


Abstract
The inguinal lymph nodes are an unusual site of metastases for prostate adenocarcinoma. We present a case in which a 61-y-old man with biochemically recurrent prostate cancer underwent attenuation-corrected 11C-acetate PET/CT, which demonstrated multiple foci of increased activity in the left inguinal, left iliac chain, and right inguinal regions. The attenuation-corrected CT portion of the scan also showed anterior wall thickening of the rectum. The imaging findings were suggestive of metastatic involvement of the rectum below the dentate line with subsequent spread to the inguinal lymph nodes.
Lymphatic spread of prostatic cancer rarely involves the inguinal region. In a patient presenting with inguinal lymphadenopathy, careful consideration of the routes of lymphatic drainage may allow sites of metastasis to be identified. A variety of imaging modalities have been used with variable success to identify and localize sites of recurrence.
CASE REPORT
The institutional review board approved this study, and the requirement to obtain informed consent was waived. A 61-y-old man with a history of prostate cancer (Gleason score 7) was found to have a prostate-specific antigen level of 8.0 ng/mL 20 mo after brachytherapy treatment. A radionuclide bone scan had normal findings. A subsequent CT scan of the abdomen and pelvis revealed multiple enlarged left inguinal lymph nodes, with the two largest measuring 2.3 and 2 cm and several other mildly enlarged nodes measuring less than 1 cm. On the basis of these results, the patient was then referred for an attenuation-corrected 11C-acetate scan PET/CT scan.
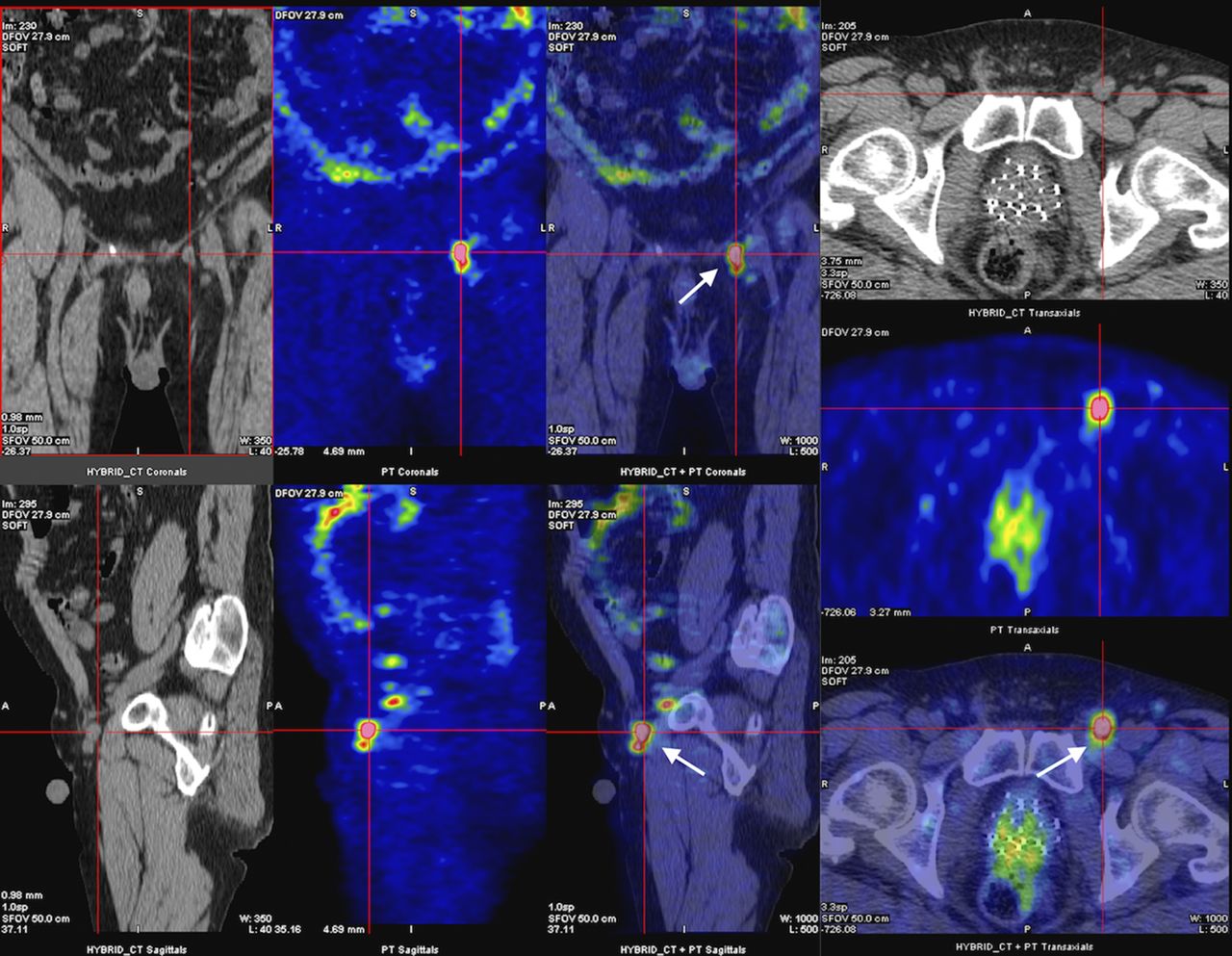
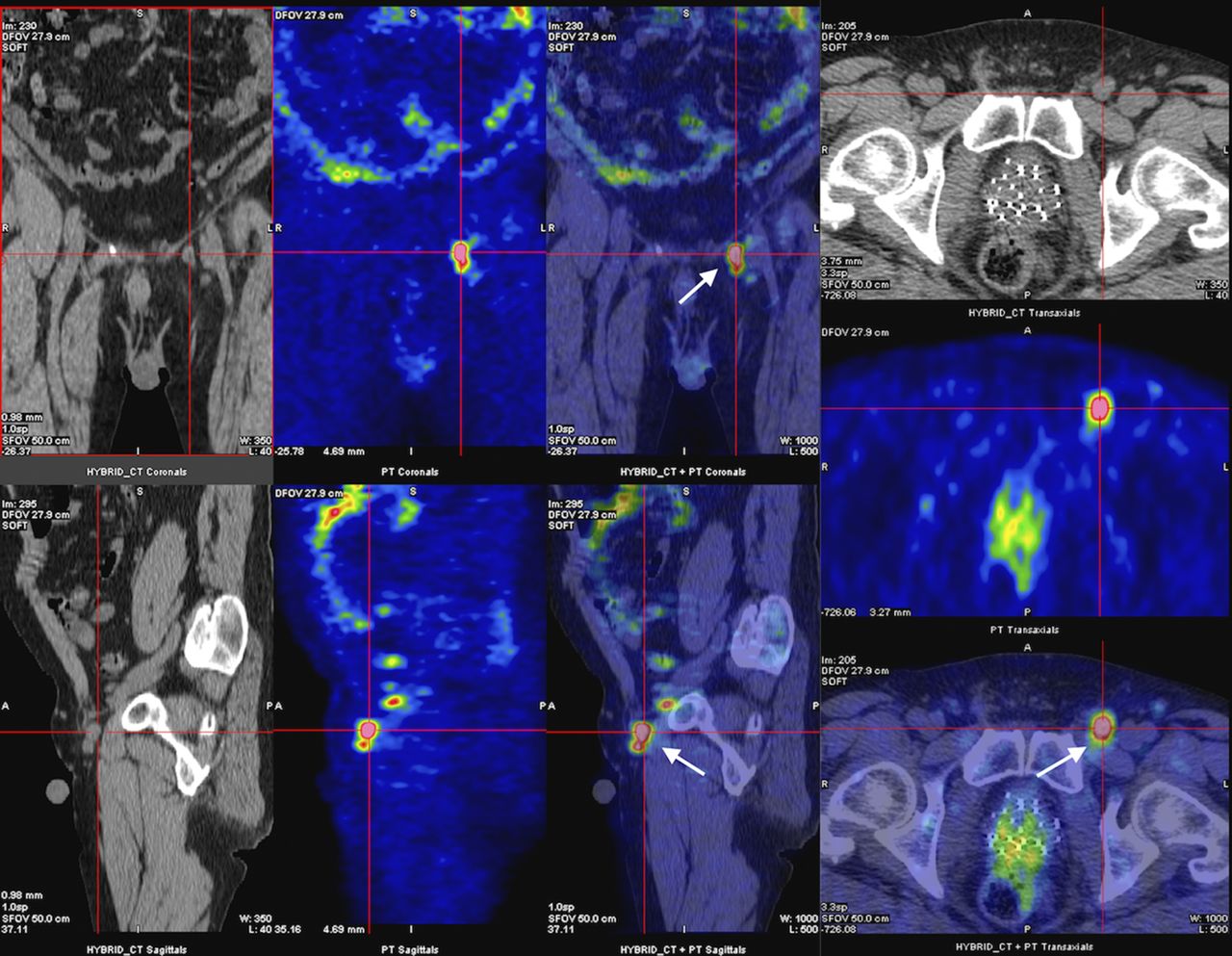
The scan demonstrated a focal concentration of increased metabolic activity (SUVmax 3.92) in the posterior region of the prostate at the interface of the anterior wall of the rectum (Fig. 1). Associated thickening of the anterior wall of the rectum was also demonstrated on the CT portion of the scan.

Attenuation-corrected PET/CT images in axial, coronal, and sagittal views demonstrating increased metabolic activity in posterior region of prostate at interface with anterior wall of rectum (white arrows) (SUVmax 3.92), as well as spread to left inguinal node (yellow arrow).
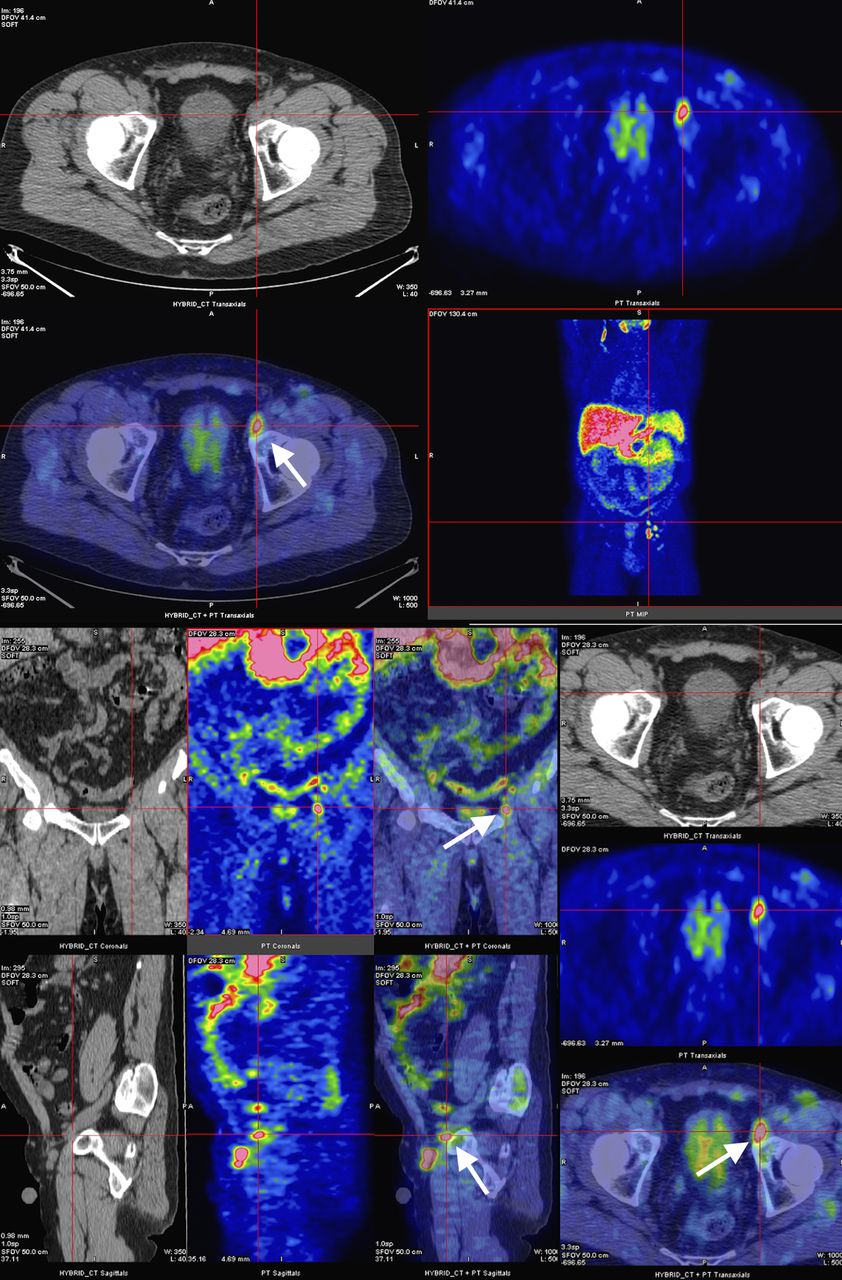
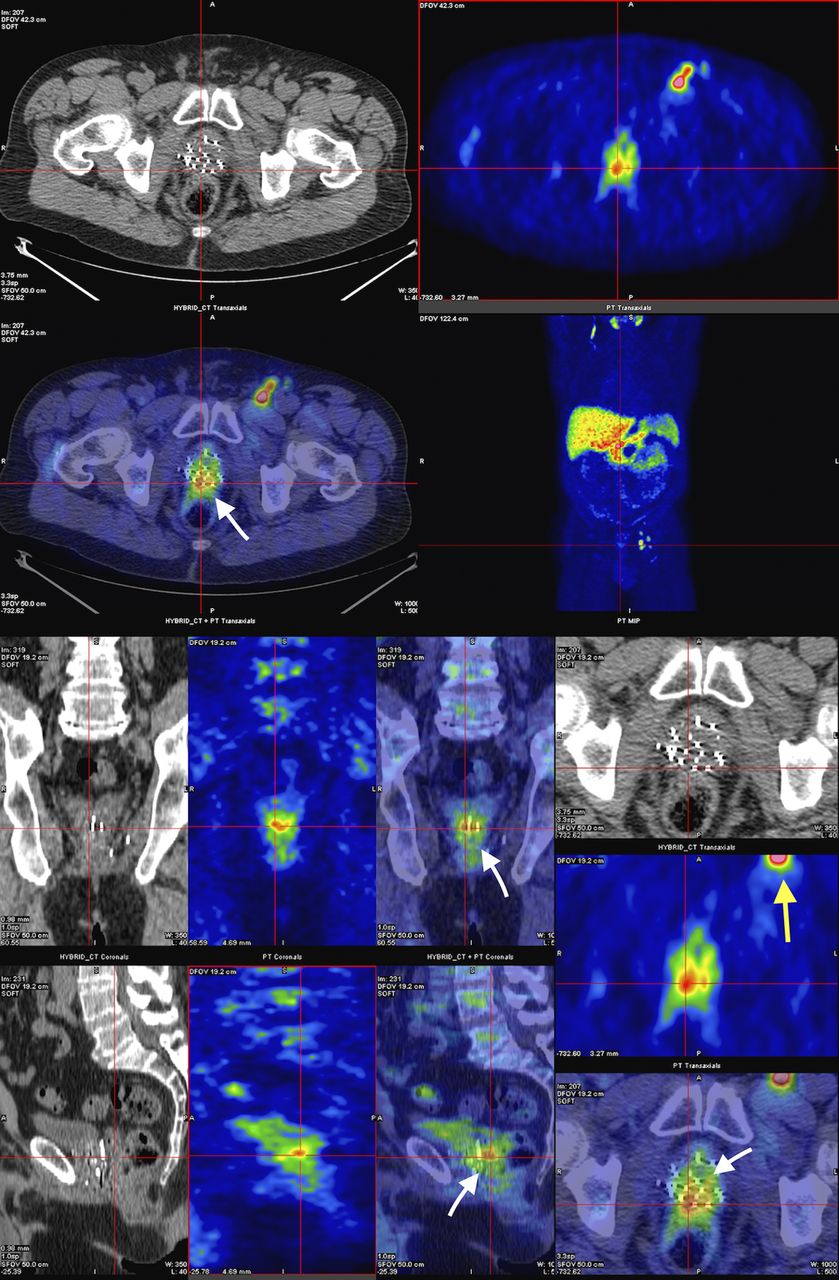
Extensive hypermetabolic lymphadenopathy was noted in the left inguinal region (SUVmax 2.28, 6.11, 4.51, and 5.05) (Fig. 2) and external iliac chain (SUVmax 5.42, 2.28, and 3.39) (Figs. 3 and 4), with a smaller lymph node in the right inguinal area anterior to the femoral neurovascular bundle (SUVmax 1.91).
Attenuation-corrected 11C-acetate PET/CT images in axial, coronal, and sagittal views showing uptake within large left inguinal lymph node (arrows) (SUVmax 6.11).
Attenuation-corrected PET/CT images in axial, coronal, and sagittal views demonstrating increased 11C-acetate uptake within left external iliac chain in node of Cloquet (arrows) (SUVmax 5.42).

Attenuation-corrected PET/CT images in axial, coronal, and sagittal views showing 11C-acetate uptake in proximal left external iliac lymph node (arrows) (SUVmax 3.39).
No osseous metastases were seen. The patient declined biopsy and chose to undergo salvage therapy with intensity-modulated radiation.
DISCUSSION
In the anal canal, the dentate line is the landmark for two different systems of lymphatic drainage: above, to the inferior mesenteric and internal iliac nodes, and below, to the superficial inguinal nodes (1). In prostate cancer, the external and internal iliac, obturator, presacral, and paraaortic lymph nodes are most often involved in primary lymphatic spread (2). Although inguinal lymphadenopathy is rare in prostate carcinoma, involvement of the rectum below the dentate line can be the source of metastasis to inguinal lymph nodes (3,4).
Identification of the precise anatomic location of all involved lymph nodes is mandatory if salvage therapy with intensity-modulated radiation or surgery is to be considered. 11C-acetate, like 11C-choline and 18F-choline, is a radioisotope that has been shown to have a strong positive correlation on attenuation-corrected PET/CT imaging with prostate cancer metastases. Once the patient has achieved a prostate-specific antigen threshold of 1.24 ng/mL or a prostate-specific antigen doubling time of less than 6 mo, the scan achieves a putative sensitivity and specificity of 86.6% and 65.8%, respectively (5). Currently, the best application of attenuation-corrected 11C-acetate PET/CT lies in detecting prostate cancer metastasis after biochemical recurrence or in detecting extraprostatic spread before surgery.
Other metabolic imaging, such as attenuation-corrected 18F-FDG PET/CT, was not performed, as prostate cancer cells are not particularly glucose-avid and studies have shown the superiority of attenuation-corrected 11C-acetate PET/CT (5). Similarly, although multiparametric MR imaging has shown tremendous potential in detecting locally recurrent prostate cancer, further studies are needed to elucidate its usefulness in detecting lymph node metastases.
CONCLUSION
Prostate cancer metastases to the inguinal nodes are rare. In this case, attenuation-corrected 11C-acetate PET/CT effectively demonstrated prostate cancer recurrence with inguinal node uptake, suggestive of metastatic involvement of the rectum below the dentate line.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jun. 25, 2015.
REFERENCES
- Received for publication March 19, 2015.
- Accepted for publication May 26, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.