


Abstract
A 38-y-old woman with metastatic breast carcinoma reported seeing “halos and flashes” in her left eye. Funduscopic examination revealed an elevated mass in the choroid of the left globe consistent with metastasis. Subsequent 18F-FDG PET/CT revealed focal uptake in the nasal aspect of the left choroid of the eye corresponding to the mass seen on the funduscopic examination. Through correlation with the PET/CT study, the lesion was retrospectively identified on MRI. The fact that 18F-FDG PET/CT after radiotherapy showed a complete response supports the use of this imaging modality for diagnosis and monitoring of response. A history of breast cancer and visual symptoms should trigger the nuclear medicine physician to take extra care in reading the initial slices of the PET/CT scan through the orbits in order to make this challenging imaging diagnosis.
The use of 18F-FDG PET/CT for follow-up and monitoring of response in patients with breast cancer has been increasing (1,2). A large study found that 47% of orbital metastases are from breast cancer but less than 1% of breast cancers metastasize to the orbit (3,4). The most common site of orbital metastasis is the choroid (88%) (3). Although rare at initial staging, orbital metastases from breast cancer typically develop years after diagnosis, with one study reporting a median of 8.5 y after diagnosis (4).
CASE REPORT
A 38-y-old woman with infiltrating ductal carcinoma underwent neoadjuvant chemotherapy followed by bilateral mastectomy and radiation. Staging 18F-FDG PET/CT demonstrated no distant metastases. Three years later, the level of serum tumor marker increased. 18F-FDG PET/CT then revealed widespread metastatic disease in the lymph nodes, lungs, bone, skin, and left choroid.
18F-FDG PET/CT showed focal 18F-FDG activity with an SUVmax of 5.0 in the nasal choroid of the left eye, consistent with choroidal metastasis (Figs. 1A and 1B). A fluid attenuation inversion recovery MRI sequence demonstrated subtle thickening of the left nasal choroid (Fig. 1C).
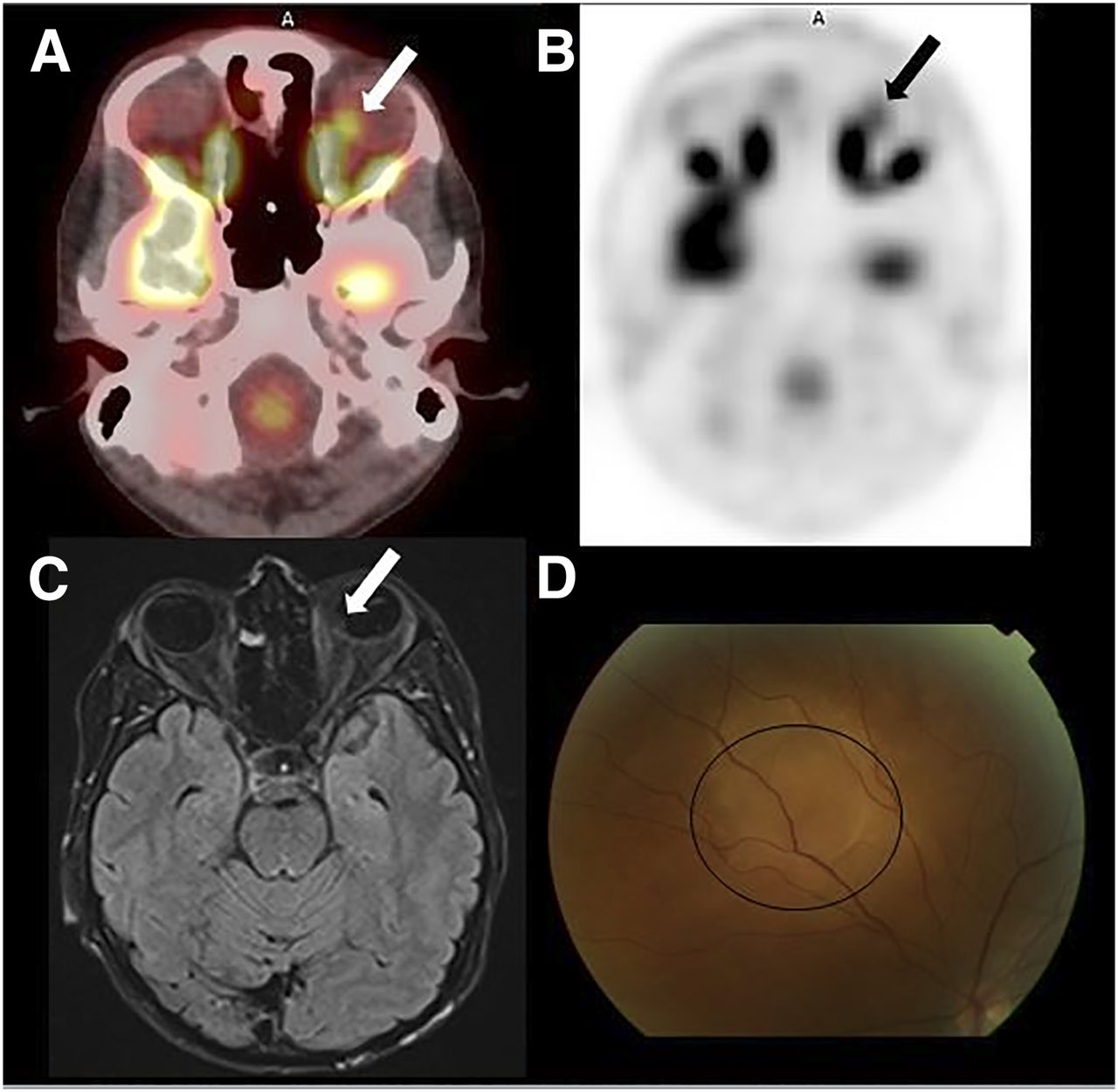
Pretreatment imaging. (A–C) Fused PET/CT (A), axial 18F-FDG PET (B), and axial fluid attenuation inversion recovery MRI (C) showed focus of 18F-FDG uptake and thickening in left nasal choroid (arrows). (D) Photograph of fundus revealed elevated 6-mm lesion in left nasal choroid (circle).
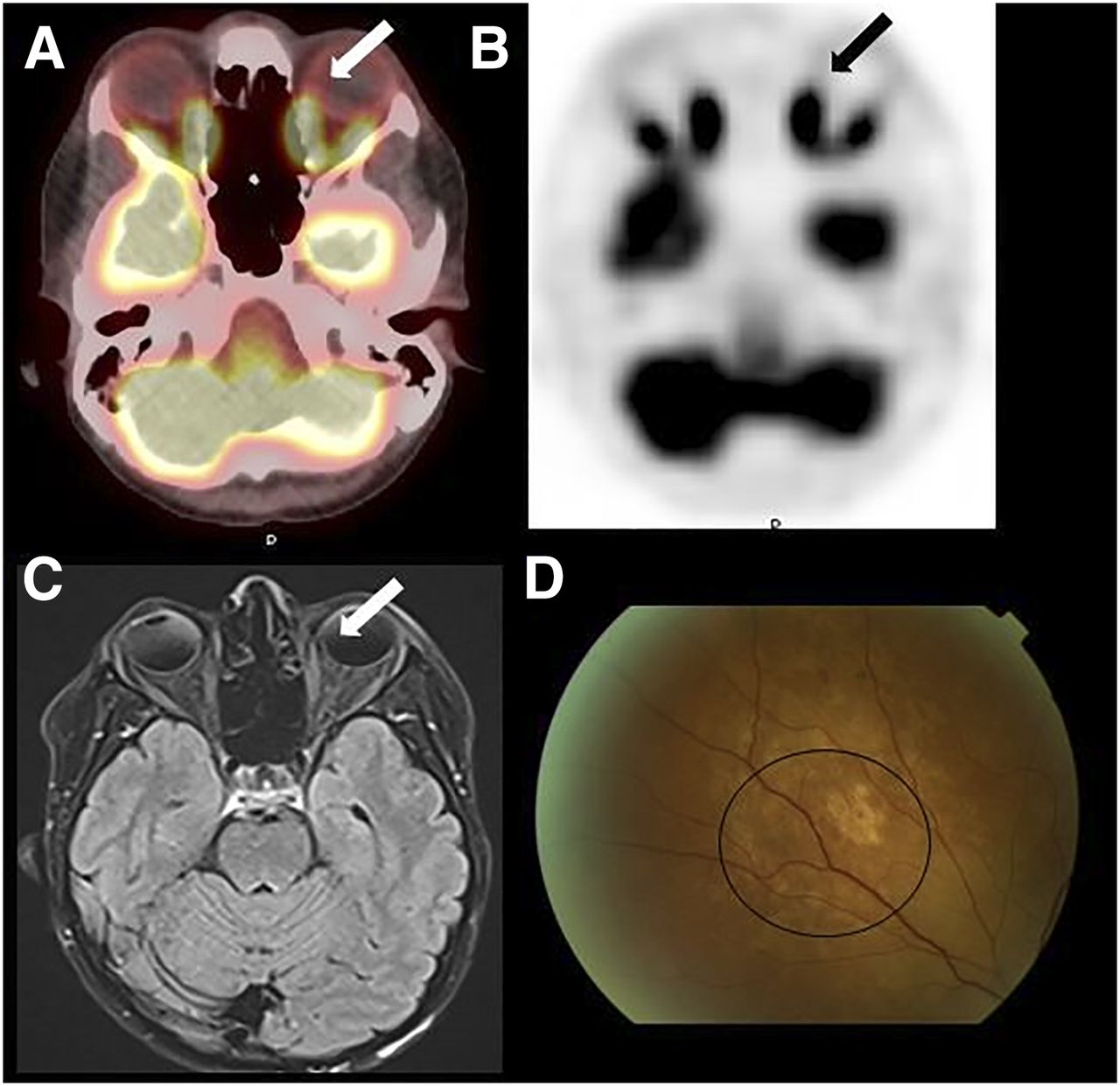
Radiation therapy is the treatment of choice for choroidal metastases from breast cancer, and this patient underwent intensity-modulated radiation therapy (5). 18F-FDG PET/CT and MRI 3 mo after radiation therapy demonstrated resolution of the lesion (Figs. 2A–2C). Fundoscopy demonstrated flattening and regression of the choroidal mass with residual atrophic pigmentary changes in the overlying retinal pigment epithelium as typically seen after radiation therapy (Fig. 2D).
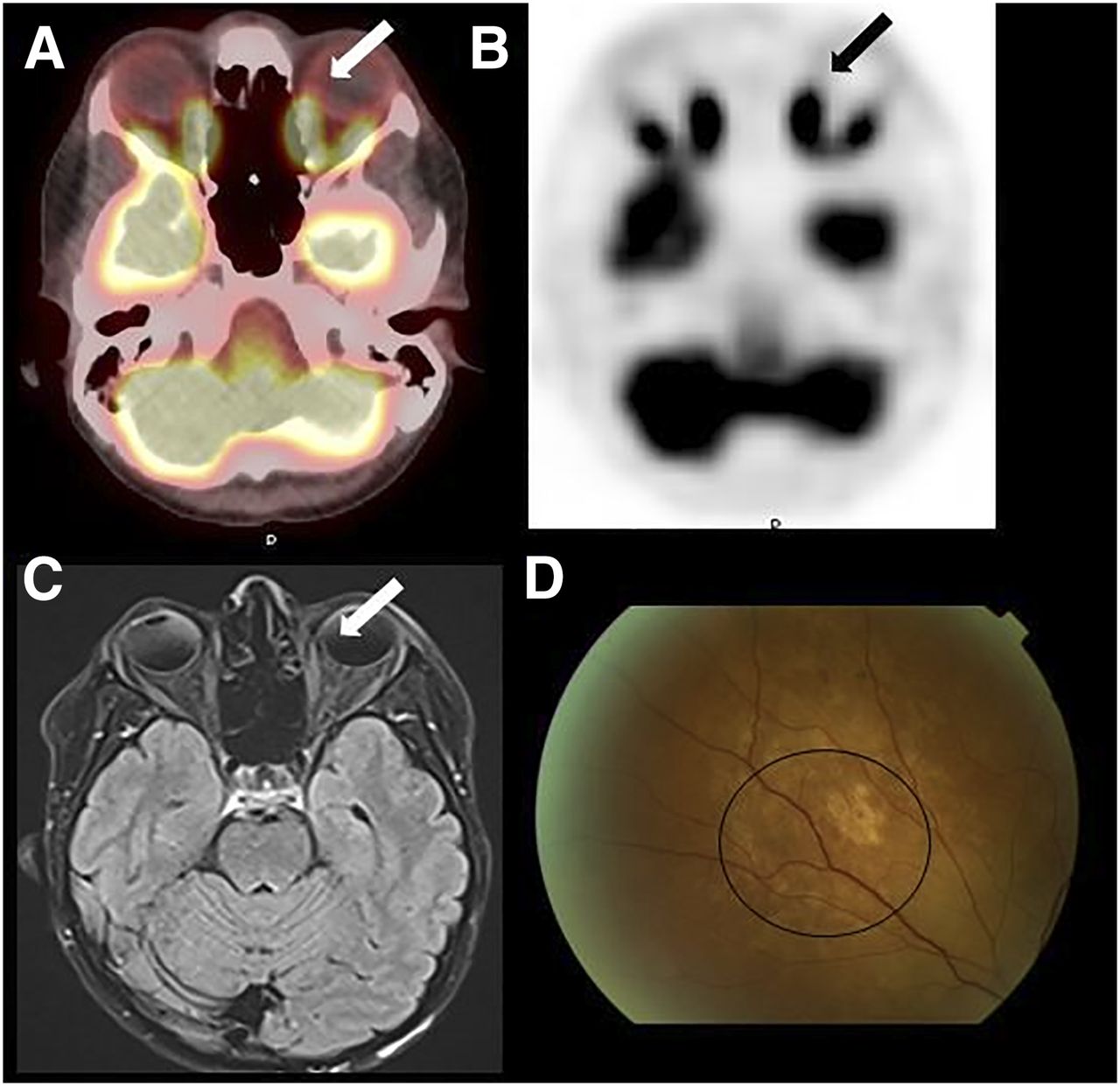
Posttreatment imaging. (A–C) Fused PET/CT (A), axial 18F-FDG PET (B), and axial fluid attenuation inversion recovery MRI (C) showed resolution of focus of 18F-FDG uptake and choroidal thickening in left nasal choroid (arrows). (D) Photograph of fundus revealed regression of choroidal mass (circle).
DISCUSSION
Since breast cancer is the most common etiology of orbital metastasis, technologists must ensure that the orbits are included in the field of view for all breast cancer patients. Physiologic uptake in extraocular muscles and the small size of choroidal metastases can make the diagnosis challenging. Therefore, the history of breast cancer and visual symptoms should trigger the nuclear medicine physician to take extra care in reading the initial slices of the PET/CT scan through the orbits.
CONCLUSION
18F-FDG PET/CT can detect and monitor response to therapy for choroidal metastasis.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Nov. 10, 2017.
- Received for publication July 31, 2017.
- Accepted for publication August 28, 2017.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.