


Abstract
This study aimed to determine whether a bismuth-coated latex shield (B-shield) could protect the eyes during brain SPECT/CT. Methods: A shield containing the heavy metal bismuth (equivalent to a 0.15-mm-thick lead shield) was placed over a cylindric phantom and the eyes of a 3-dimensional brain phantom filled with 99mTc solution. Subsequently, phantoms with and without the B-shield were compared using SPECT/CT. The CT parameters were 30–200 mA and 130 kV. The dose reduction achieved by the B-shield was measured using a pencil-shaped ionization chamber. The protective effects of the B-shield were determined by evaluating relative radioactivity concentration as well as artifacts (changes in CT number), linear attenuation coefficients, and coefficients of variation on SPECT images. Results: The radiation doses with and without the B-shield were 0.14–0.77 and 0.36–1.93 mGy, respectively, and the B-shield decreased the average radiation dose by about 60%. The B-shield also increased the mean CT number, but only at locations just beneath the surface of the phantom. Streaks of higher density near the underside of the B-shield indicated beam hardening. Linear attenuation coefficients and the coefficients of variation did not significantly differ between phantoms with and without the B-shield, and the relative 99mTc radioactivity concentrations were not affected. Conclusion: The B-shield decreased the radiation dose without affecting estimated attenuation correction or radioactivity concentrations. Although surface artifacts increased with the B-shield, the quality of the SPECT images was acceptable. B-shields can help protect pediatric patients and patients with eye diseases who undergo SPECT imaging.
SPECT/CT is a medical imaging technology that combines SPECT and CT. The CT imaging provides accurate nonuniform attenuation correction for SPECT images of the brain when the position of the head is fixed in a holder. Consequently, integrated SPECT/CT systems enable the collection of accurate qualitative and quantitative dopamine transporter images (1,2). However, the CT procedure increases the radiation dose to the patient, especially to the eye lens, which is among the most radiosensitive tissues in humans (3). From this viewpoint, the International Commission on Radiological Protection has recommended a threshold of 500 mGy for the dose absorbed by the eye lens (4,5). Accordingly, various techniques have been used to reduce the radiation dose delivered by CT (6–8). Widely used approaches include tube current control and automated exposure control (9), iterative reconstruction (10), and shielding of organs (11). Although automated exposure control and iterative reconstruction have good potential to reduce the radiation dose while maintaining image quality, these are not available in all systems. On the other hand, superficial organs have been protected with bismuth-coated latex shields (B-shields) which have a reasonable cost and suitable attenuation characteristics. Hein et al. (12) reported that such shields can reduce the surface radiation dose by 40% during paranasal CT. In addition, Hopper et al. (13) reported that B-shields can decrease the average radiation dose by 48.5%. These findings indicate that B-shields might also be useful during SPECT/CT imaging. However, the effects of B-shields on brain SPECT/CT images have not been investigated, especially the accuracy of attenuation correction and SPECT image quality.
The purpose of this study was to assess whether B-shields can be used to protect the eyes during brain SPECT/CT imaging. We evaluated the quality of brain SPECT/CT images acquired when a B-shield was used and the ability of the shield to reduce the radiation dose.
MATERIALS AND METHODS
SPECT/CT Instrument, Phantoms, and B-Shield
We acquired and reconstructed all images using a Symbia T2 dual-head hybrid SPECT/CT camera (Siemens AG) equipped with a low-energy, high-resolution collimator. The CT component is the same as that for the Sensation scanner (Siemens AG). The radiation dose was measured using a CT dose index phantom, and SPECT image quality was assessed using a cylindric phantom (diameter, 16 cm; height, 15 cm) and a 3-dimensional (3D) brain phantom (14) containing a solution of 99mTc (activity, 32.8 or 45.8 kBq/mL). A in-house–developed flexible shield containing bismuth (equivalent to a 0.15-mm-thick lead shield) was placed over the surface of the phantom and shaped to cover both eyes.
Dose Measurements
We measured the radiation dose at the top area of the CT dose index phantom with and without the B-shield (Fig. 1) using a pencil-shaped ionization chamber (Toyo Medical Co.). The eye lens equivalent dose should ideally be assessed at a depth of 3 mm, but the value more commonly used is at a depth of 70 μm or 1 cm, and this is within 10% of the actual value. Therefore, the ionization chamber was inserted at a 1-cm depth in the CT dose index phantom. The phantom was assessed by CT using the parameters 130 kVp, 30–200 mA, 2 × 0.5-mm collimation, 0.8-s rotation time, 5-mm slice thickness, and a pitch value of 0.95. The radiation dose reduction caused by the B-shield was calculated as where Dosebismuth and Dosecont represent radiation doses with and without the B-shield, respectively. The measurements were repeated 5 times for each CT scan.
where Dosebismuth and Dosecont represent radiation doses with and without the B-shield, respectively. The measurements were repeated 5 times for each CT scan.

Phantom with B-shielding. (A) CT dose index (CTDI) phantom with B-shielding placed over surface. (B) Pencil-shaped ionization chamber positioning.
Evaluation of Image Quality
Data Acquisition and Reconstruction
SPECT/CT data were acquired with and without the B-shield using both cylindric and 3D brain phantoms. Projection data were obtained in continuous mode with rotation through 120 angular views. The pixel size was 3.3 × 3.3 mm (scale for enlargement, 1.45) with a 128 × 128 matrix. The total acquisition time was 20 min (10 repetitions of 2 min/cycle). A photopeak of 99mTc was set as a 21% energy window centered at 140 keV. A low subwindow to correct multiple-energy-window scatter was set at 7% on the bottom of the photopeak window (116–124 keV). All CT images were acquired using the same parameters as in the dose measurement.
All phantom images were reconstructed using ordered-subset expectation maximization with resolution recovery, and both scatter correction and CT-based attenuation correction were derived from the current in the CT tube. The reconstruction parameters were 15 iterations, 6 subsets, and 3D gaussian filtering of 8.6 mm in full width at half maximum as postsmoothing.
Data Analysis
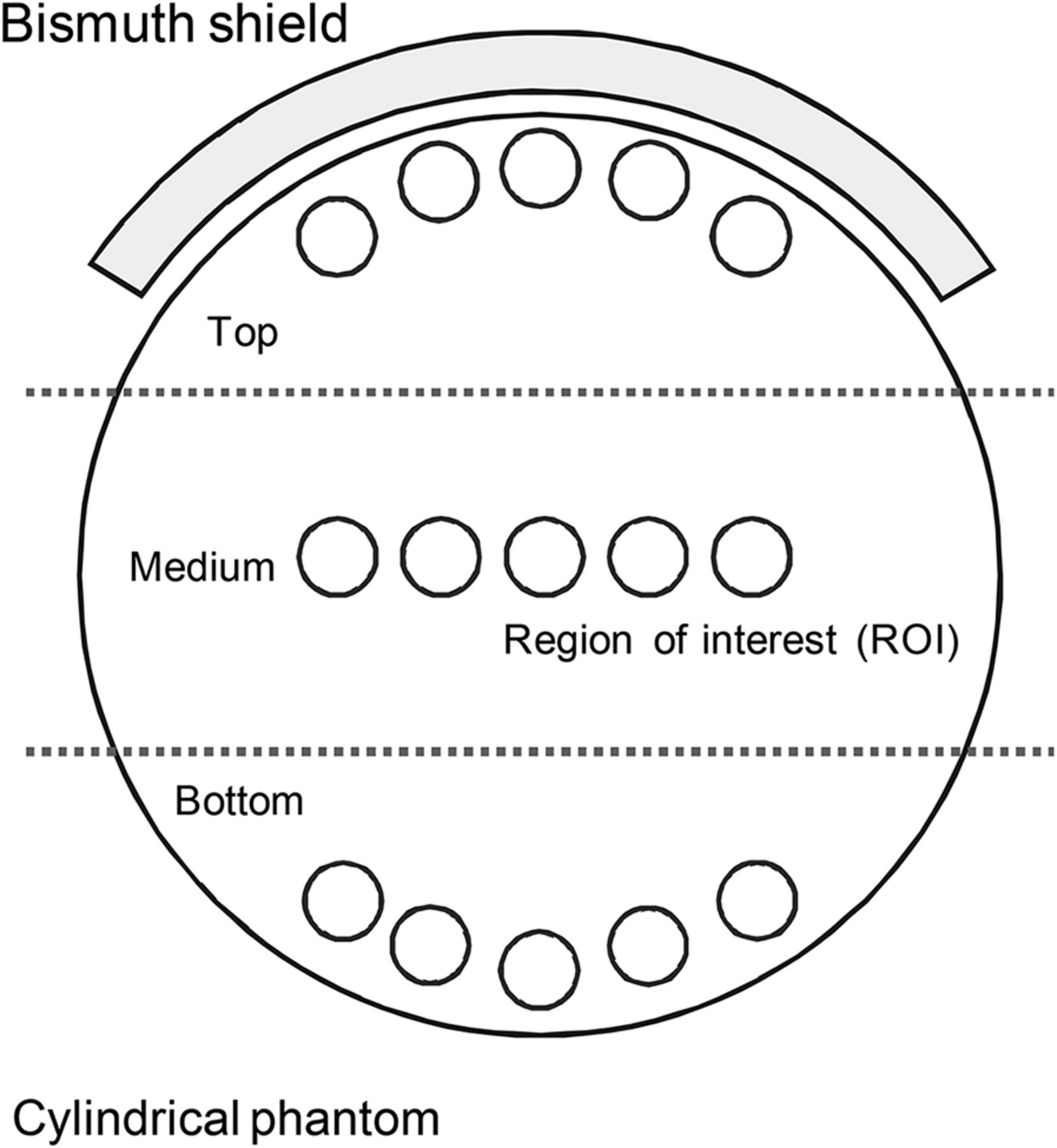
Five circular regions of interest (ROIs) were placed on the top, middle, and bottom of the CT images and the attenuation correction map (Fig. 2). The mean CT number and linear attenuation coefficients were then measured. The same ROIs were placed on the SPECT images, and the coefficient of variation (CV) was calculated as where the mean represents the mean count in the SPECT image ROI and SD is the SD of the ROI. We also investigated the effect of the B-shield on regional radioactivity by automatically placing ROI templates on 3D stereotactic ROIs (15). The anterior, precentral, central, parietal, angular, temporal, occipital, pericallosal, lenticular, thalamic, hippocampal, and cerebellar regions were used in the analysis. The difference in regional radioactivity was calculated as
where the mean represents the mean count in the SPECT image ROI and SD is the SD of the ROI. We also investigated the effect of the B-shield on regional radioactivity by automatically placing ROI templates on 3D stereotactic ROIs (15). The anterior, precentral, central, parietal, angular, temporal, occipital, pericallosal, lenticular, thalamic, hippocampal, and cerebellar regions were used in the analysis. The difference in regional radioactivity was calculated as where meanbismuth and meanref are the mean SPECT counts with and without B-shielding, respectively.
where meanbismuth and meanref are the mean SPECT counts with and without B-shielding, respectively.
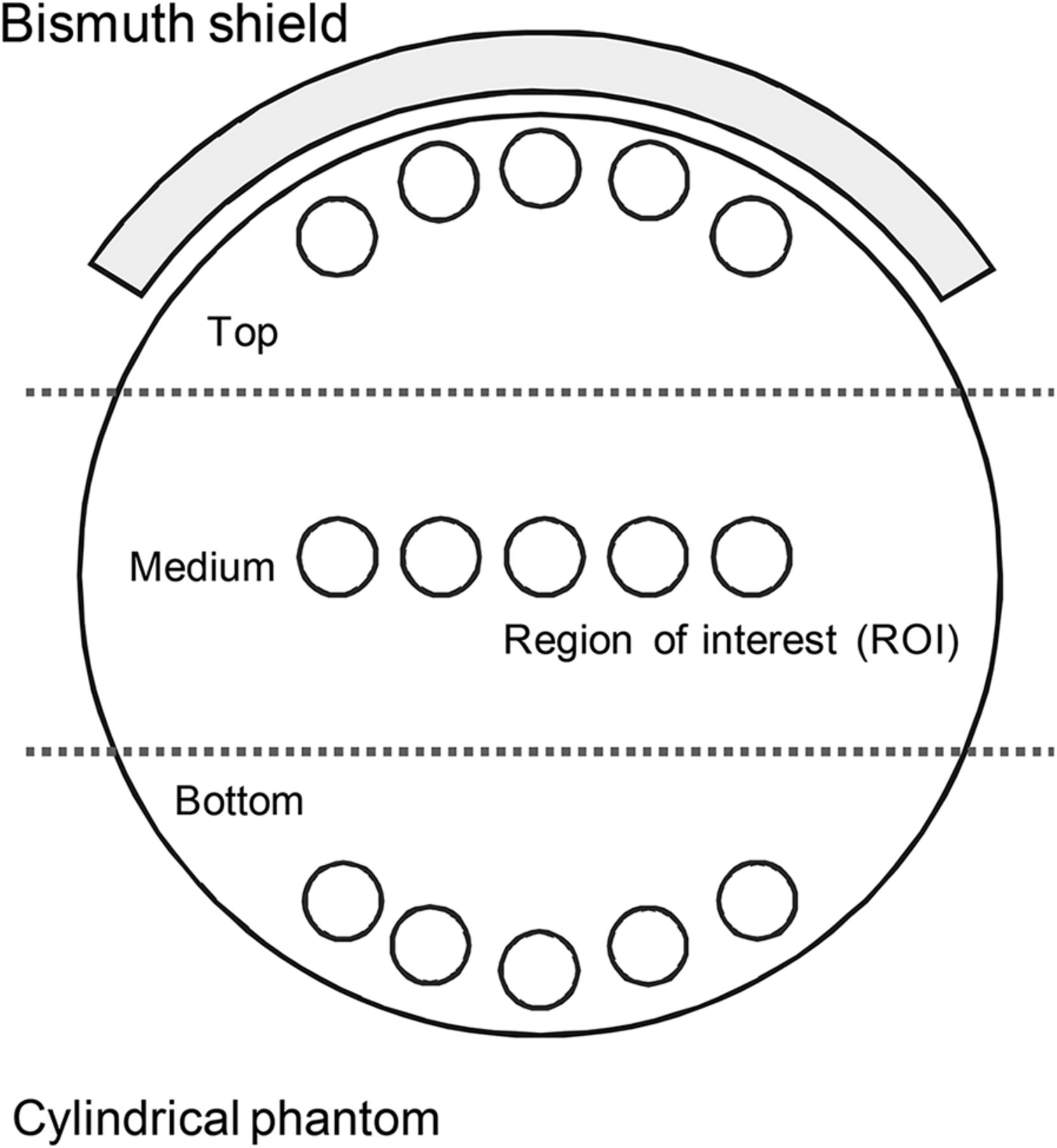
Images with ROI settings for evaluation. ROIs are placed at top, middle, and bottom of image.
Statistical Analysis
All data were compared using a paired t test, with a P value of less than 0.05 indicating a statistically significant difference.
RESULTS
Dose Measurement
The radiation doses and reduction values are shown in Table 1. The radiation dose was significantly lower (60.3% ± 0.5%) with the B-shield at each tube current.
Effect of B-Shielding on Radiation Doses
Image Quality
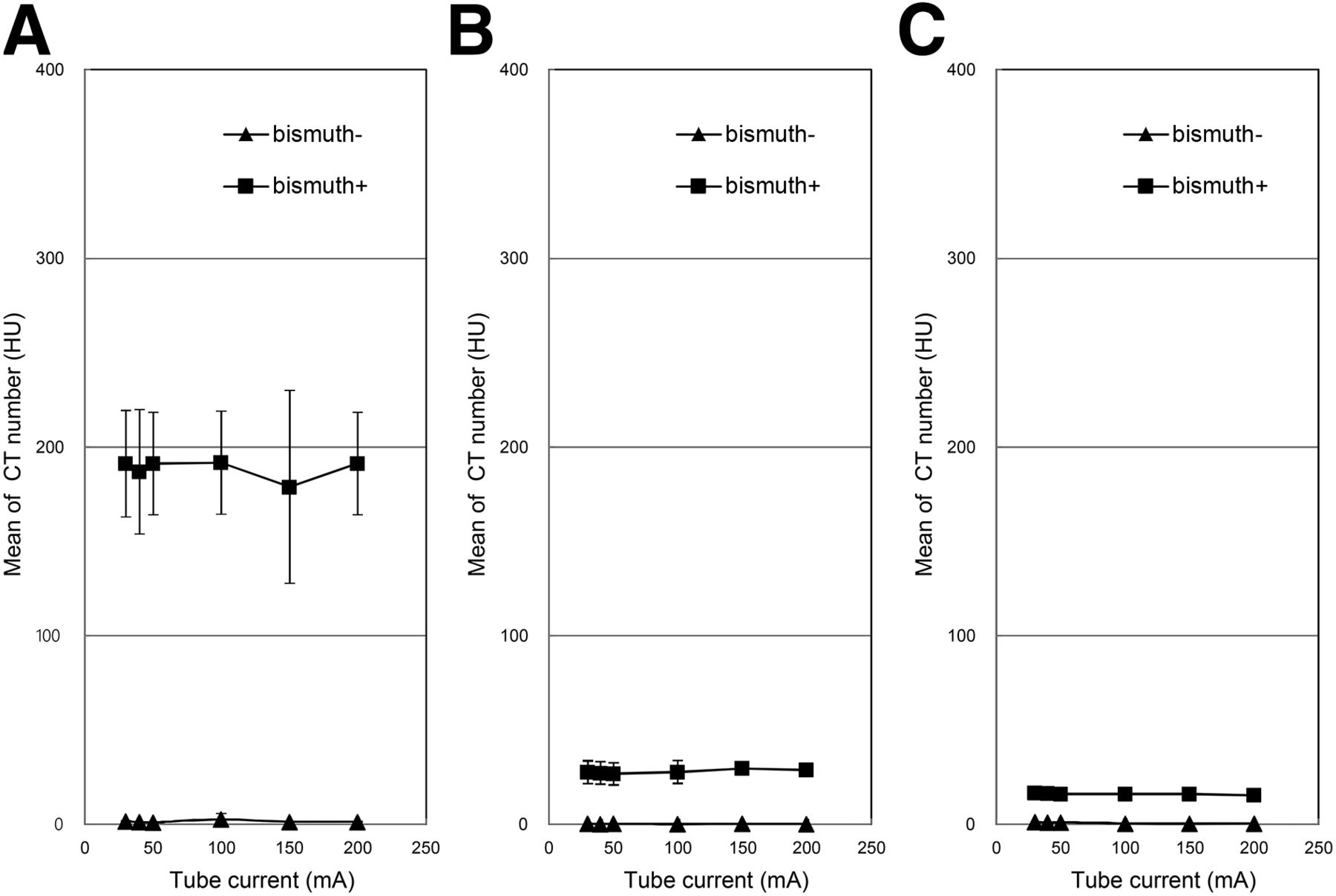
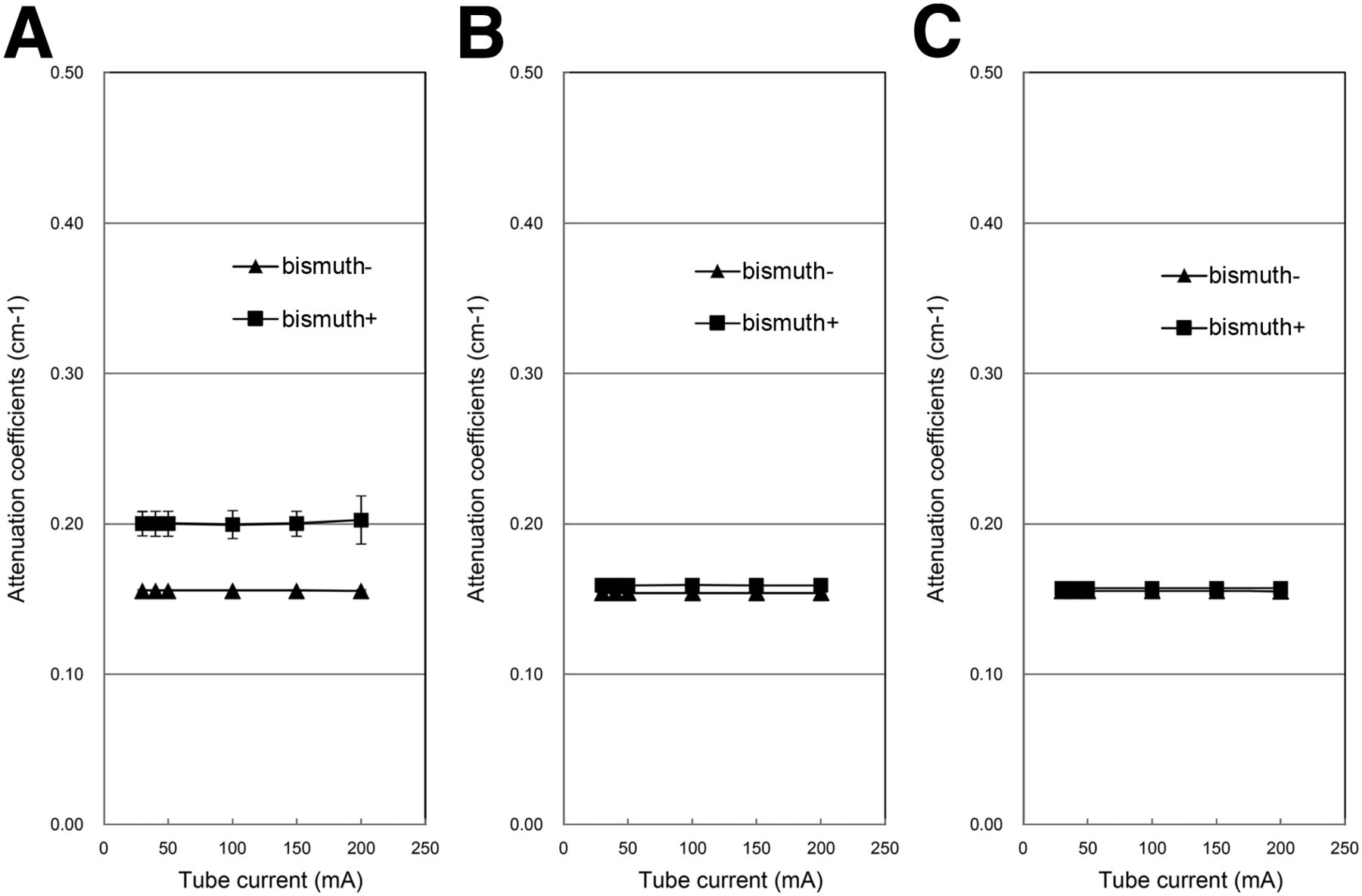
The mean CT number when using the B-shield was significantly increased at the top of the phantom (Fig. 3A) and slightly increased at the middle and bottom of the phantom (Fig. 3B). Figure 4 shows a comparison of linear attenuation coefficients with and without the B-shield. Although linear attenuation coefficients at the top of the phantom were increased when using the B-shield, changes could not be detected at the middle or bottom. The coefficient of variation of SPECT images with and without the B-shield are shown in Figure 5. The coefficients of variation were essentially constant, and no differences between the shielding and nonshielding conditions could be detected, especially at the middle or bottom of the phantom.
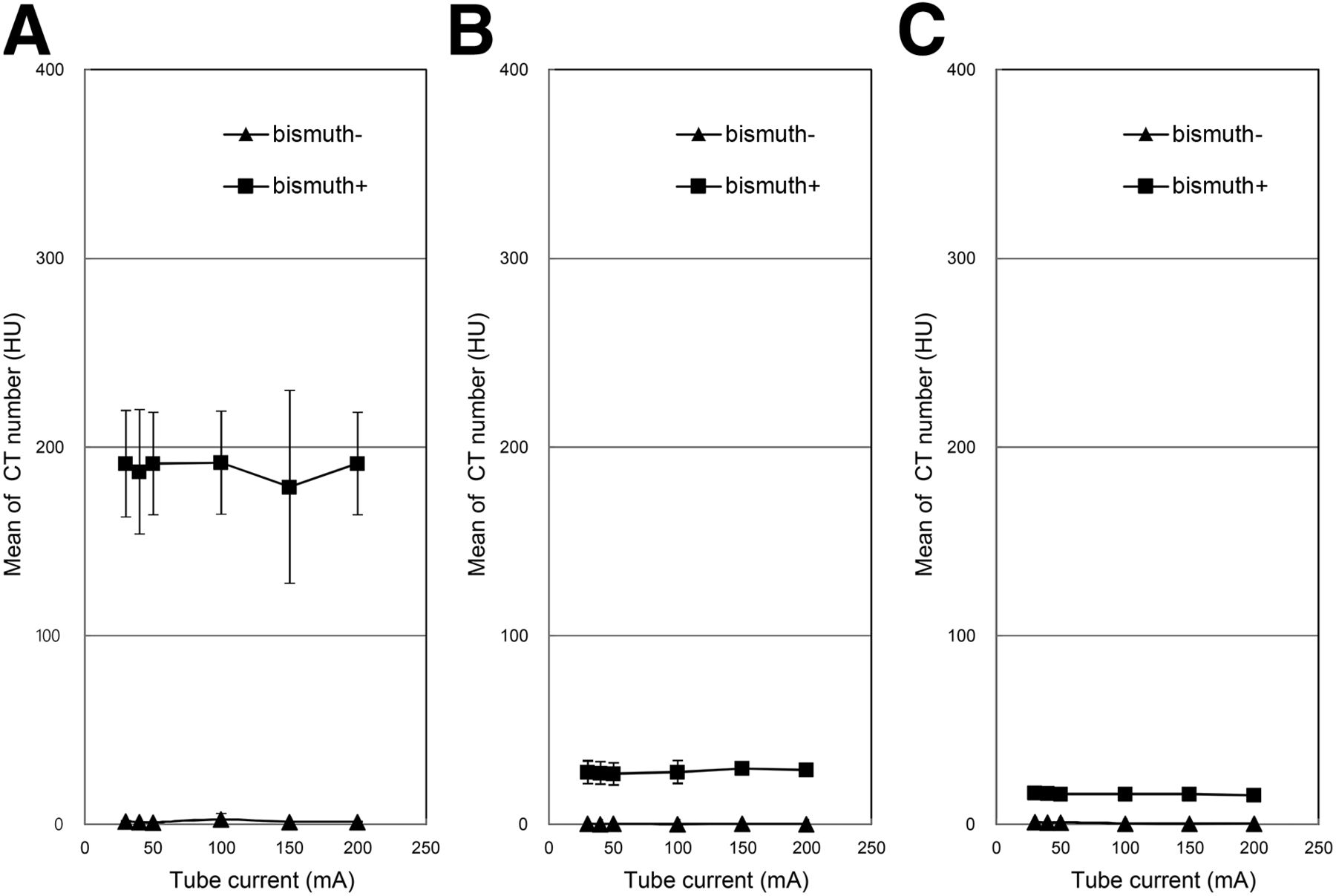
Mean of CT number determined on CT images as function of B-shielding at top (A), middle (B), and bottom (C) of image. Mean CT number generated with shielding is slightly higher at middle and bottom of image.
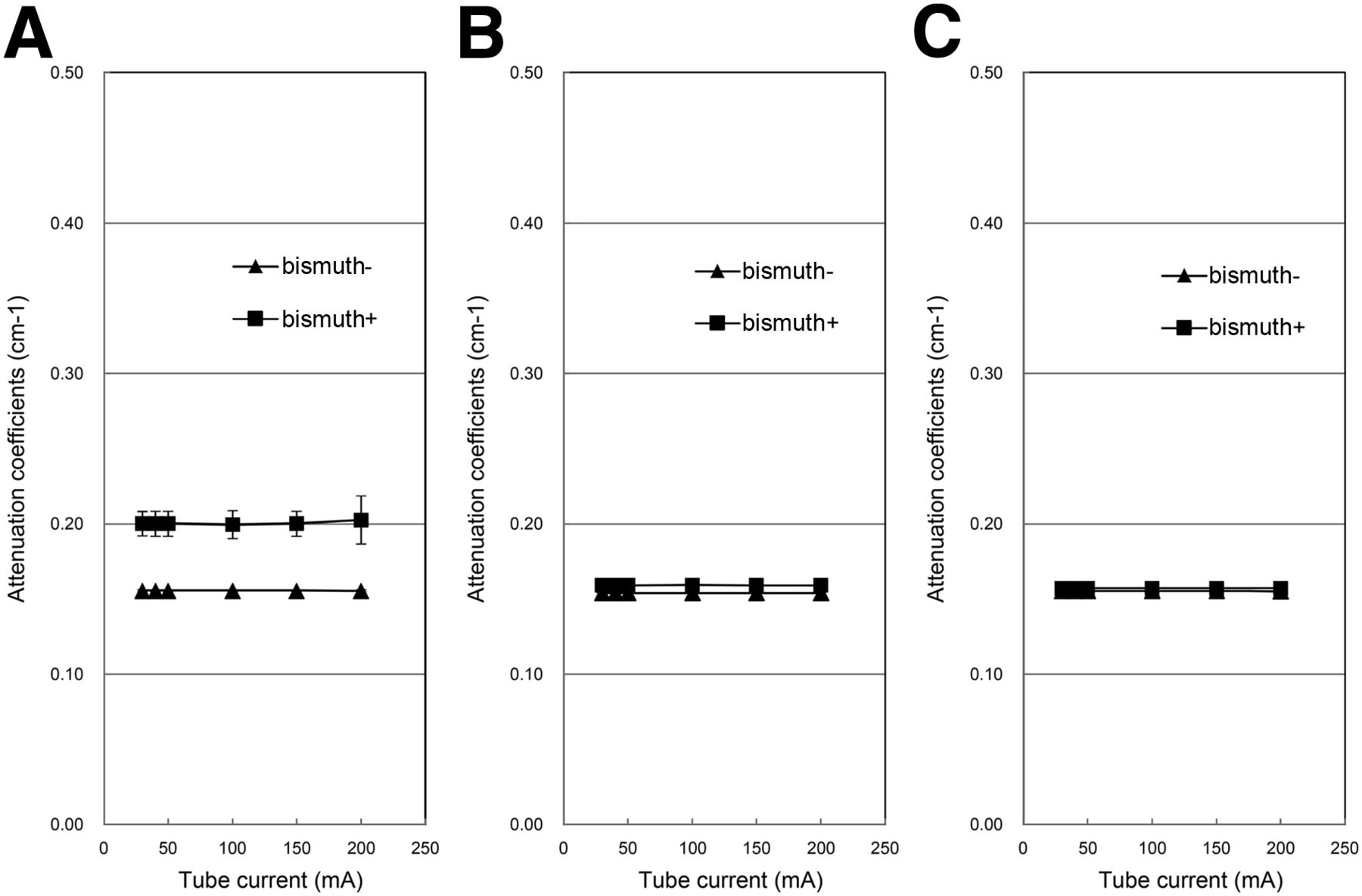
Comparison of attenuation coefficients with and without B-shielding at top (A), middle (B), and bottom (C) of image. Attenuation coefficients at middle and bottom of image are not significantly different with and without B-shielding.
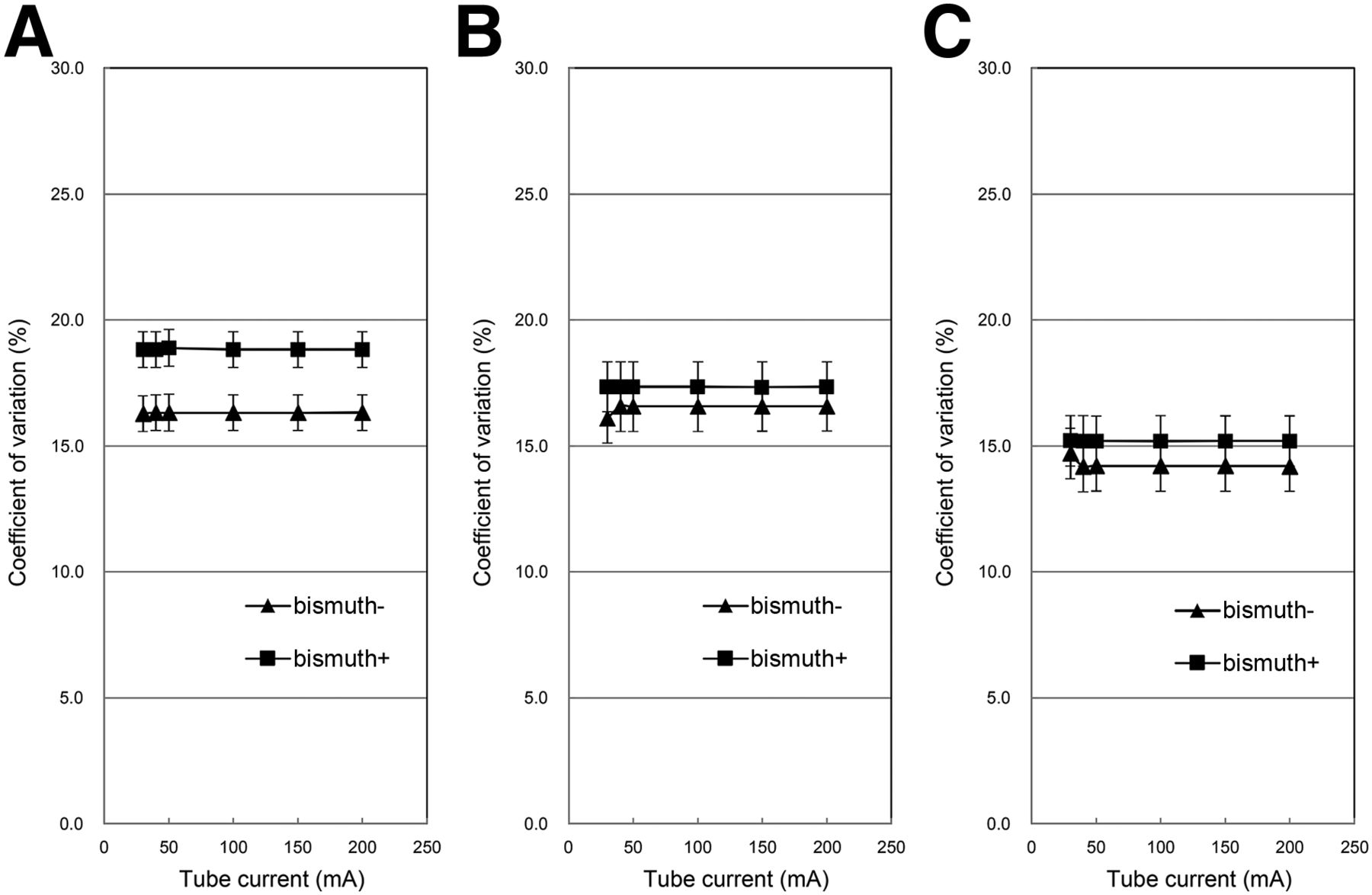
Coefficient of variation as function of B-shielding at top (A), middle (B), and bottom (C) of image. Coefficient of variation = SD/mean.
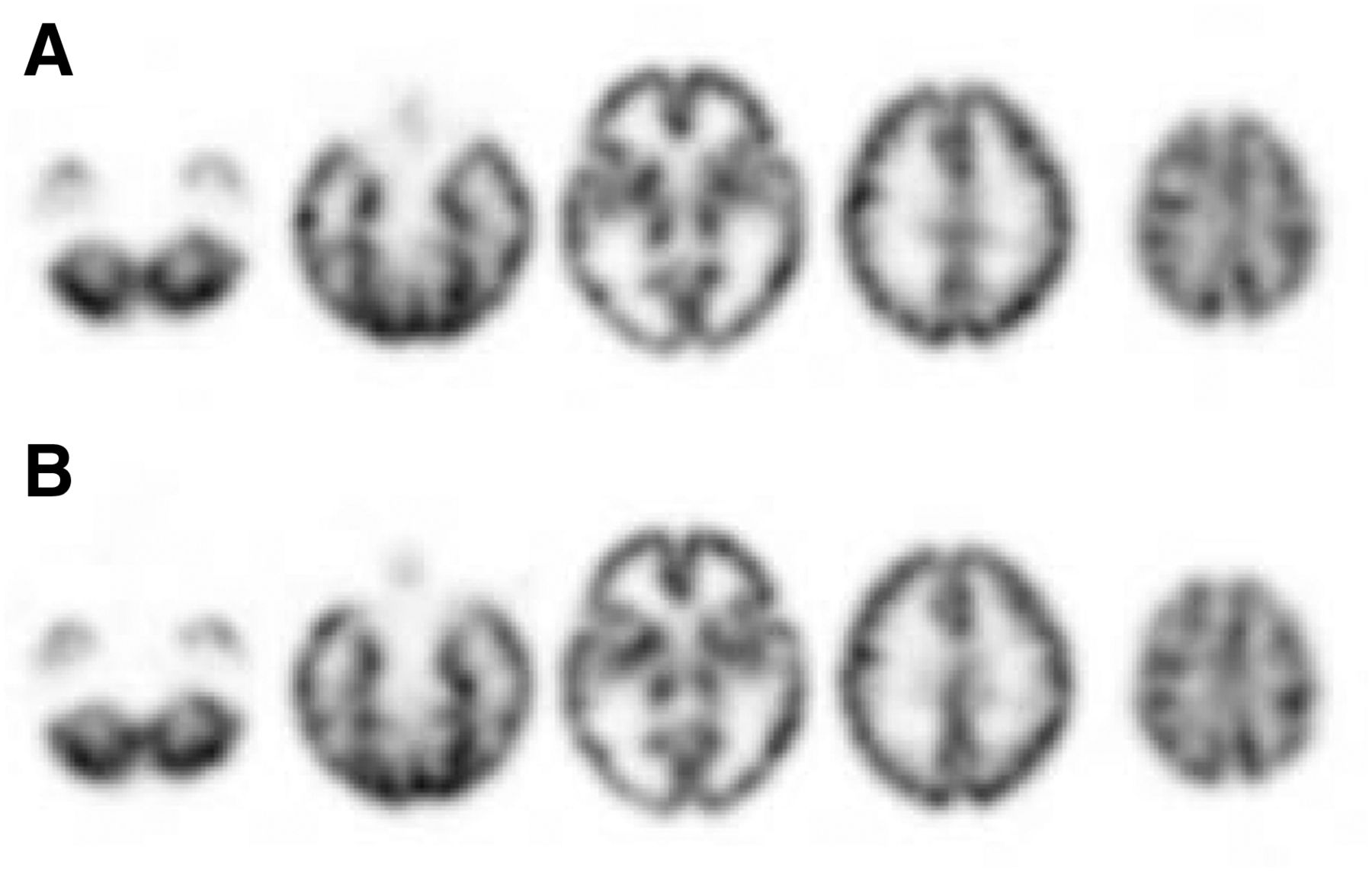
Figure 6 shows images acquired at tube currents of 50, 100, and 200 mA. For the 3D brain phantom, the radiation dose remained essentially the same with and without the B-shield. The difference in the radioactivity concentrations with and without B-shielding was the largest in the thalamus and was no more than 5.1% in any other region. Figure 7 shows that radioactivity concentrations on SPECT images were similar with and without the B-shield.
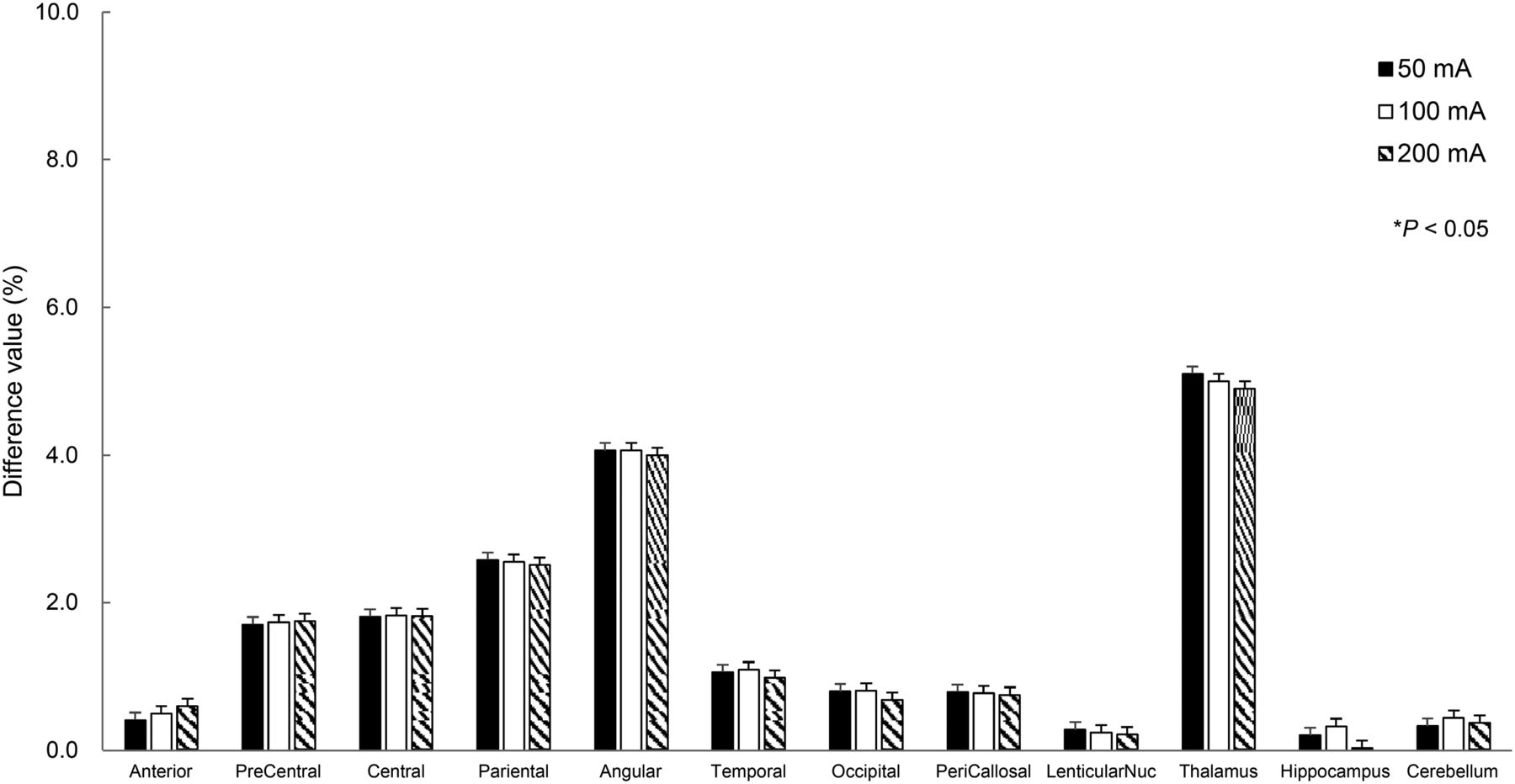
Comparison of regional radioactivity with and without B-shielding. Amounts of regional radioactivity do not differ significantly. Difference was highest in thalamus (5.1%).
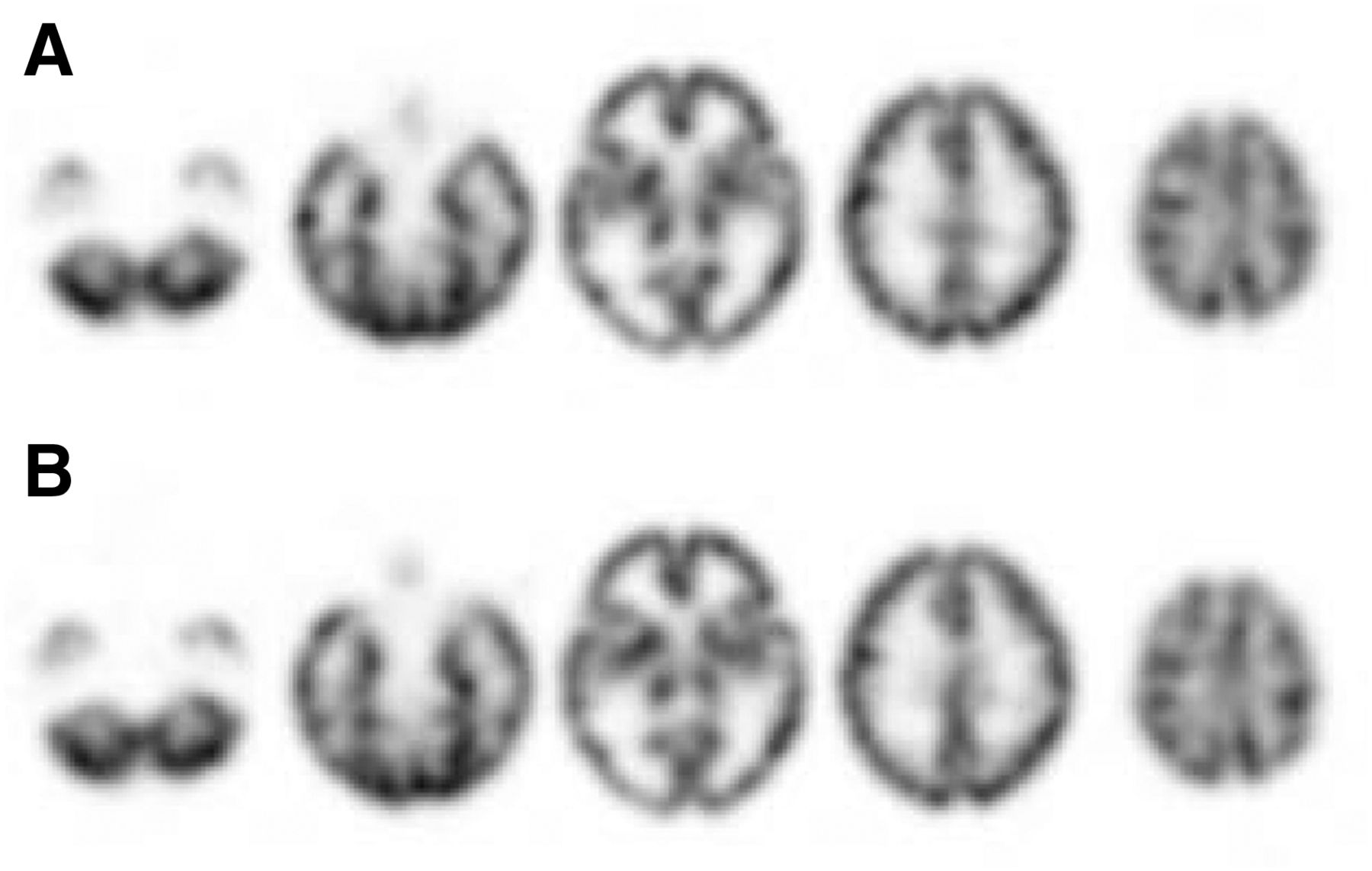
Examples of SPECT images acquired with B-shielding. (A) Reference image from 3D brain phantom. (B) Image acquired with B-shielding. Quality of both images is similar.
DISCUSSION
Although particularly radiosensitive organs are conventionally protected with a lead shield during radiography, lead causes metal artifacts and decreases image quality. However, B-shields and conventional lead shields react differently to x-rays. Lead shields completely absorb radiation, whereas B-shields decrease the amount of soft radiation and thus alter only the x-ray energy distribution. Therefore, B-shields should be useful for protecting radiosensitive organs, such as the eye lens, because B-shields generate fewer metal artifacts than lead shields.
The present study evaluated whether B-shields could reduce the radiation dose and maintain the accuracy of SPECT images. We found that B-shields reduced the radiation dose to the eye lens by about 60% and that radioactivity concentrations with and without the B-shield were equivalent. These results indicate that B-shields could confer radioprotection, especially for pediatric patients and patients with extant eye diseases who undergo brain SPECT/CT imaging.
The radiation dose was reduced by about 60% at the top of the CT dose index phantom at each tube current. For comparison, Ciarmatori et al. (16) reported that B-shielding can reduce the entrance surface dose by 21%–29% during head CT examinations and Wang et al. (17) reported that a B-shield and tube current modulation reduced the radiation dose to the eye lens by 26.4%. Our results are essentially consistent with these previous findings, but the dose reduction was significantly greater during CT imaging in the present study. The reason for this difference is the difference in the lead equivalent of the B-shield. The lead equivalent in the current and previous studies was 0.15 and 0.06 mm, respectively. Hopper et al. (13) showed that the CT dose decreased when the shield thickness increased. Therefore, we think that optimization of the lead equivalent is necessary for more effective dose reduction. Our results indicate that the CT dose per scan is tiny compared with the International Commission on Radiological Protection–recommended dose (<2.0 mGy). However, for radiation examinations, every effort should be made to reduce radiation doses without compromising image quality according the “as low as reasonably achievable” concept. The use of B-shielding is considered to improve the benefits of brain SPECT/CT for patients.
The mean CT number increased with the B-shield because of beam-hardening artifacts, but this increase was limited to a superficial region. This result agrees with those of previous studies. Hopper et al. (13) reported that the increased CT number caused by a protection shield did not project into the brain. Hein et al. (12) found that use of an eye shield did not impair diagnostic information in a study of 127 patients. In addition, Hohl et al. (18) showed that a spacer between the surface and shield can reduce the deleterious effects on image quality caused by beam-hardening artifacts.
Linear attenuation coefficients did not significantly differ between the shielded and nonshielded conditions at the middle and bottom of the phantom. The linear attenuation coefficient was estimated on the basis of the CT number. Because the CT number changed only slightly, we considered that the accuracy of the attenuation coefficient was maintained when using the B-shield. We also found that the coefficient of variation was similar with and without the B-shield. These findings indicate that B-shields can be used during brain SPECT/CT image acquisition.
The relative amounts of radioactivity in the 3D brain phantom with and without the B-shield did not differ significantly. The maximum difference between measurements with and without B-shielding was 5.1%, and this was found only in the thalamus. For comparison, Akamatsu et al. (19) reported that the regional radioactivity differed by 1.8%–11.5% among several reconstruction methods. Ishii et al. (20) showed that the relative SPECT counts obtained by Chang’s attenuation correction increased by 5.0% and decreased by 4.6% in the frontal and cerebellar regions, respectively, compared with CT attenuation correction. The results support the notion that the use of a B-shield can benefit patients by decreasing the radiation exposure risk to their corneas. Although B-shields have several disadvantages, we recommend their application from the perspective of radiation protection during brain SPECT/CT.
This study has some limitations. One is the simple protocol using several geometric phantoms. In addition, the region of white matter in the 3D brain phantom did not contain the radioactive solution. Further study is required to evaluate clinical brain SPECT/CT with B-shields. Another limitation is that we did not compare the effect of dose reduction using B-shields with dose reduction using other techniques, such as organ-based tube current modulation and CT iterative reconstruction (21,22). These techniques can also potentially reduce the radiation dose. The effects of the B-shield combined with other methods of reducing the radiation dose should be evaluated.
CONCLUSION
We evaluated the effects of a B-shield on brain SPECT/CT images in a phantom study. The shield reduced the dose of radiation delivered to the eye lens by about 60%. Although the B-shield increased image artifacts at the surface, the concentration of radioactivity was acceptable. Our results suggest that the B-shield can help protect patients undergoing assessment by brain SPECT/CT, especially pediatric patients and patients with eye disease.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online May 4, 2017.
REFERENCES
- Received for publication March 11, 2017.
- Accepted for publication April 26, 2017.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.