


Abstract
Planar perfusion scintigraphy with 99mTc-labeled macroaggregated albumin is often used for pretherapy quantification of regional lung perfusion in lung cancer patients, particularly those with poor respiratory function. However, subdividing lung parenchyma into rectangular regions of interest, as done on planar images, is a poor reflection of true lobar anatomy. New tridimensional methods using SPECT and SPECT/CT have been introduced, including semiautomatic lung segmentation software. The present study evaluated inter- and intraobserver agreement on quantification using SPECT/CT software and compared the results for regional lung contribution obtained with SPECT/CT and planar scintigraphy. Methods: Thirty lung cancer patients underwent ventilation–perfusion scintigraphy with 99mTc-macroaggregated albumin and 99mTc-Technegas. The regional lung contribution to perfusion and ventilation was measured on both planar scintigraphy and SPECT/CT using semiautomatic lung segmentation software by 2 observers. Interobserver and intraobserver agreement for the SPECT/CT software was assessed using the intraclass correlation coefficient, Bland–Altman plots, and absolute differences in measurements. Measurements from planar and tridimensional methods were compared using the paired-sample t test and mean absolute differences. Results: Intraclass correlation coefficients were in the excellent range (above 0.9) for both interobserver and intraobserver agreement using the SPECT/CT software. Bland–Altman analyses showed very narrow limits of agreement. Absolute differences were below 2.0% in 96% of both interobserver and intraobserver measurements. There was a statistically significant difference between planar and SPECT/CT methods (P < 0.001) for quantification of perfusion and ventilation for all right lung lobes, with a maximal mean absolute difference of 20.7% for the right middle lobe. There was no statistically significant difference in quantification of perfusion and ventilation for the left lung lobes using either method; however, absolute differences reached 12.0%. The total right and left lung contributions were similar for the two methods, with a mean difference of 1.2% for perfusion and 2.0% for ventilation. Conclusion: Quantification of regional lung perfusion and ventilation using SPECT/CT-based lung segmentation software is highly reproducible. This tridimensional method yields statistically significant differences in measurements for right lung lobes when compared with planar scintigraphy. We recommend that SPECT/CT-based quantification be used for all lung cancer patients undergoing pretherapy evaluation of regional lung function.
Quantification of regional lung perfusion with 99mTc-labeled macroaggregated albumin is commonly used to evaluate pulmonary function in patients with lung cancer before volume reduction surgery (1,2) or radiotherapy (3). Quantification allows estimation of the impact of treatment on forced expiratory volume in 1 s in those with borderline pretherapy lung function (4,5). The current most widely used method for quantification of regional lung function uses planar perfusion scintigraphy. In that method, the lung parenchyma is subdivided into 6 equal-sized rectangular regions of interest (ROIs). The relative percentage of counts in each lung region is calculated from the geometric mean on anterior and posterior views, thus approximating the lobar contribution. However, rectangular ROIs are a poor representation of true lobar anatomy (5).
With the advent of hybrid imaging, new methods of tridimensional lung segmentation using SPECT and SPECT/CT have been introduced, offering anatomically based quantification of the lobar contribution for perfusion studies (6–8) or combined ventilation–perfusion studies (9,10). Recently, a semiautomatic lung segmentation software program has been developed for SPECT/CT (Hermes Hybrid 3D Lung Lobe Quantification; Hermes Medical Solutions). However, the reproducibility of measurements obtained with this software in a clinical setting has not been studied, nor has the feasibility of SPECT/CT quantification in a group of patients with a high prevalence of underlying lung disease, such as nonsurgical candidates undergoing radiotherapy.
In the present study, we evaluated the feasibility and the inter- and intraobserver agreement of lung quantification using this software, and we compared the regional lung contribution results with those of traditional planar methods for ventilation–perfusion studies.
MATERIALS AND METHODS
We included 30 consecutive lung cancer patients (14 women and 16 men with a mean age 68.2 y; range, 52–80 y) referred to our Nuclear Medicine Department for preradiotherapy evaluation of lung function from April 2015 to June 2016. The institutional review board approved this study, and all subjects signed an informed consent form. The patient characteristics are detailed in Table 1.
Patient Characteristics
Ventilation and perfusion scintigraphy were performed on the same day with inhalation of 99mTc-Technegas (Cyclomedica; mean dose, 577 MBq placed in a crucible) and intravenous injection of 99mTc-macroaggregated albumin (mean dose, 292 MBq). The ratio of perfusion counting rate to ventilation counting rate was higher than 4 in all patients. All studies were performed on a dedicated SPECT/CT camera (Discovery NM/CT 670; GE Healthcare). A SPECT-only acquisition was performed for the ventilation study, whereas a SPECT/CT acquisition with attenuation correction was performed for the perfusion study. Planar anterior and posterior acquisitions were obtained for both the ventilation and the perfusion studies. The SPECT acquisition parameters included a 20% energy window centered at 140 keV, a 128 × 128 matrix, a total acquisition of 60 frames over 360°, with 28 s per projection for the ventilation acquisition and 17 s for the perfusion acquisition. Acquisitions were performed using a low-energy, high-resolution parallel-hole collimator and a zoom factor of 1.28. SPECT reconstructions were performed using iterative tridimensional ordered-subsets expectation maximization (HRECON, version 1.1C; Hermes Medical Solutions) with 3 iterations, 6 subsets, and a tridimensional gaussian filter (1.25 cm in full width at half maximum). A helical CT acquisition was obtained during free breathing immediately before the perfusion SPECT acquisition. The CT parameters included a voltage of 120 kV, a current of 150 mA, a 0.5-s rotation time, a pitch of 1.375, 16 × 0.625 mm collimation, and reconstruction at a 1.25-mm slice thickness using filtered backprojection and a soft-tissue filter. There was no intravenous contrast injection. The estimated effective doses were 3 mSv for SPECT acquisitions and 2 mSv for a single CT acquisition. SPECT and SPECT/CT images were reviewed for adequate coregistration. Planar ventilation images were visually assessed for central deposition of Technegas.
For planar scintigraphy, quantification was performed using Hermes Hybrid Viewer lung quantification software (Hermes Medical Solutions), which subdivides each lung into 3 rectangular ROIs and computes the relative contribution (percentage) of each ROI from the geometric mean of counts on anterior and posterior views (Fig. 1A). For SPECT and SPECT/CT, tridimensional quantification was performed using Hermes Lung Lobe Quantification with Hybrid 3D. The workflow in this software consists of, first, automatic CT-based lung volume detection through a region-growing algorithm; second, semiautomatic delimitation of lung fissures (the user defines 6 points along each lung fissure on multiple reconstructed CT slices in the sagittal plane); third, software computation of 5 volumes of interest, one for each lobe (right upper, right middle, right lower, left upper, and left lower).

(A) Quantification of perfusion using planar method. (B and C) Quantification of perfusion with semiautomatic SPECT/CT-based lung segmentation software (CT-based volumes of interest [C] with tridimensional rendering [B]).
Ventilation and perfusion studies are coregistered to CT with a mutual-information algorithm and an identical frame of reference, respectively. Volumes of interest are applied to coregistered ventilation–perfusion SPECT data, and the relative contribution (percentage) of each lobe is computed for both ventilation and perfusion. A tridimensional rendering of CT-based volumes of interest is displayed along with the quantification results (Figs. 1B and 1C).
SPECT/CT-based segmentation was performed by observer 1 for both ventilation and perfusion studies for all patients and by observer 2 once for perfusion. Observer 1 repeated the measurements at least 1 wk later to minimize recall bias. The observers were masked to any previous measurement.
Interobserver and intraobserver agreement on the tridimensional quantification of perfusion and ventilation, respectively, was assessed using 2-way random, absolute-agreement, single-measures intraclass correlation coefficients (11).
For both the interobserver and the intraobserver analyses, absolute differences between measurements were calculated, as well as the mean absolute difference for each lobe. Bland–Altman plots were also done for interobserver analysis (12).
The quantification results for the left middle third on planar scintigraphy were redistributed equally between the left upper and left lower thirds to allow comparison with the left upper and left lower lobes, respectively, for the tridimensional method (Fig. 2). The quantification results for the right lung ROIs on planar scintigraphy were compared directly (i.e., upper third with right upper lobe, middle third with right middle lobe, and lower third with right lower lobe). Comparison of results for total right and total left lungs, as well as lobar quantification obtained by planar and SPECT/CT studies (using results from observer 1) was performed using paired-sample t tests for both ventilation and perfusion. Subgroup analysis was performed for patients with and without central deposition of Technegas on the planar ventilation study. P values of less than 0.05 were considered statistically significant. Mean absolute differences for the results of both methods were also calculated. Statistical analyses were performed with SPSS (version 24.0.0.0; IBM).

Schematic representation for comparison of quantification measurements on planar scintigraphy and SPECT/CT.
RESULTS
Semiautomatic segmentation using the SPECT/CT-based software was feasible in 29 of the 30 patients, taking on average 5–10 min per patient. We excluded one patient because automatic detection of the lung contour failed.
Mean measurements obtained by planar imaging and SPECT/CT, mean absolute differences between the two methods, and P values from paired-sample t tests comparing the two methods are shown in Tables 2 and 3 for perfusion and ventilation, respectively.
Comparison of Quantification Values on Perfusion Studies
Comparison of Quantification Values on Ventilation Studies
The right/left lung differentials obtained by the planar and tridimensional methods did not significantly differ for the perfusion studies (Table 2) but did for the ventilation studies (Table 3). However, no statistically significant difference was found when only the subgroup of patients without central deposition of Technegas was considered (n = 18) (Table 3).
For lobar quantification of both perfusion and ventilation, there was a statistically significant difference in values obtained by the planar and tridimensional methods for the right upper, right middle, and right lower lobes, whereas there was no statistically significant difference for the left upper and left lower lobes, as shown in Tables 2 and 3. For the left lung lobes, one third of patients had an absolute difference of more than 5.0% in quantification measurements between the two methods.
When considering only the lobe of clinical interest for each patient (e.g., left upper lobe quantification for a patient with left upper lobe tumor), there was a statistically significant difference in measurements obtained by SPECT/CT and planar methods (P = 0.04), with a mean absolute difference of 7.1% for perfusion (minimum, 0.2%; maximum, 22.8%). For both perfusion and ventilation, absolute differences between total right and left lung contribution measured with planar and tridimensional methods were very small. However, absolute differences were much higher for individual lobar values, especially for right lung lobes, with a maximal absolute difference for the right middle lobe of 36.0% for perfusion and 29.7% for ventilation (Tables 2 and 3).
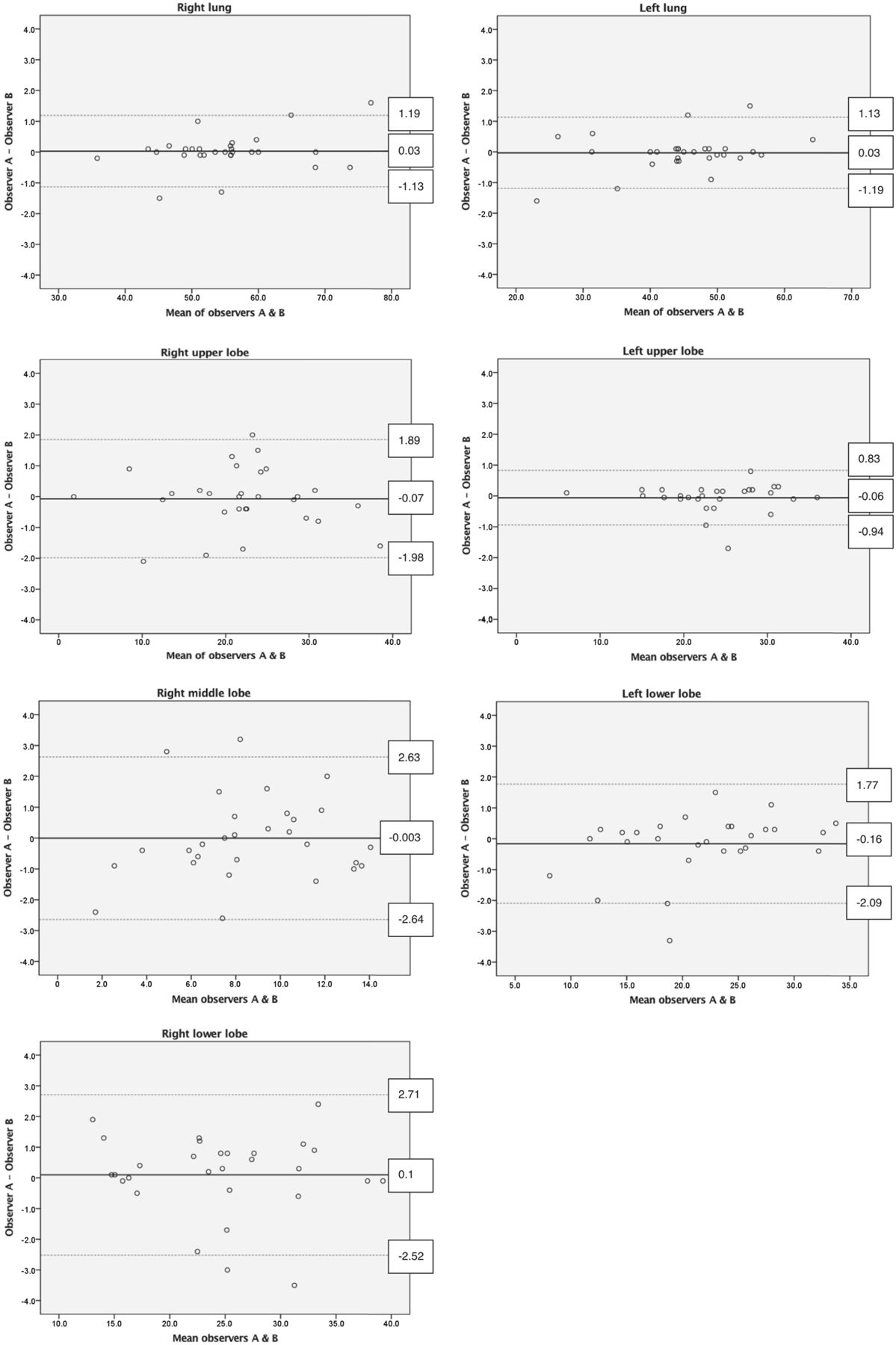
Comparison of interobserver measurements revealed very small mean absolute differences (0.3%–1.0%), as well as intraclass correlation coefficients in the excellent range (Table 4). Bland–Altman plots showed narrow limits of agreement for all measurements (Fig. 3).
Interobserver Measurements for Quantification on SPECT/CT Perfusion Studies

Bland–Altman plots for interobserver measurements of total lung and lobar perfusion using SPECT/CT.
Intraclass correlation coefficients for intraobserver measurements were also excellent (>0.9) for all lobes and for total right and left lungs, with very small mean absolute differences between repeated measurements (0.3%–1.3%) (Table 5).
Intraobserver Measurements for Quantification on SPECT/CT Ventilation Studies
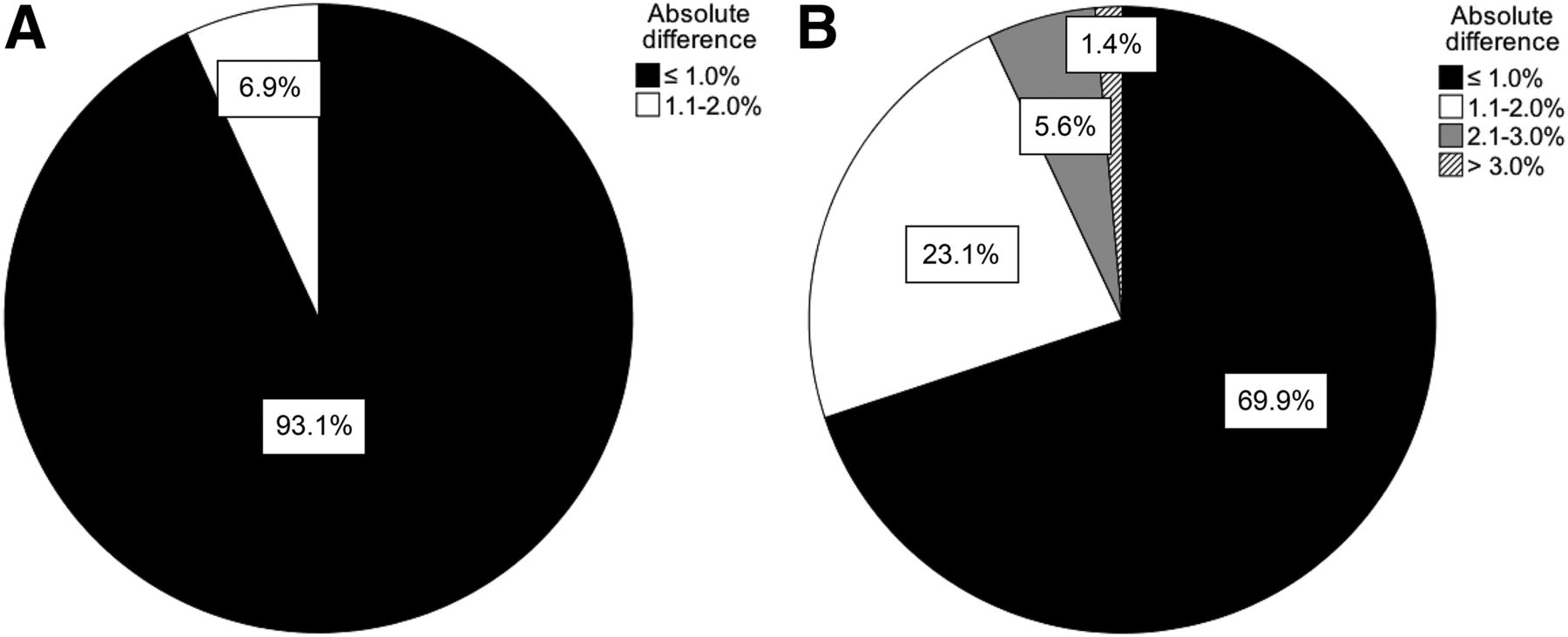
Absolute differences of less than 2.0% were found in 96% of repeated interobserver and intraobserver measurements (Figs. 4 and 5).

Absolute differences in interobserver measurements of total lung (A) and lobar (B) contribution using SPECT/CT.
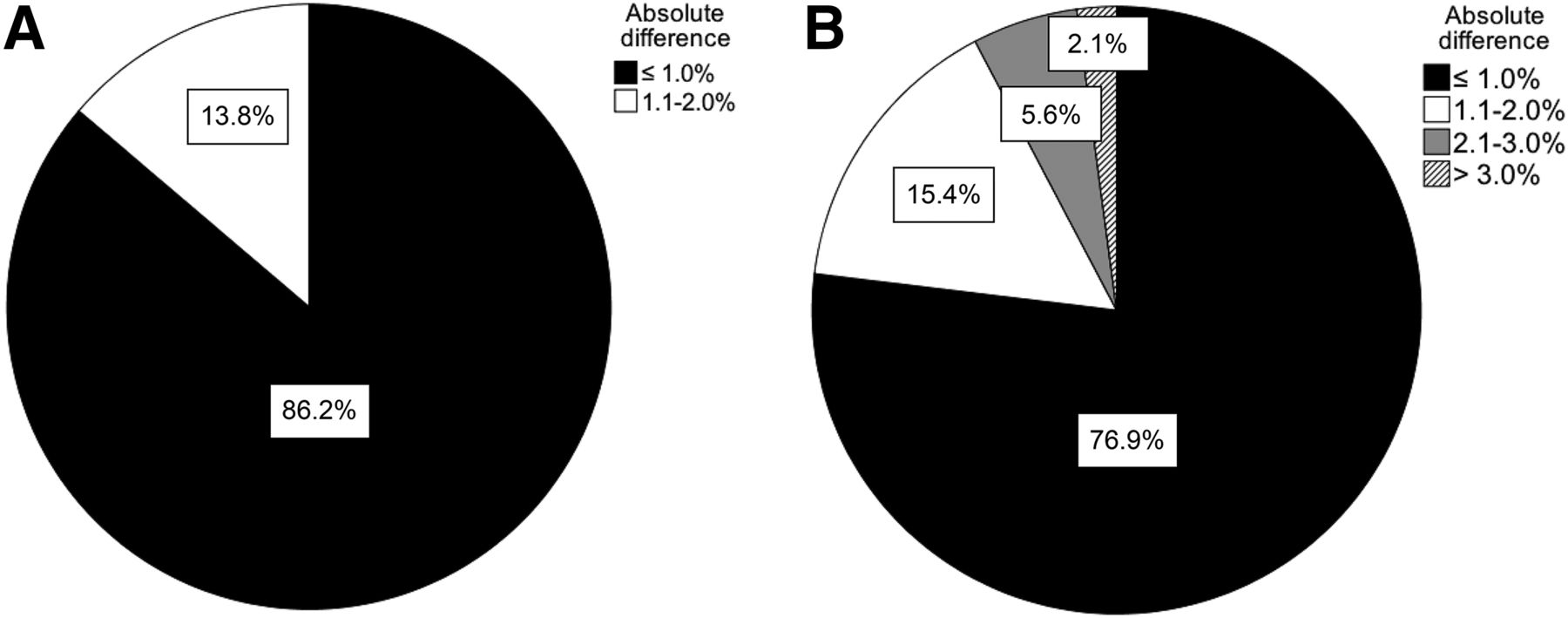
Absolute differences in intraobserver measurements of total lung (A) and lobar (B) contribution using SPECT/CT.
DISCUSSION
Quantification of lobar perfusion and ventilation using SPECT and SPECT/CT with a semiautomatic segmentation algorithm has excellent inter- and intraobserver agreement. This method yields statistically and clinically significant differences when compared with segmentation with planar scintigraphy for the right lung lobes, with an absolute difference of up to 36.0%. Although differences in values for the left lung lobes were not statistically significant, they can be considered clinically significant, with absolute differences of greater than 5.0% in one third of patients and maximal absolute differences of 12.0%. We can hypothesize that such differences could alter the clinical management of certain patients.
In practice, the left lung is often subdivided into 3 ROIs when planar images are used for quantification. For the purpose of this study, the contribution of the left middle ROI was redistributed equally to the left upper and left lower thirds. This redistribution more closely approximates true left lung anatomy, with more or less equal-sized upper and lower lobes. This may explain the lack of statistically significant differences when we compare quantification results for the left lung lobes from planar and SPECT/CT segmentation techniques.
Delineation of volumes of interest from the CT acquisition more accurately represents individual patient anatomy. Therefore, ventilation–perfusion quantification obtained from those volumes of interest is more likely to represent the true lobar contribution to perfusion and ventilation than the arbitrarily defined rectangular subdivisions drawn on planar scintigraphy. Furthermore, on planar images, extraneous activity may not be easily excluded from the quantification. Examples include tracheobronchial deposition of 99mTc-Technegas, thyroid and gastric activity from free pertechnetate, and residual vascular activity on 99mTc-macroaggregated albumin studies. Additionally, in some cases, the right and left lungs cannot be easily separated with the preset rectangular ROIs (Fig. 6). Tridimensional segmentation with SPECT/CT overcomes these limitations by considering only the activity corresponding to true lung parenchyma. For these reasons, we believe that planar-based quantification should be abandoned in favor of SPECT/CT or SPECT in centers without access to hybrid cameras.
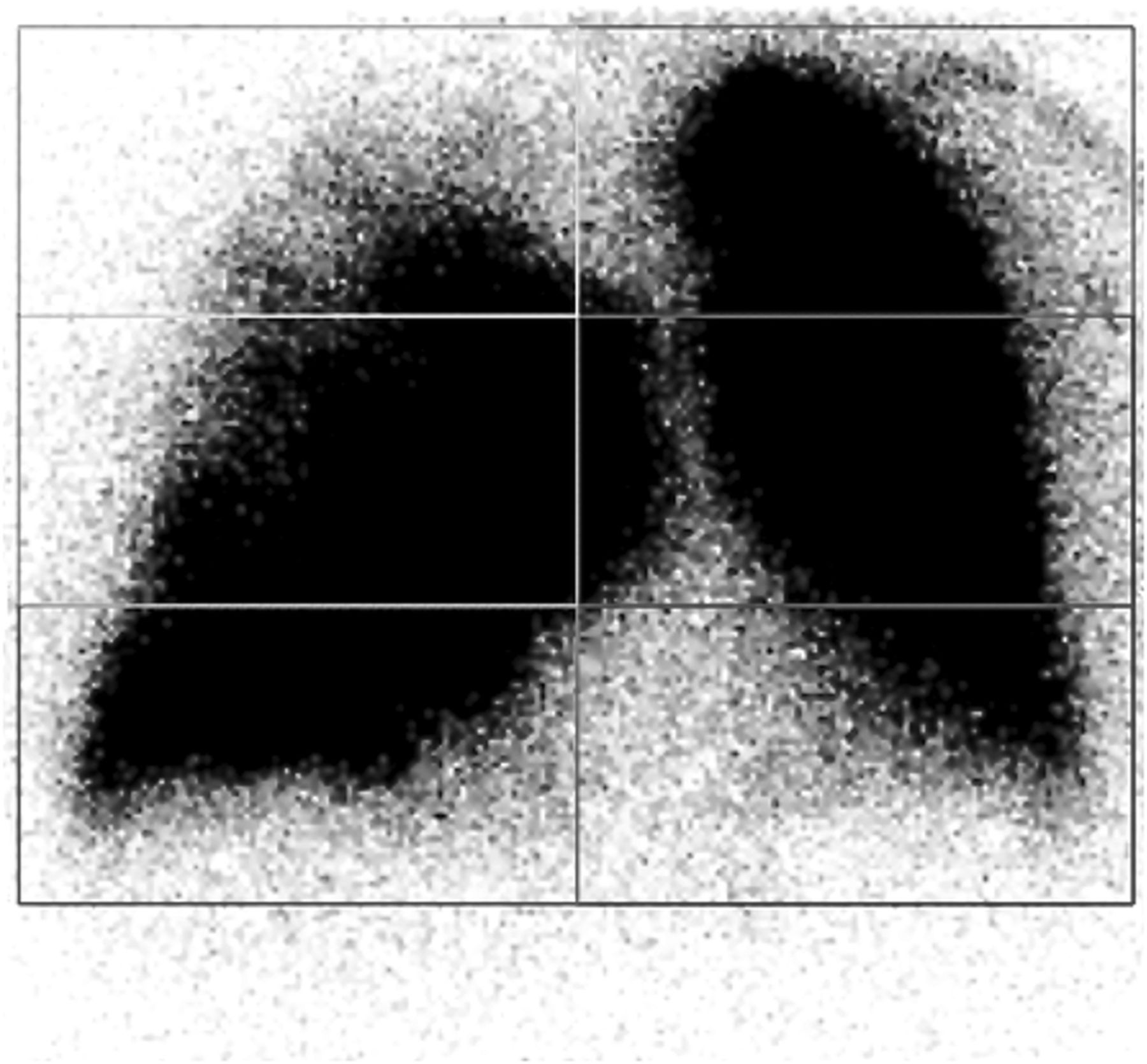
Example of inadequate segmentation on planar scintigraphy due to right lung parenchyma overlying midline. There is also prominent vascular activity, partly included in left upper and left middle lung regions (anterior view is shown; image contrast is increased).
Several studies have investigated manual tridimensional lung segmentation techniques using SPECT or SPECT/CT for both preoperative (6–8,10,13–15) and preradiotherapy (16,17) patients. Only a few studies investigated semiautomatic algorithms for total lung and lobar segmentation using SPECT/CT in preoperative patients (9,18). No studies had previously compared results to those obtained with planar scintigraphy, or evaluated interobserver and intraobserver agreement on patient studies. In our study, we demonstrated the excellent reproducibility of the semiautomatic segmentation technique in a population with a high prevalence (63%) of underlying lung disease, which makes visualization of lung anatomy more challenging. We can hypothesize that we would obtain even more reproducible results in patients with unaltered lung parenchyma, such as most preoperative patients.
Quantification based on perfusion scintigraphy only, as opposed to combined ventilation–perfusion scintigraphy, has been used by some groups (7,8,18), with few studies having investigated the role of ventilation scintigraphy on prediction of posttreatment forced expiratory volume in 1 s (9,10). However, at our institution, combined ventilation–perfusion scintigraphy is routinely performed to exclude underlying thromboembolic disease in cancer patients referred for quantitative perfusion lung scintigraphy. In our cohort, one patient had an incidental finding of pulmonary emboli.
Multiple non–nuclear medicine imaging techniques have been described for evaluation of lung perfusion, including MRI, CT pulmonary angiography, and double-energy CT with parenchymal iodine mapping (19). Although these techniques are accurate, widespread use for perfusion quantification has been restricted by limited accessibility, as well as contraindications and the inherent risk of iodine contrast injection. These CT-based techniques also have substantially higher radiation doses to patients than do nuclear medicine techniques.
The semiautomatic lung segmentation software used in this study allows simple and rapid quantification of both perfusion and ventilation studies in a single streamed workflow, taking on average 5–10 min per patient. Some limitations of this technique include occasional difficulty in visualizing lung fissures on free-breathing CT, although this occurred in a minority of patients and did not significantly influence inter- or intraobserver agreement, as shown in our results. In our study, CT was acquired during free breathing to match perfusion acquisition. In patients with suboptimal fissure visualization, it would have been possible to use a previous diagnostic CT scan and coregister it for lung segmentation; however, this was not done because we wanted to ensure uniformity of the method across patients and avoid differences in lung volumes between CT and SPECT acquisitions. Another limitation of the software is that the automatic lung contour detection is sometimes more difficult when lung density is highly heterogeneous, such as in the presence of extensive bullae mixed with areas of fibrosis. As previously mentioned, one patient had to be excluded because the software failed to detect the lung contours. This failure was found to be due to an endobronchial density that prevented the region-growing algorithm from functioning correctly. A disadvantage of SPECT/CT-based methods is dependence on tomographic acquisitions and hybrid cameras, which can increase imaging cost.
Limitations of this study also include a small number of patients, who were all nonsurgical candidates with a high prevalence of underlying lung disease. He et al. (9) have described the accurate prediction of postlobectomy lung function in 305 patients using a semiautomatic lung segmentation algorithm. Further work is needed to evaluate whether results obtained with the tridimensional technique predict the posttreatment forced expiratory volume in 1 s more accurately than traditional planar scintigraphy in patients undergoing radiotherapy. It would also be interesting to take into account the actual radiation treatment fields in quantification of regional parenchymal perfusion and prediction of posttherapy forced expiratory volume in 1 s.
CONCLUSION
Tridimensional lung lobar quantification can easily be performed using SPECT/CT acquisitions and semiautomatic segmentation software for both perfusion and ventilation studies. This segmentation technique demonstrates excellent interobserver and intraobserver agreement. Results obtained with this method differ significantly from those obtained with planar scintigraphy, especially for the right lung lobes. We recommend that SPECT/CT-based quantification be used for all lung cancer patients undergoing pretherapy evaluation of regional lung function. Further studies are needed to evaluate prediction of postradiotherapy forced expiratory volume in 1 s with this technique and whether quantification of perfusion or ventilation yields the most accurate results.
DISCLOSURE
The semiautomatic lung segmentation software (Hermes Hybrid 3D Lung Lobe Quantification) was provided by Hermes Medical Solutions with a prerelease agreement. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Apr. 13, 2017.
REFERENCES
- Received for publication January 31, 2017.
- Accepted for publication April 11, 2017.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Three-dimensional (3D) lung segmentation for diagnosis of COVID-19 and the communication of disease impact to the public
- Head-to-Head Prospective Comparison of Quantitative Lung Scintigraphy and Segment Counting in Predicting Pulmonary Function in Lung Cancer Patients Undergoing Video-Assisted Thoracoscopic Lobectomy