


Abstract
We present a case study in which artifacts from collimator contamination and patient motion were seen on a bone scan. Any identified artifact must be further investigated and documented so as to detect its source and thus prevent its future occurrence.
Radioactive contamination and image artifacts can be introduced at any time during a nuclear scan. Contamination leads to unwanted radiation exposure to patients, caregivers, and staff, as well as interrupting the acquisition schedule (1).
We report a case of collimator contamination and motion artifact that occurred during a bone scan. Our purpose is to describe the pattern of this artifact so as to help nuclear medicine technologists and physicians identify it.
CASE STUDY
A 55-y-old man with a known case of prostate carcinoma underwent whole-body bone scanning to check for skeletal metastases. A 740-MBq injection of 99mTc-methylene diphosphonate was given intravenously, and delayed whole-body anterior and posterior planar images from the skull to the feet were acquired on a dual-head SPECT system (Hawkeye 4; GE Healthcare).
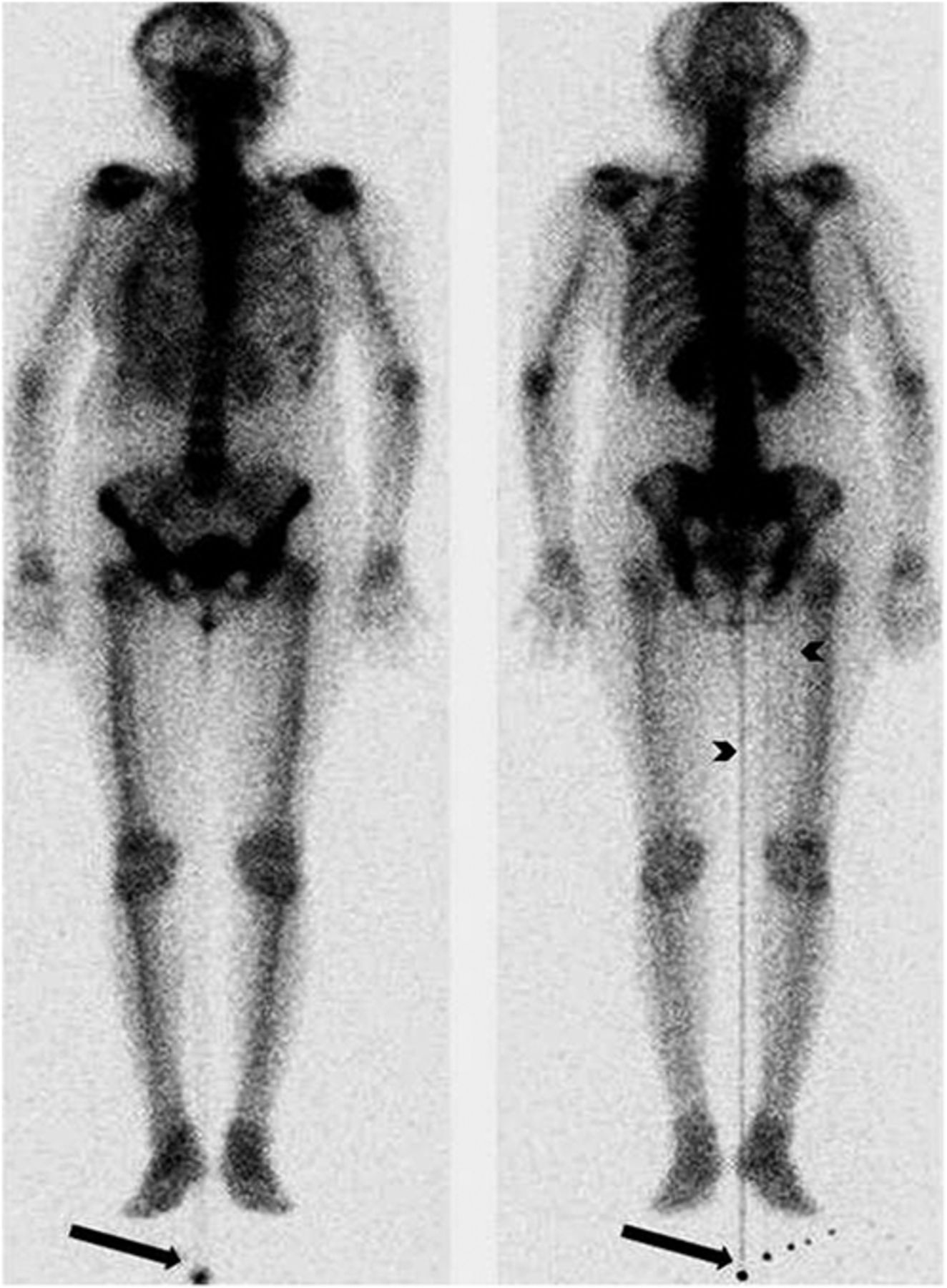
The images revealed 3 abnormal foci of radiotracer outside the body contour near the right foot, predominantly in the posterior projection. Well-defined linear tracer activity was also noted arising from these extracorporeal tracer foci, most prominently in the center of body but also faintly at the medial aspect of the right thigh. In addition, there was blurring of the head-and-neck region on both anterior and posterior images because the patient had moved during the acquisition (Fig. 1).

Anterior (left) and posterior (right) whole-body bone scans revealing contamination foci (arrows) from which arises well-defined linear activity, most prominently in center of body and also faintly at medial aspect of right thigh (arrowheads). Motion artifact in head-and-neck region is also seen.
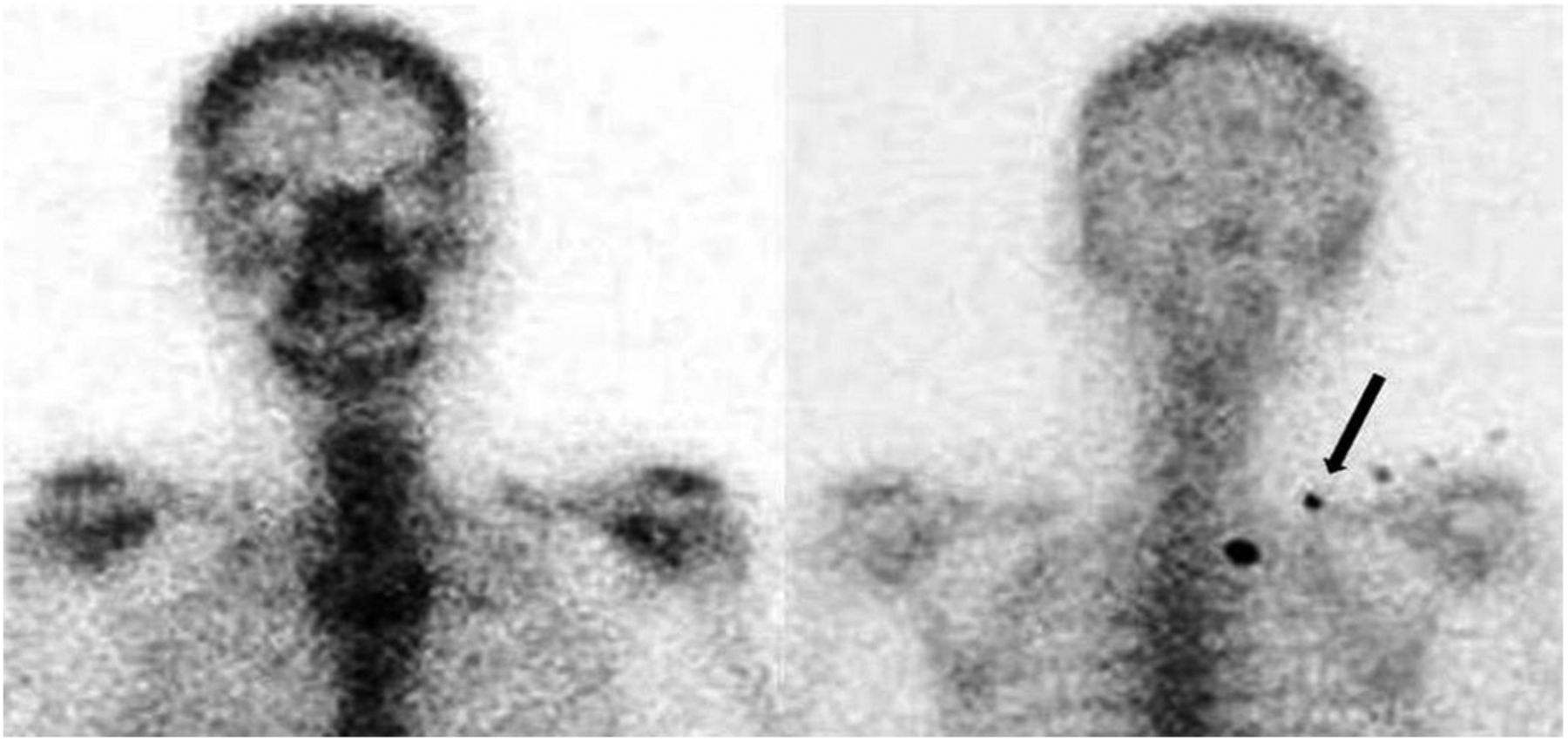
A spot image of the head, neck, and thorax was acquired with the patient in head-first supine position to correct the motion artifact. As we changed the orientation of the patient from feet-first supine to head-first supine, the foci of abnormal update that had been seen outside the body contour near the right foot were now seen in the right upper thoracic region around the first and second ribs. Though false-positive, this finding might be reported as metastatic disease if not scrutinized adequately (Fig. 2).
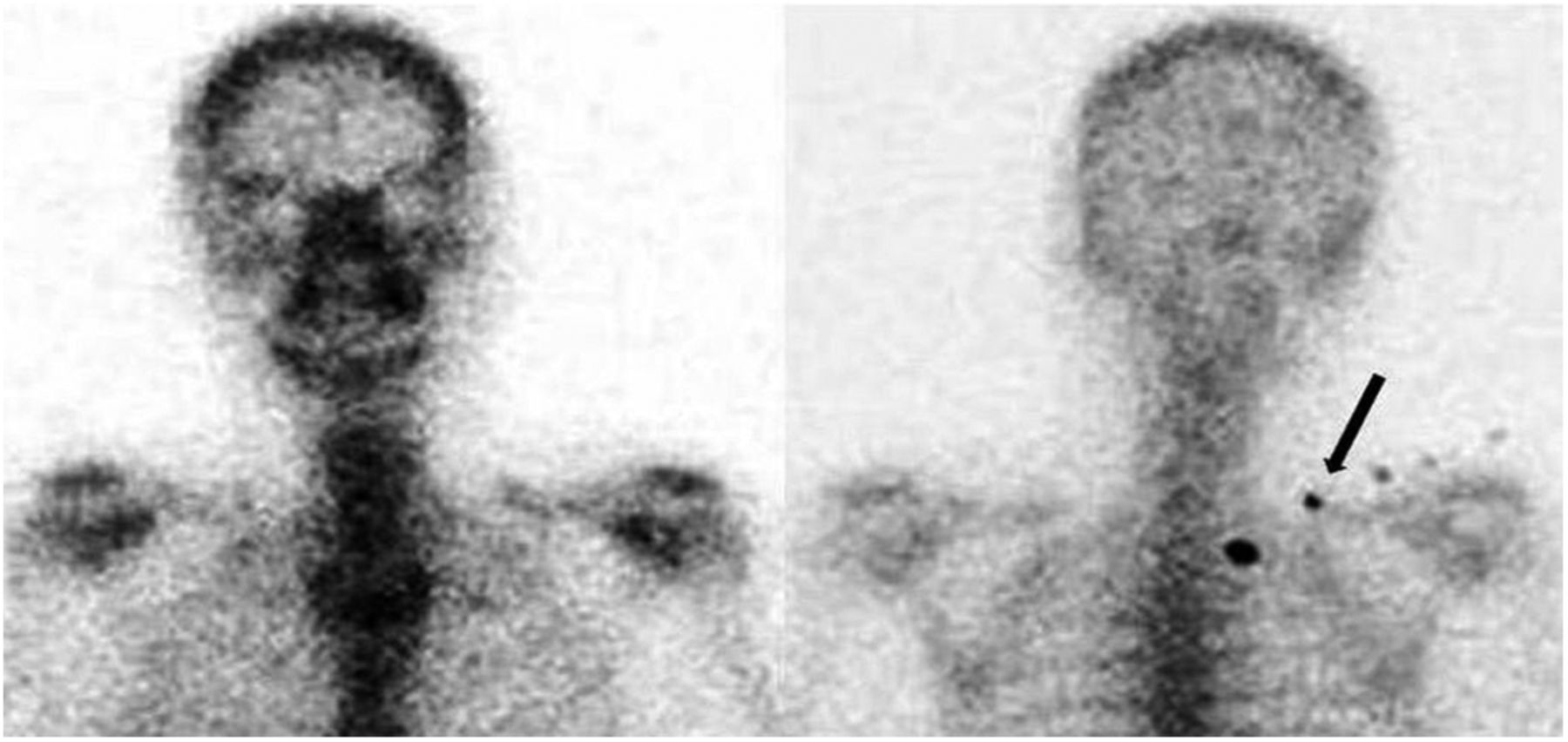
With patient in head-first supine position, there is no motion artifact in spot static anterior (left) or posterior (right) images of head, neck, and thorax, but contamination that was seen beside right foot previously is now seen in right upper thoracic region (arrow).
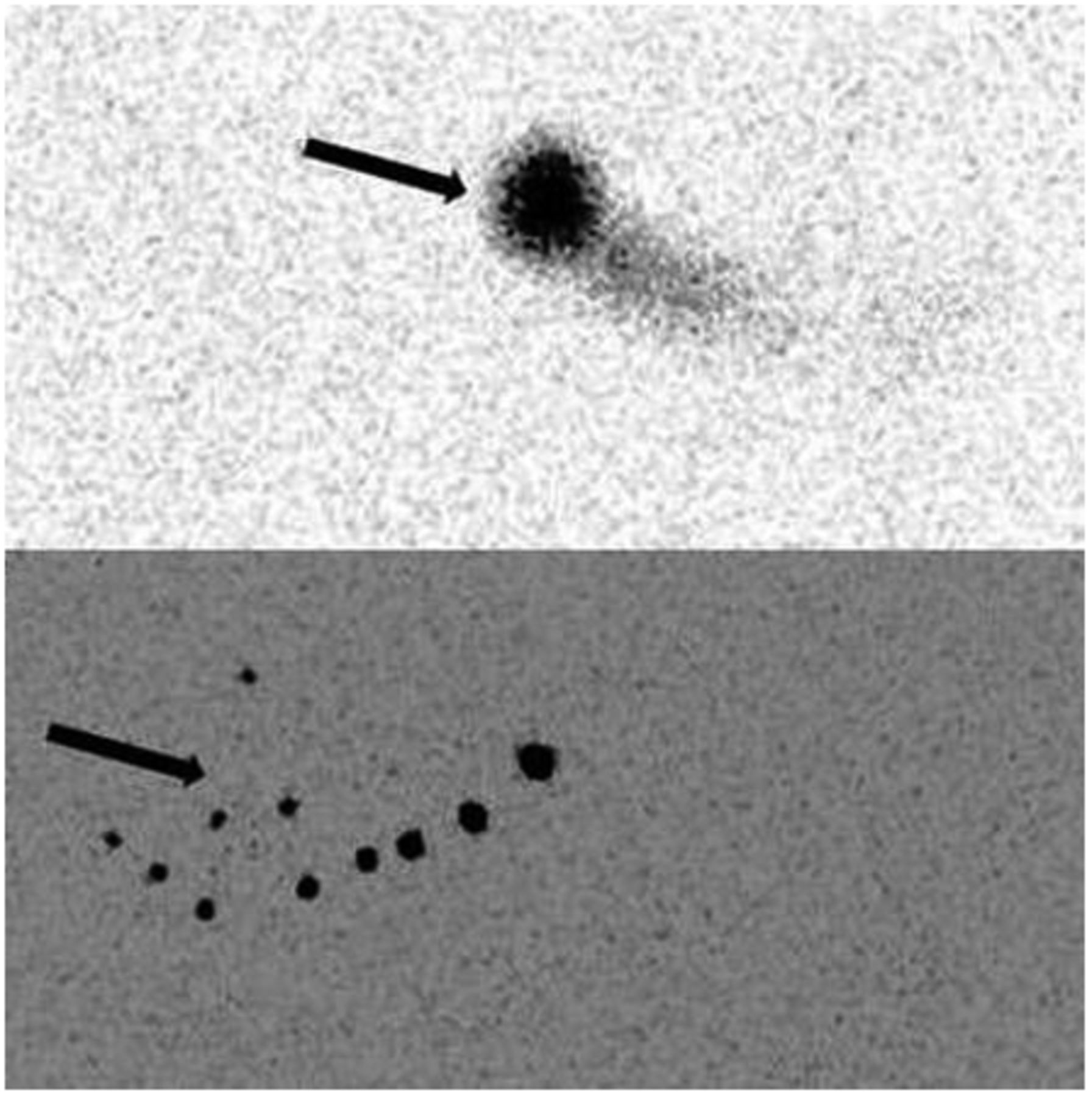
The patient was then removed from the camera and images of the collimators alone were acquired, with the two collimators facing each other. The bright foci of tracer were well evident on these images (posterior > anterior) and hence were determined to be due to contamination of the collimators (Fig. 3).

Anterior (top) and posterior (bottom) images obtained without patient and table reveal multiple foci of contamination (arrows) on collimators, more prominent in posterior image.
DISCUSSION
Contamination can be categorized as either directly patient-related, such as contamination of the clothing or hair, or indirectly patient-related, such as contamination of the patient’s surroundings (camera detectors, floors, sink, dustbins). Patient contamination can be identified easily during image acquisition, but because surrounding contamination cannot be so easily identified, daily wipe tests are mandatory (2).
Interpretation of a nuclear scan can be affected by many kinds of technical errors during its acquisition, as well as by injection artifacts, prosthetic implants, patient motion, and extracorporeal contamination such as that of the patient’s clothes, the table, or the collimator (1). The possibility of false-positive results due to technical errors or contamination should always be kept in mind, especially if the lesions are prominent in a single projection (3).
Contamination of the detector or collimator usually involves a limited area and appears as a line throughout whole-body images (3). Detector contamination differs from direct patient contamination; in the latter, the location of the radiotracer changes with movement of the patient, whereas in the former, the location remains static. In our case, the observed contamination of the collimators was suspected to be due to urinary spillage during the direct radionuclide cystogram that had been performed just before the bone scan.
Patient motion is also a common source of artifacts in images but usually can easily be detected by cine displays, sinograms, and summed planar images. To avoid any discomfort-induced motion artifacts, the technologist should ensure that the patient is comfortably positioned during the image acquisition. If needed, an arm support, holding straps, and sandbags may also be used to reduce patient movement during the acquisition (4).
Care should be taken to avoid contamination and other artifacts, as they interrupt the workflow of nuclear medicine technologists and physicians (because of the time needed for cleaning and decontamination) and expose patients to additional radiation (because of the need to repeat the imaging study).
CONCLUSION
Nuclear medicine technologists—usually being the first to encounter an instance of a potential artifact—must have a thorough knowledge of such problems and the experience to identify them. Nuclear medicine physicians also need to have a sound knowledge of such sources of error and the ability to differentiate a false-positive finding from a true pathologic abnormality. Proper training programs and designation of duties is of the utmost importance for the personnel in a nuclear medicine facility to avoid and manage radioactivity-related accidents such as artifacts. Any identified artifact must be investigated as to its source and documented to prevent its future occurrence.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Apr. 13, 2017.
REFERENCES
- Received for publication January 24, 2017.
- Accepted for publication April 1, 2017.





{kind=link}
{kind=link}
{kind=link}