


Abstract
Mandibular condylar hyperplasia (CH) is a complex developmental deformity resulting in asymmetries of the hyperplastic condyle. Bone scan SPECT is a sensitive and accurate method of detecting the growth activity of this disorder. This method can be used to quantitate the radionuclide uptake differences between the left and right condyles. Uptake differences of 10% or more between the left and right condyles, with increased uptake ipsilateral to the CH, are considered to be evidence of active growing CH. Quantitative assessment of CH is important to select an appropriate treatment course. Degenerative arthropathies of the temporomandibular joints may result in altered uptake, but this is mostly associated with the side contralateral to the CH. The CT portion of SPECT/CT is useful to assess the condylar dimensions and underlying bony changes.
- bone
- SPECT
- SPECT/CT
- bone scintigraphy
- condylar hyperplasia
- mandibular condyle hyperplasia
- temporomandibular disorders
Condylar hyperplasia (CH) is a complex developmental deformity leading to asymmetries of the hyperplastic condyle. It causes facial asymmetry and malocclusion and can be associated with pain and dysfunction. Accurate assessment of condylar growth and establishment of disease activity provide guidance for treatment. Bone scan SPECT has demonstrated a performance in this application superior to planar imaging through the accurate and quantifiable assessment of mandibular condylar growth (1–3). The CT portion of SPECT/CT provides detailed anatomic information associated with growth activity.
CASE REPORT
A 40-y-old woman (who gave consent for study inclusion) presented with a 20-y history of pain in the bilateral TMJs (temporomandibular joints), with pain worse in severity on the left side. Bone scintigraphy was ordered to evaluate growth activity in the left CH.
A limited examination of the TMJs consisted of radionuclide angiography and immediate postinjection images with 3-h delayed planar image collection after intravenous administration of 740 MBq (20 mCi) of 99mTc-methylene diphosphonate (MDP). Subsequent SPECT/CT was performed using a GE-640 SPECT/CT camera (GE Healthcare).
DISCUSSION
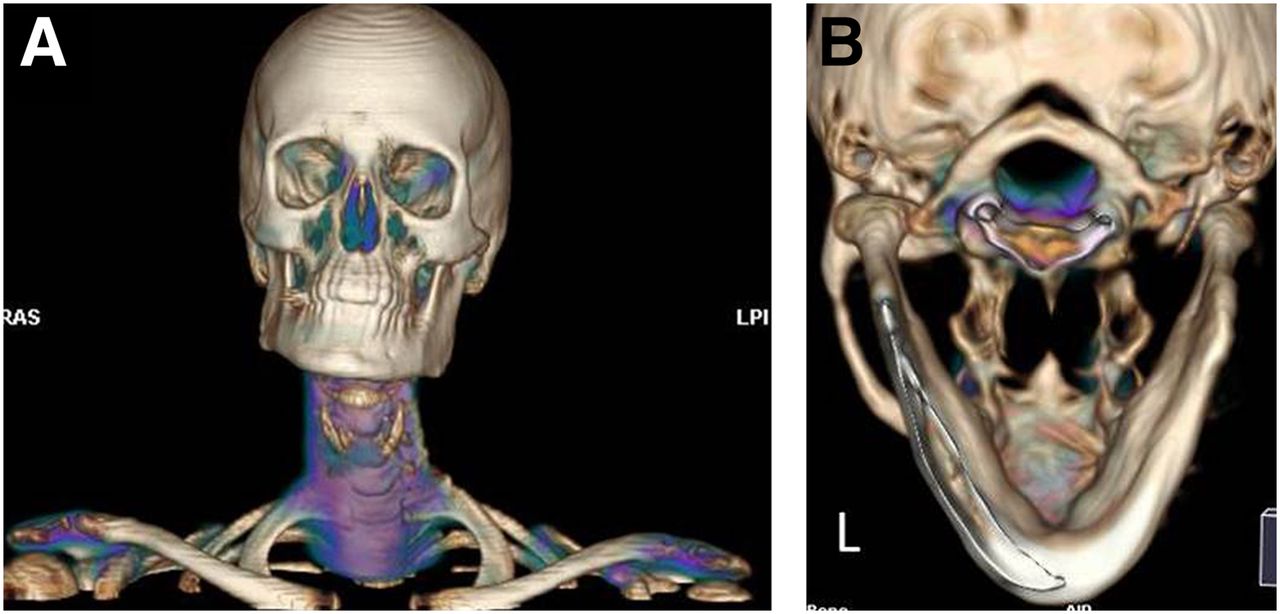
The CT 3-dimensional volume reconstruction image showed the patient’s chin tilted to the right (Fig. 1), consistent with the patient’s facial asymmetry on physical exam.
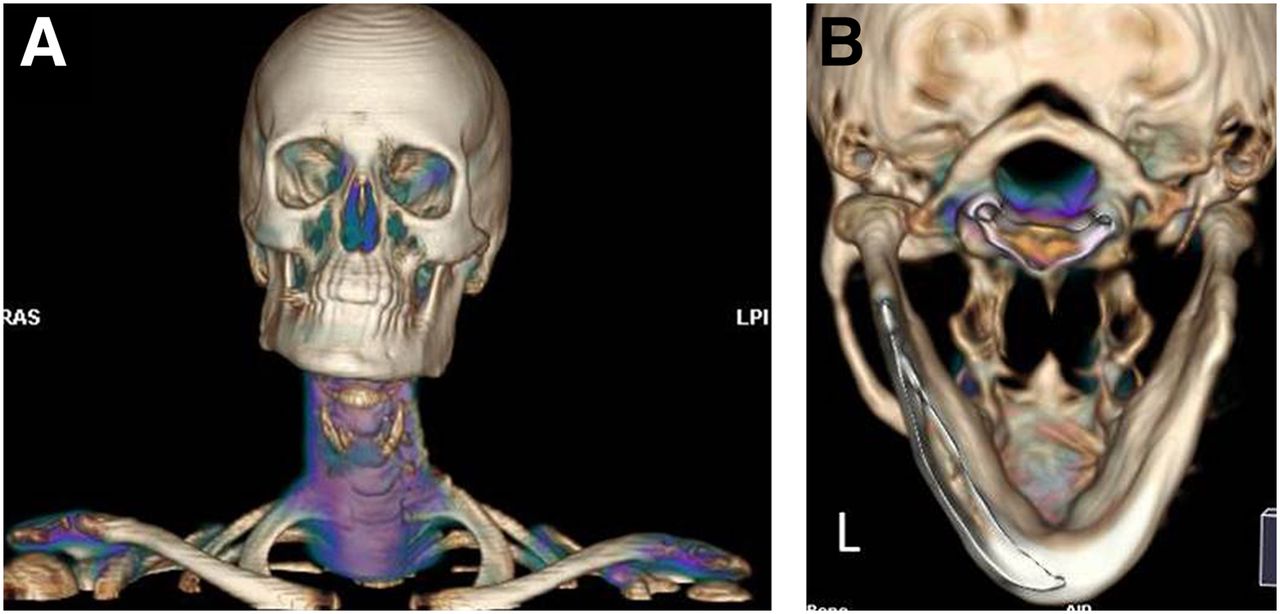
CT 3-dimensional volume reconstruction image shows asymmetry of mandible. (A) Right mandibular ramus is shorter vertically than left mandibular ramus. Corresponding posterior volume reconstruction views (B) further demonstrate larger left condyle. These findings are consistent with patient’s facial asymmetry as found on physical exam.
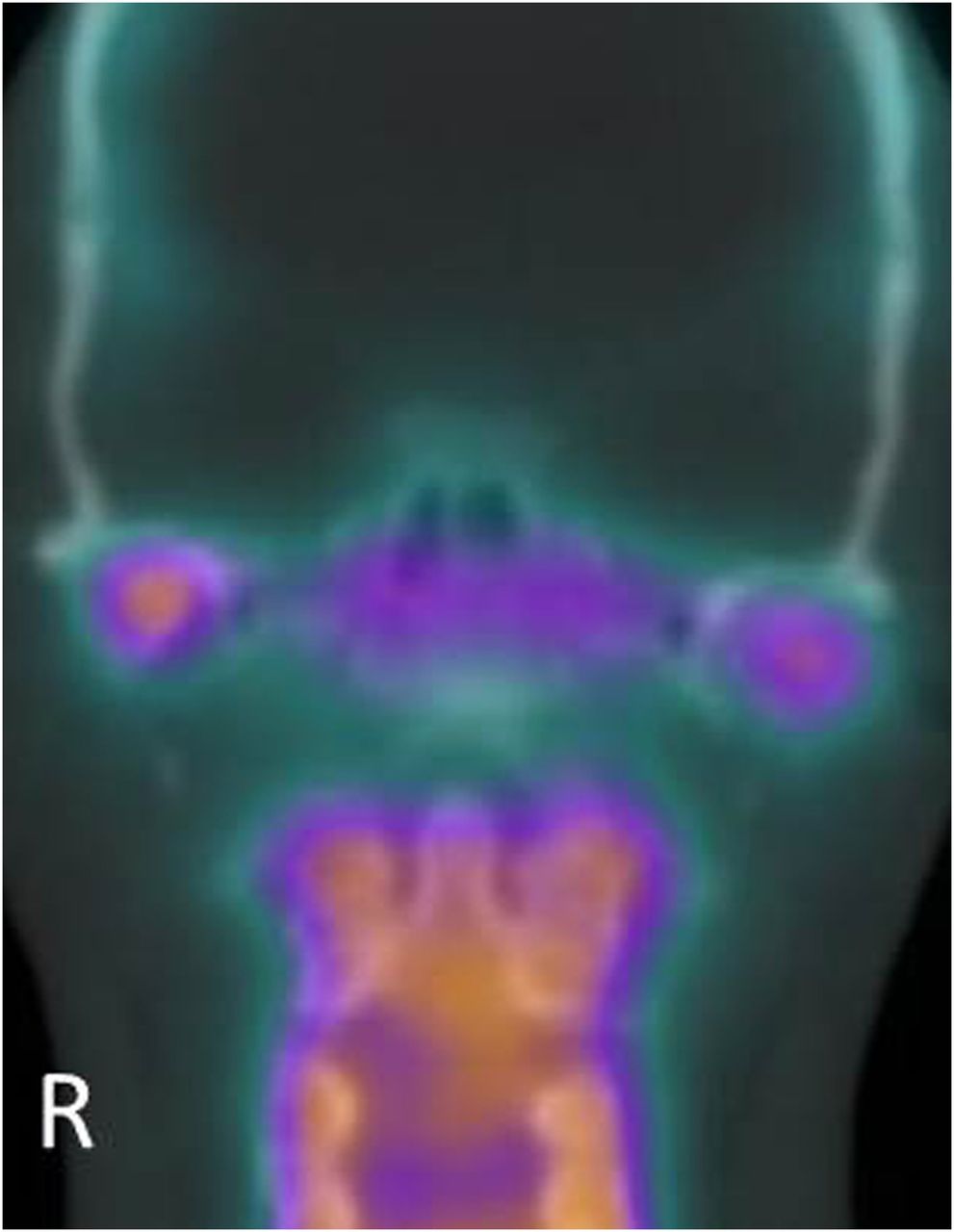
The SPECT results showed increased 99mTc-MDP uptake in the mandibular condyles compared with that of the clivus. Additionally, asymmetric MDP uptake was observed, with the right increased over the left side (Figs. 2 and 3). Calculated uptake was 55% on the right (right condyle counts divided by the sum of right and left condyle counts) and 45% on the left. The 10% difference observed with increased uptake on the side contralateral to the CH indicated inactive growth. This asymmetric 99mTc-MDP uptake was not observed in the planar images (not shown).
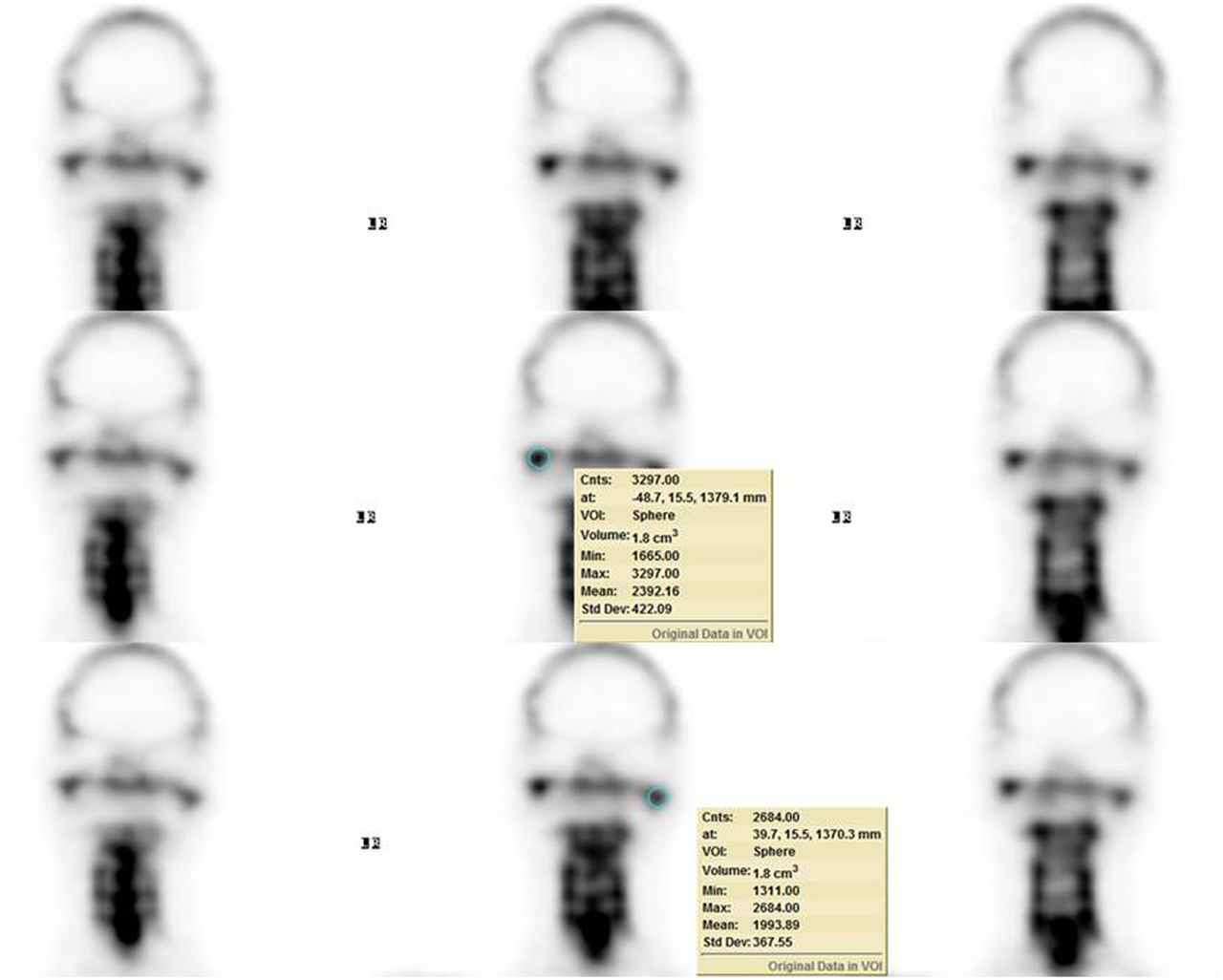
Same serial coronal SPECT images are displayed with measured counts shown on rows 2 and 3. Volumetric 3-dimensional quantification software (GE Healthcare) was used to indicate region of interest on each condyle. Total counts of right condyle, 3,297.00 counts/1.8 cm3, and of left condyle, 2,684.00 counts/1.8 cm3, are shown on rows 2 and 3, respectively. There is increased 99mTc-MDP uptake in mandibular condyles compared with that of clivus. SPECT scan was obtained using the optimal 640 hybrid camera (GE Healthcare) with dual heads and a pair of low-energy, high-resolution collimators. SPECT data were acquired from 120 projections over 360° at 30 s per projection on a matrix of 128 × 128. Three-dimensional SPECT images were reconstructed on Xeleris workstation with Volumetrix MI Evolution software (GE Healthcare) for bone using following parameters: 2 iterations, 10 subsets, Butterworth filter with cutoff frequency at 0.48, and power at 10. Slice thickness was 4.42 mm. Cnts = counts; Max = maximum; Min = minimum; Std Dev = standard deviation; VOI = volume of interest.
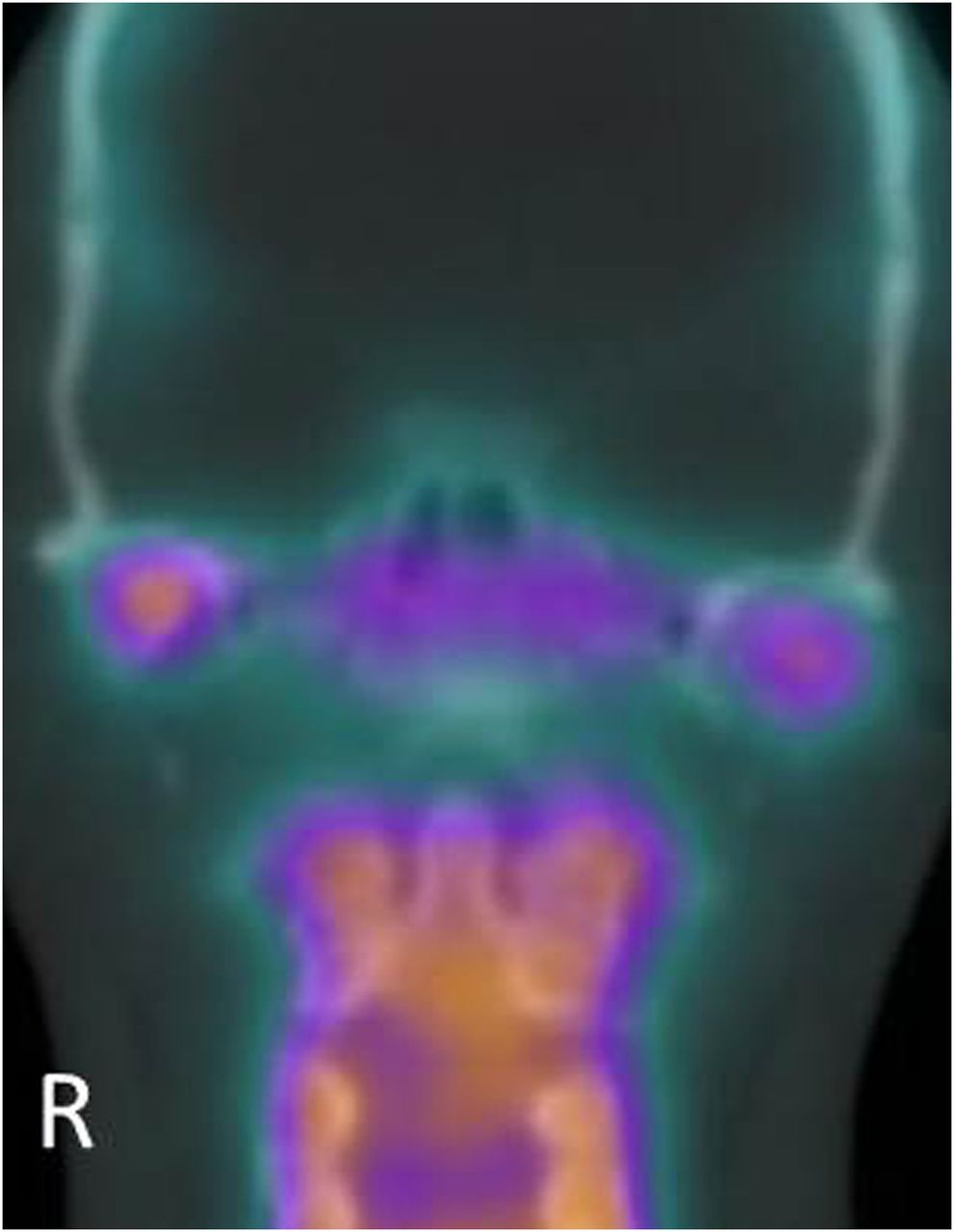
Coronal fusion image of SPECT and CT shows asymmetric uptake in bilateral mandibular condyles with increased uptake on right side compared with left side.
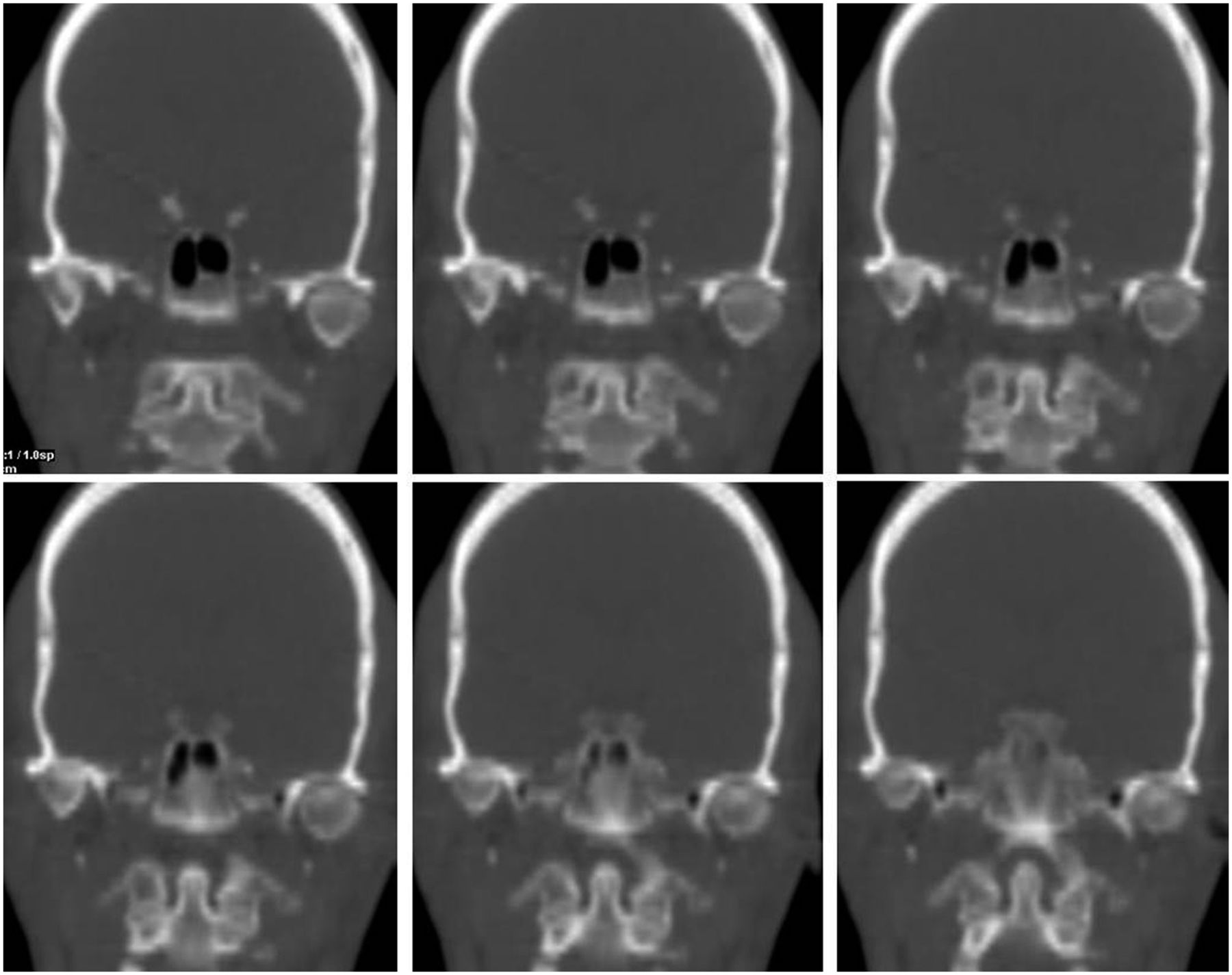
The low-dose CT showed that the left mandibular condyle was larger (21.4 × 22.5 × 12.2 mm) than the right mandibular condyle (17.8 × 16.1 × 9.8 mm) in the axial, coronal, and sagittal reconstruction images, respectively (Fig. 4). The TMJ spaces were narrowed with sclerosis (particularly on the right side) (Fig. 5). These findings led to 2 conclusions: the left mandibular condyle was larger with less 99mTc-MDP uptake, indicating an inactive left mandibular CH; and the TMJs, narrowed with sclerosis, had increased 99mTc-MDP uptake, indicating degenerative changes, with the right side being more advanced.
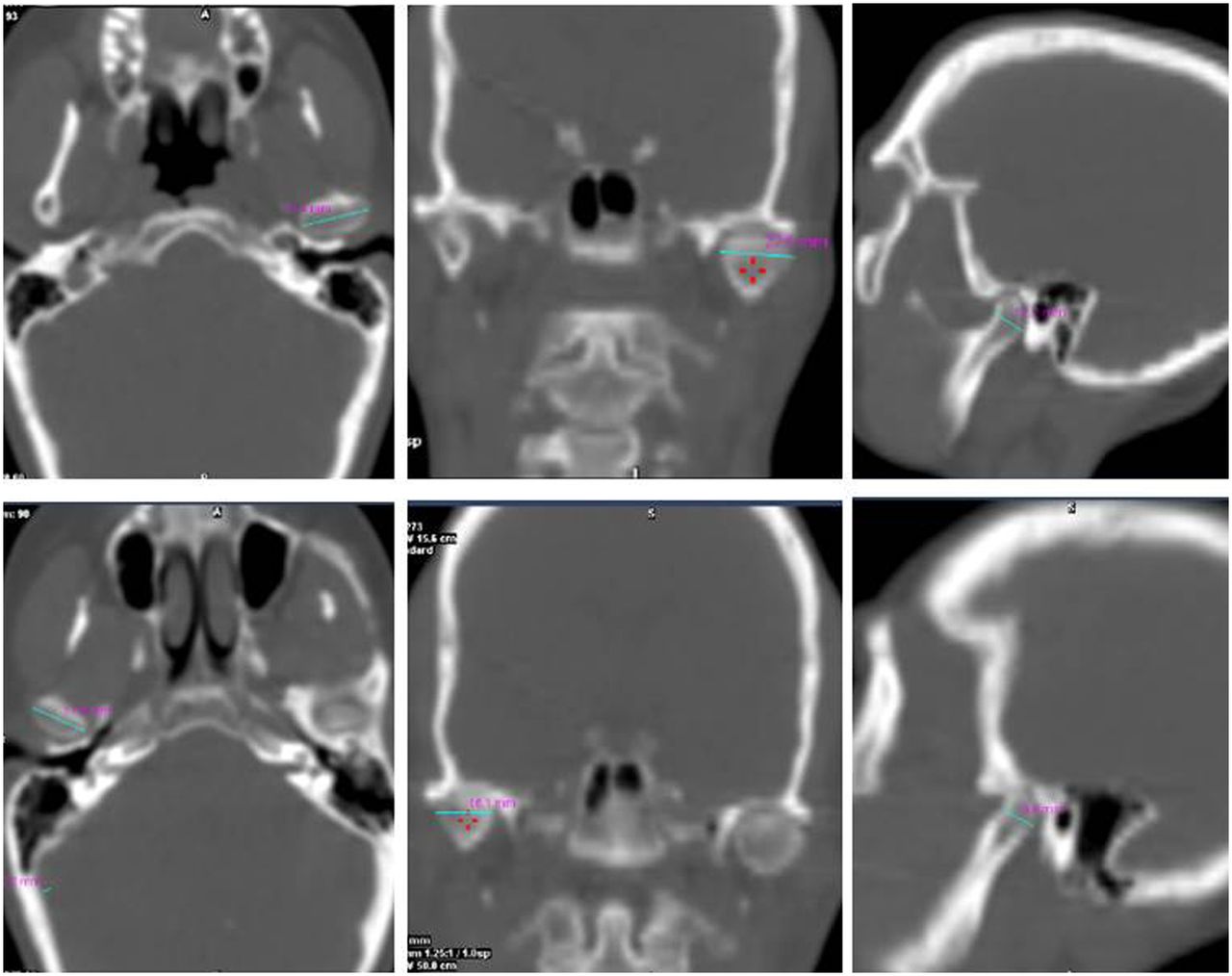
Low-dose CT shows left condyle (top row) as larger than right condyle (bottom row). Left condyle measures 21.4 × 22.5 × 12.2 mm, and right condyle measures 17.8 × 16.1 × 9.8 mm in axial, coronal, and sagittal reconstruction images, respectively.

Serial low-dose CT coronal images show narrowed TMJ spaces with sclerosis that are worse on right side. CT scan was obtained immediately after SPECT scan using 4-slice, low-dose, spiral CT system, at 120 kV and 20 mA, with pitch of 1.75. CT slices were reconstructed at 2.5-mm thickness using standard kernel filter. Radiation dose of this low-dose CT is about 2.7 mSv.
Patients with CH often present with malocclusion and mandibular asymmetry (deviation of the chin to the unaffected side). CH is a self-limiting process that can cease active growth at any time, generally between the ages of 11 and 30 (4).
Bone scans can highlight areas of increased osteoblastic activity, aiding in the diagnosis of active or inactive CH. This can guide treatment decisions: partial condylectomy for active CH or definitive operations for inactive CH. Definitive interventions may involve osteotomies to correct any residual malocclusion or facial asymmetry. Postsurgical deformity may develop if osteotomies are performed while the CH is in an active phase (1).
Consequently, accurate assessment of condylar growth activity is crucial to guiding treatment options. Assessment and diagnosis may be difficult if limited to planar imaging methods. SPECT methods are more sensitive and accurate in detecting growth activity and offer a quantitative means to determine growth differences between the left and right condyles. A 10% or more difference in the radionuclide uptake between the left and right condyles with increased uptake ipsilateral to the CH is considered to be evidence of active, growing CH (1–3).
Normally, the condyles are nearly symmetric and CT is a useful tool to measure and evaluate condylar dimensions (5).
Degenerative or inflammatory arthropathies of TMJs may complicate evaluation of growth activity as these conditions manifest with inherently increased 99mTc-MDP uptake. However, this is generally not problematic as patients present with CH when they are relatively young (1). Degenerative bony changes occur more often and are more severe on the unaffected side than on the affected, hyperplastic side (4). The CT portion of SPECT/CT can be used to evaluate the underlying bony changes to confirm degenerative changes and rule out other possible causes of increased uptake, such as a tumor or trauma.
CONCLUSION
This case suggests that bone scan SPECT/CT provides an accurate means for the assessment of growth activity and detailed underlying anatomic information in a patient with CH. These are helpful not only for diagnosis but also for the choice of an appropriate treatment. Degenerative arthropathies of TMJs may complicate evaluation of comparative uptake, but these conditions are more common and more severe on the side contralateral to the CH.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jun. 25, 2015.
- Received for publication April 8, 2015.
- Accepted for publication June 2, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.