


Abstract
A 25-y-old woman with known neurofibromatosis type 1 and a large anterior mediastinal mass was investigated. 18F-FDG PET/CT revealed a radiotracer-avid anterior mediastinal mass having an SUVmax of 4.3 and demonstrating a hypoactive center. The 123I-metaiodobenzylguanidine SPECT/CT study performed subsequently did not demonstrate any uptake, thereby excluding, for the most part, the diagnosis of paraganglioma or neuroblastoma. At final pathology, a malignant peripheral nerve sheath tumor of the pericardium with areas of chondrosarcomatous and angiosarcomatous differentiation was diagnosed.
- malignant peripheral nerve sheath tumors
- neurofibromatosis type 1
- pericardium
- anterior mediastinum
- FDG
- PET/CT
We report the case of a woman with known neurofibromatosis type 1 and a large anterior mediastinal mass in whom the combination of 18F-FDG and 123I-metaiodobenzylguanidine allowed us to correctly orient the diagnosis toward a primary malignant tumor of the pericardium and characterize its heterogeneity.
CASE REPORT
A 25-y-old woman with known neurofibromatosis type 1 came to the emergency room complaining of palpitations and chest pain. The initial work-up, including thoracic CT, revealed a large pericardial collection. After pericardiocentesis, a large anterior mediastinal mass was demonstrated by cardiac ultrasound, leading to further investigation.
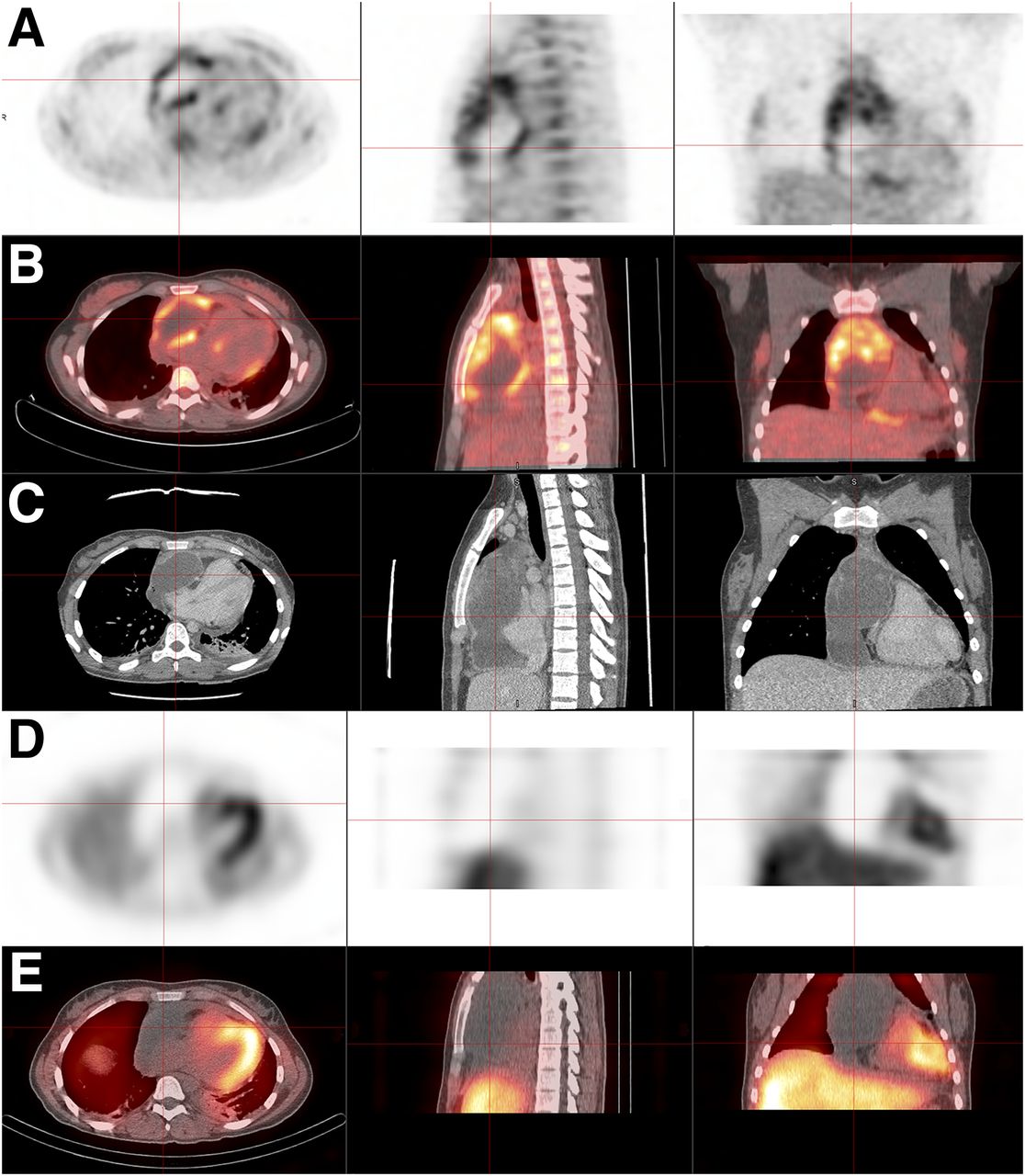
18F-FDG PET/CT images (Figs. 1A and 1B), along with corresponding slices of a contrast-enhanced thoracic CT (Fig. 1C), revealed a radiotracer-avid anterior mediastinal mass having an SUVmax of 4.3 and demonstrating a hypoactive center. The tumor-to-liver ratio was measured at 2.85. The mediastinal mass was deemed malignant on the basis of these findings. No distant active lesion was detected.
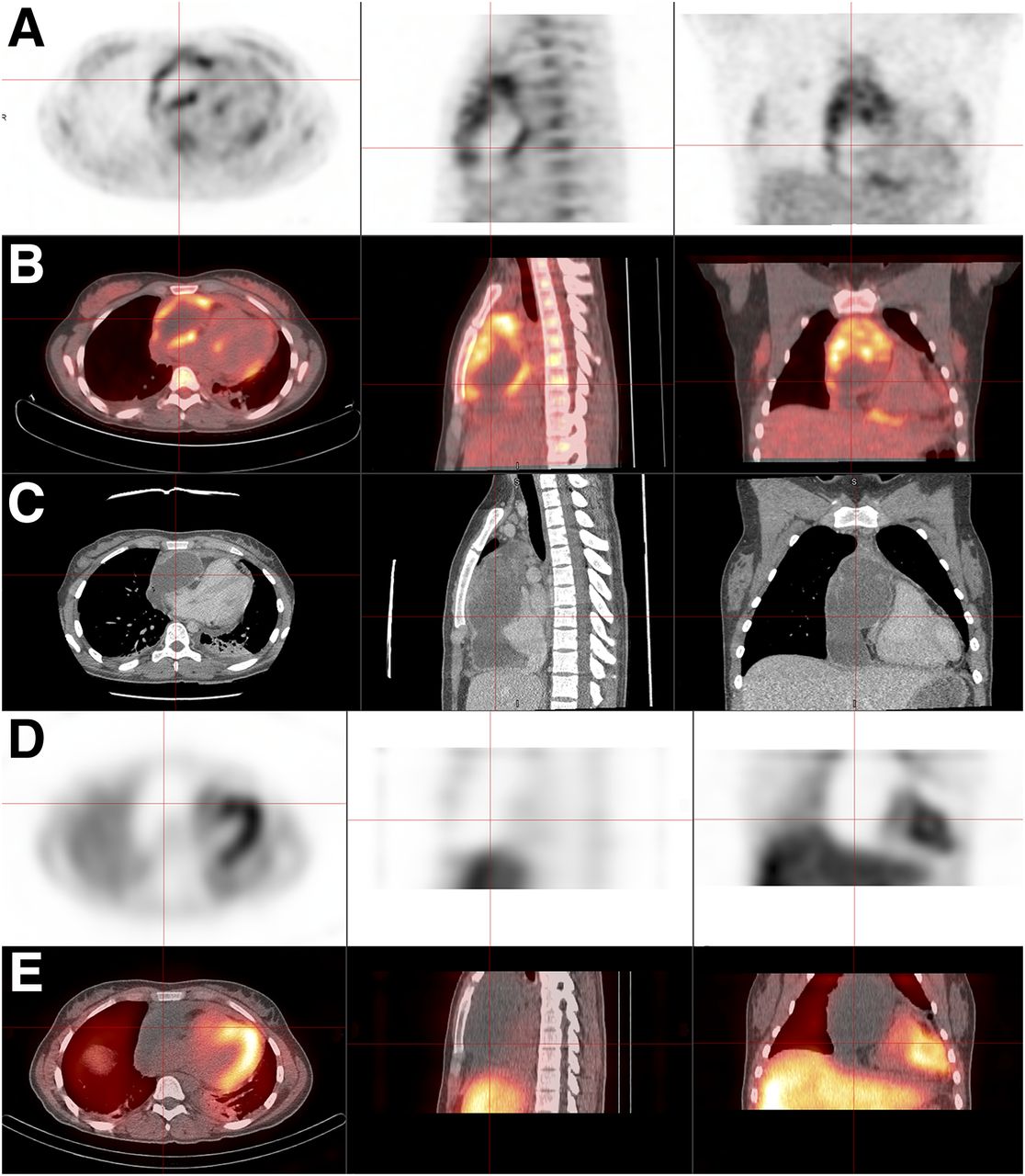
18F-FDG PET (A), PET/CT (B), and CT (C) reveal radiotracer-avid anterior mediastinal mass with hypoactive center. 123I-metaiodobenzylguanidine SPECT (D) and SPECT/CT (E) show no radiotracer uptake by mediastinal mass.
The 123I-metaiodobenzylguanidine SPECT/CT study (Figs. 1D and 1E) performed subsequently did not demonstrate any radiotracer uptake by the mediastinal mass, thereby excluding, for the most part, the diagnosis of paraganglioma or neuroblastoma.
At final pathologic examination of the surgically removed lesion, a malignant peripheral nerve sheath tumor of the pericardium with areas of chondrosarcomatous and angiosarcomatous differentiation was diagnosed.
DISCUSSION
Neurofibromatosis patients carry up to a 10% lifetime risk of developing a malignant peripheral nerve sheath tumor, although this type of tumor is rare in the general population (<0.1%) (1). 18F-FDG PET/CT was found to be highly sensitive and specific for the diagnosis of malignant peripheral nerve sheath tumor in neurofibromatosis type 1 patients (1–3). Warbey et al. reported a sensitivity of 0.97 and specificity of 0.87 using a cutoff SUVmax of 3.5 (4). Salamon et al. proposed a tumor-to-liver ratio of more than 2.6 as being more specific (5). Both criteria were met in our case.
CONCLUSION
The combination of 18F-FDG and 123I-metaiodobenzylguanidine allowed us to correctly orient the diagnosis toward a primary malignant tumor of the pericardium and characterize its heterogeneity.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Nov. 10, 2017.
REFERENCES
- Received for publication July 26, 2017.
- Accepted for publication September 11, 2017.





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.