%). Middle–distal femur metastasis was observed in 54 patients. Tibia metastasis was detected in 19 patients, and fibula metastasis was detected in 24 patients (Fig. 1). One patient with multimetastatic disease also had calcaneus metastasis. All patients with lower-extremity metastasis had multiple bone metastases shown on the limited whole-body 68Ga-PSMA PET/CT scan. None of these patients had oligometastatic disease, nor did they have isolated lower-extremity metastasis.

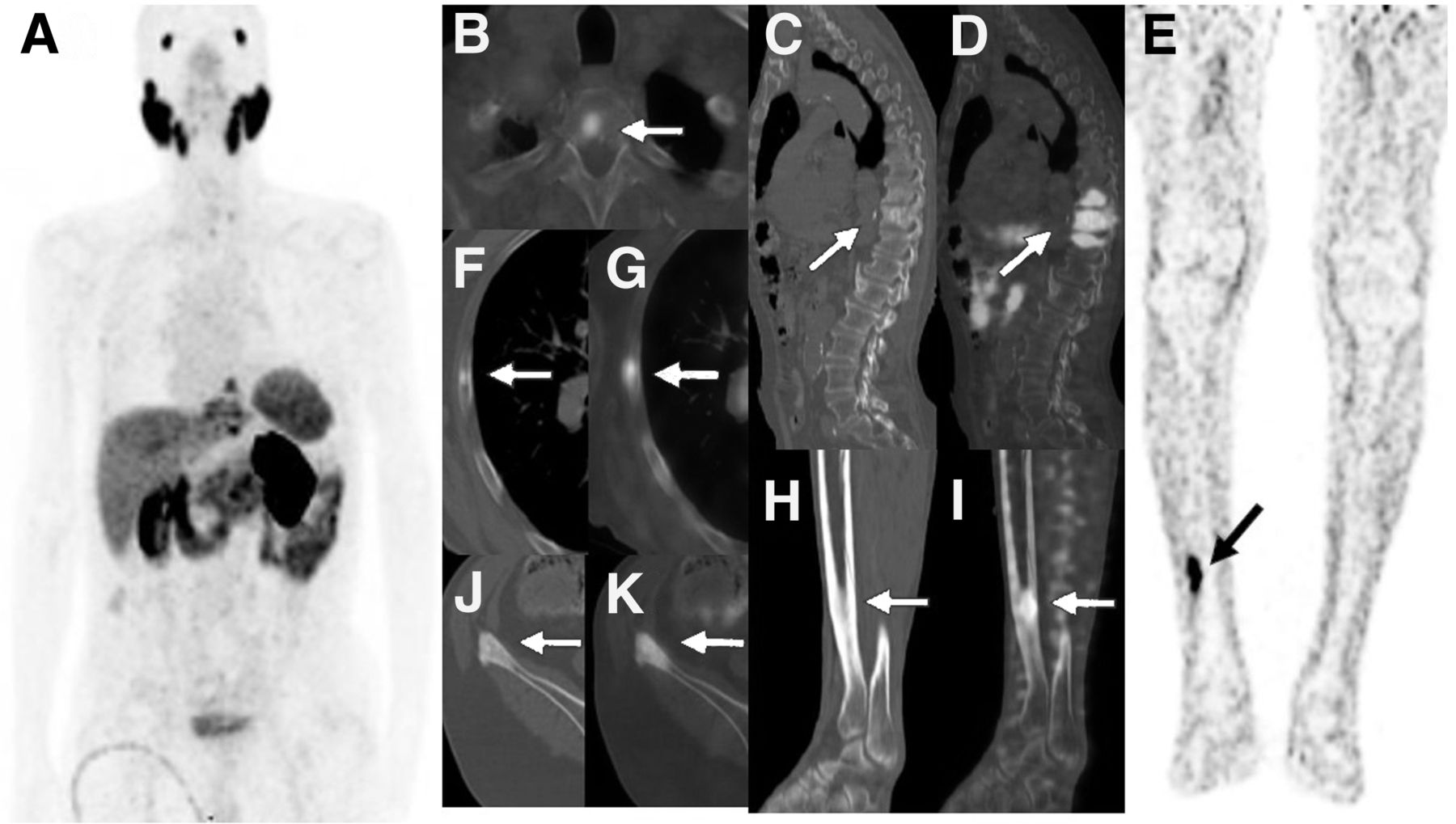
Example of multimetastatic patient with tibial metastasis of PC. A 75-y-old man who received androgen deprivation therapy was scanned with 68Ga-PSMA PET/CT for restaging because of elevated serum PSA level (GS, 4 + 3 = 7; PSA, 25.17 ng/mL). Pathologic 68Ga-PSMA uptake in sclerotic metastases was seen to have localized in right fifth rib (arrows on axial CT [F] and axial fusion [G]), T1 vertebra (arrow on fusion [B]), T9–T11 vertebrae (arrows on sagittal CT [C] and sagittal fusion [D]), and right iliac crest (arrows on axial CT [J] and axial fusion [K]) on limited whole-body 68Ga-PSMA PET/CT images (maximum-intensity projection [A]). Additionally, sclerotic metastasis in right distal tibia with intense 68Ga-PSMA uptake (arrows on sagittal CT [H], sagittal fusion [I], and coronal PET [E]) was seen on lower-limb 68Ga-PSMA PET/CT images. Stage of disease did not change with tibial metastasis. However, patient had leg pain for almost 4 wk and received external radiotherapy for palliation.
Lower-limb metastasis was detected more frequently in a therapy response group, at 26.3% (in 20/76 patients), which comprised patients with known bone metastasis from previous imaging. In the restaging group, the ratio was slightly higher than in the staging group, at 8.5% (32/376) versus 3.6% (9/249), respectively. When we evaluated patients according to the presence of symptoms, 39 of 55 symptom-positive patients (70.1%) had lower-limb metastasis and 22 of 546 symptom-negative patients (4%) had lower-limb metastasis. Meanwhile, demonstrating the lower-limb metastasis did not change the metastatic status or significantly affect the therapeutic approach. Patients with symptoms or riskier metastasis of weight-bearing bone were treated with analgesics, bisphosphonates, and external radiotherapy.
We compared the median PSA value and GS for positive versus negative 68Ga-PSMA PET/CT scans, multimetastatic versus oligometastatic patients, and multimetastatic patients with lower-limb metastasis versus those without lower-limb metastasis. The median PSA value was significantly higher in positive than in negative 68Ga-PSMA PET/CT scans (P < 0.001), multimetastatic than in oligometastatic patients (P < 0.001), and multimetastatic patients with lower-limb metastasis than in those without lower-limb metastasis (P < 0.001), according to the Mann–Whitney U test. A higher GS (8–10) was correlated with positive 68Ga-PSMA PET/CT scans and multimetastatic disease, in comparison to negative 68Ga-PSMA PET/CT scans (χ2 = 26.642, P < 0.001) and oligometastatic disease (χ2 = 13.902, P < 0.001). However, no statistical differences were found between the multimetastatic patients with lower-limb metastasis and those without lower-limb metastasis in terms of GS, according to the χ2 test (χ2 = 0.042, P = 0.837).
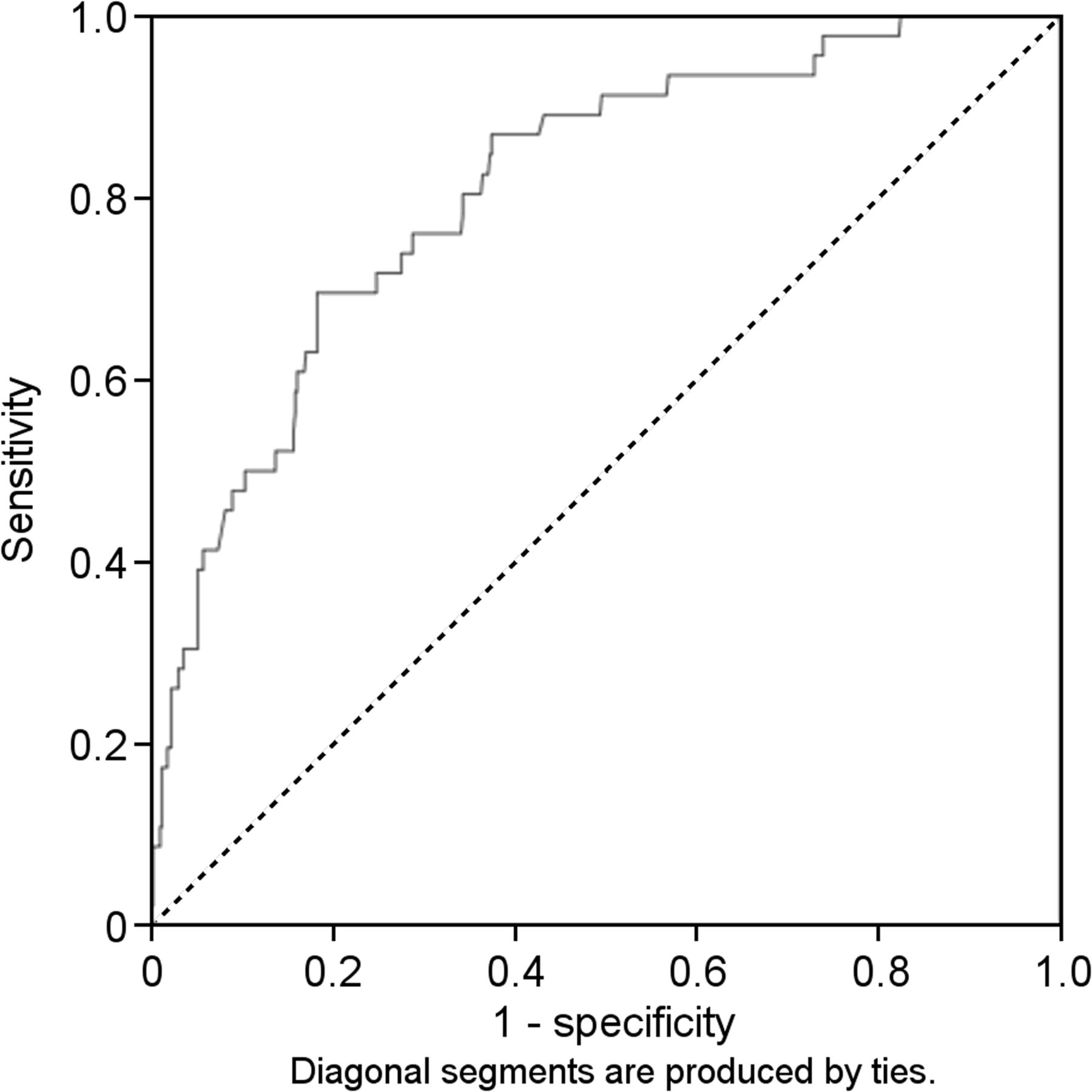
We evaluated the utility of PSA to diagnose lower-limb metastasis by a receiver-operating-characteristic curve analysis. The area under the curve (0.81; 95% confidence interval, 0.74–0.87) revealed that PSA has a good predictive value for detecting lower-limb metastasis. Using a PSA reference cutoff of 24 ng/mL, we could correctly detect lower-limb metastasis with 76.6% sensitivity and 72% specificity (Fig. 2). The results of 68Ga-PSMA PET/CT imaging and the distribution of metastasis are shown in Table 2.

Receiver-operating-characteristic curves for PSA.
Results of 68Ga-PSMA PET/CT Imaging
The effective doses for additional lower-limb CT scans were based on ICRP-103 weighting factors. The median dose for lower-limb CT scans was 2.33 mSv (range, 1.1–4.07 mSv).
DISCUSSION
Bone is the most common site of PC metastasis, representing over 80% of all cases, and is associated with a high risk of morbidity (3). Detection or exclusion of bone metastasis has clinical significance for the management and prognosis of patients (15). Bone scintigraphy is commonly used for the assessment of skeletal metastasis in PC (4,5). In possessing a high diagnostic power, 68Ga-PSMA PET/CT scans were recently proposed for PC imaging for the assessment of bone metastasis (6,7,10). However, scanning is generally limited to the area from the base of the skull to the upper thigh, in contrast to whole-body bone scintigraphy (11). A limited whole-body 68Ga-PSMA PET/CT scan is performed for 5–7 bed positions at 3–5 min per position, requiring a total time of 15–35 min. Lower-limb imaging is acquired for 5–7 bed positions, adding an extra 10–14 min of acquisition time per patient. Many nuclear medicine departments perform limited whole-body 68Ga-PSMA PET/CT scans in daily practice to decrease scanning time. Thus, bone metastasis of lower limbs can be missed on PET/CT scans because they fall outside the field of view.
In the literature, there are limited numbers of studies including whole-body 68Ga-PSMA PET/CT scans (6,16,17). Pyka et al. discussed the distribution of bone metastasis in PC by comparing bone scans and whole-body 68Ga-PSMA PET/CT scans in 126 patients (17). That study documented that there is a higher lower-extremity metastasis ratio in a whole-body 68Ga-PSMA PET/CT scan than in a bone scan, with data standing at 9.2% versus 7.9% retrospectively, thus supporting our idea. Because of limited data about the incidence of lower-extremity metastasis of PC, we have checked the results of previous studies that used bone scintigraphy and CT as an imaging modality for the detection of PC. The ratio of lower-limb metastasis was higher in the tibia and fibula than was seen in other studies (18,19). We thought that the superior resolution of the PET/CT may have been the reason for the detection of higher numbers of these lower-limb bone metastases. Overall, the detection of lower-extremity metastasis with 68Ga-PSMA PET/CT did not change the metastatic status of disease. Lower-limb metastasis was, at most, part of widespread metastasis in the whole body.
According to our results, none of the PC patients had any isolated lower-extremity metastasis. However, a limited number of PC cases with isolated lower-extremity metastasis have been reported in literature (20–23). According to previous reported hypotheses, metastasis may spread to the lower extremities through the Batson plexus, during thermal changes, as a result of trauma, or by hemodynamic factors (24,25). In this present study, lower-limb metastasis was mostly seen in both symptom-positive groups and patients with high PSA levels (>24 ng/mL). Thus, the use of additional lower-limb imaging may be considered in symptomatic patients, when high PSA levels cannot be explained by a limited whole-body 68Ga-PSMA PET/CT scan alone.
Skeleton-related issues, such as pathologic fractures and spinal cord compression, have great importance in terms of morbidity (26). The weight-bearing bones (such as the proximal femurs or lumbar vertebrae) are the areas that pose the highest risk, and these are sufficiently scanned in limited whole-body 68Ga-PSMA PET/CT (27). In this current study, none of the patients with lower-extremity metastasis had pathologic fractures during follow-up. Patients with symptomatic and at-risk weight-bearing bone metastasis were treated with analgesics, bisphosphonates, and external radiotherapy. The presentation of lower-extremity metastasis on additional 68Ga-PSMA PET/CT scans has not affected the therapeutic approach significantly (besides the exposure of the patient to additional radiation). However, if patients present symptoms suggestive of lower-limb metastasis, additional 68Ga-PSMA PET/CT imaging may show lower-extremity metastasis that could be treated with palliative therapies. On the basis of our results, we presume that symptom-positive, multimetastatic patients with a higher PSA level (>24 ng/mL) are at a higher risk of developing lower-limb metastasis.
The main limitation of the present study was its retrospective nature. Additionally, for ethical reasons, histologic confirmation of metastasis was mostly unavailable. Imaging results were therefore used instead.
CONCLUSION
To our knowledge, this is the first report that evaluates additional lower-limb 68Ga-PSMA PET/CT imaging for PC over a large patient population. According to our results, lower-limb imaging did not change the metastatic status of disease, nor did it affect the therapeutic approach significantly. However, if multimetastatic patients present relevant symptoms for lower-limb metastasis, it could be beneficial to consider including lower-limb imaging for possible palliative therapies.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Apr. 24, 2019.
REFERENCES
- Received for publication December 2, 2018.
- Accepted for publication February 20, 2019.





{kind=link}
{kind=link}