


Abstract
Hepatobiliary scintigraphy (HBS) is a widely used modality to diagnose biliary injury. In patients with a history of trauma or surgery, the common presentations of bile leaks on HBS are a progressive collection of radiotracer outside the biliary system. However, the precise localization of a bile leak is usually not conveyed by noninvasive techniques including CT or ultrasound or even HBS. This case study of a patient with liver trauma demonstrates a direct bile leak sign leading to recognition of an exact bile leakage site from the left intrahepatic duct. This diagnosis helped clinicians perform less-invasive management.
- hepatobiliary scintigraphy (HBS)
- bile leak
- biliary leak
- hepatobiliary iminodiacetic acid (HIDA) scan
- cholescintigraphy
- hepatic laceration
Hepatobiliary scintigraphy (HBS) is a widely used modality to diagnose biliary injury (1). In patients with a history of trauma or surgery, the common presentations of bile leaks on HBS are a progressive collection of radiotracer outside the biliary system (2). However, the precise localization of a bile leak is usually not conveyed by noninvasive techniques including CT or ultrasound or even HBS (3,4).
CASE REPORT
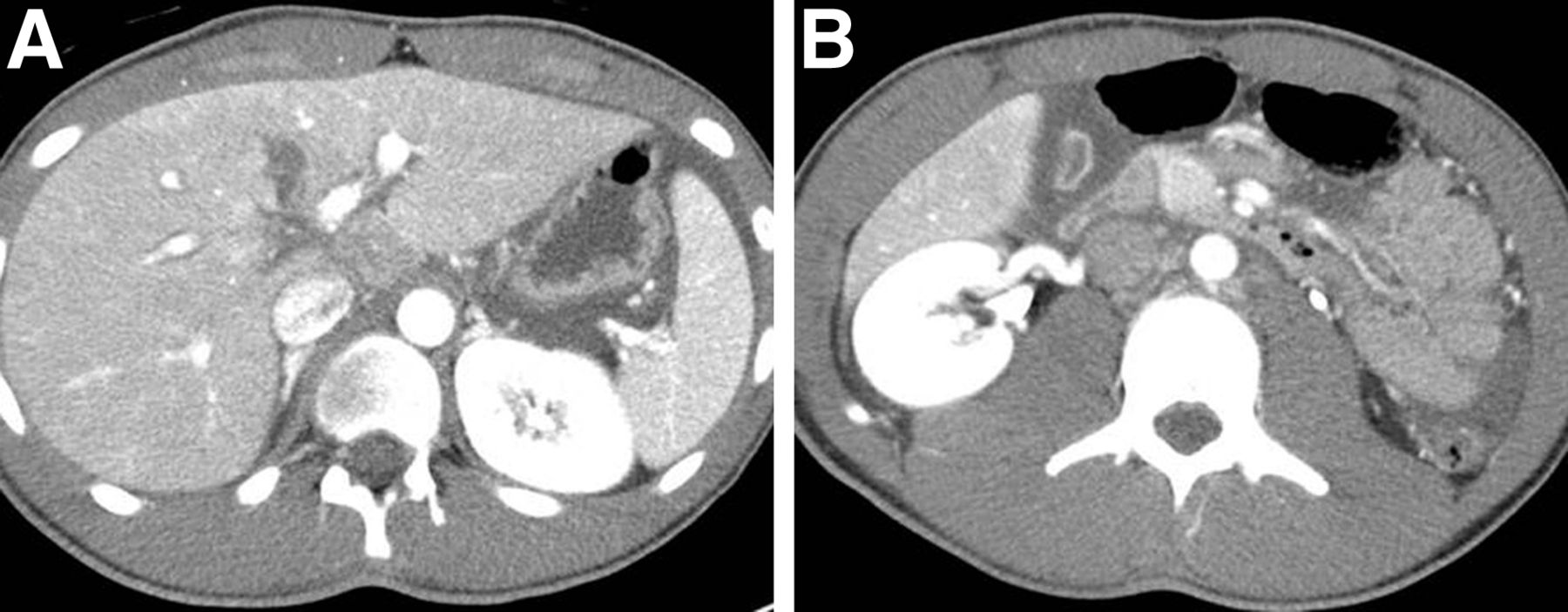
A 16-y-old male (who along with his parent gave permission to use the data from his studies for our article) presented with injuries from a motor vehicle accident. A CT scan of the abdomen/pelvis with contrast demonstrated central hepatic laceration with extension into gallbladder fossa and peritoneal fluid. HBS was required to determine whether a biliary injury was present or not.
After intravenous administration of 99mTc-mebrofenin, sequential dynamic abdominal images were obtained over 60 min (Fig. 1). Images showed an area with decreased activity over the region between the 2 hepatic lobes, corresponding with the known hepatic laceration seen on the CT (Fig. 2). Over time, there was a progressive accumulation of tracer outside the biliary system over the inferior left hepatic lobe. A couple of lines of tracer uptake connected this abnormal focal area to the left intrahepatic duct. Eventually, this abnormal tracer accumulation spread throughout the abdomen. These findings indicated an exact bile-leaking site at the left intrahepatic duct.

HBS over 60 min shows area with decreased activity over region between the 2 hepatic lobes, corresponding with known hepatic laceration seen on CT (black arrow). Over time, there is a progressive accumulation of tracer outside the biliary system over inferior left hepatic lobe (pink arrow). A couple of lines of tracer uptake (red arrows) connected this abnormal focal area to left intrahepatic duct. Eventually, this abnormal tracer accumulation spread throughout abdomen (blue arrows). These findings indicate exact bile-leaking site at left intrahepatic duct.
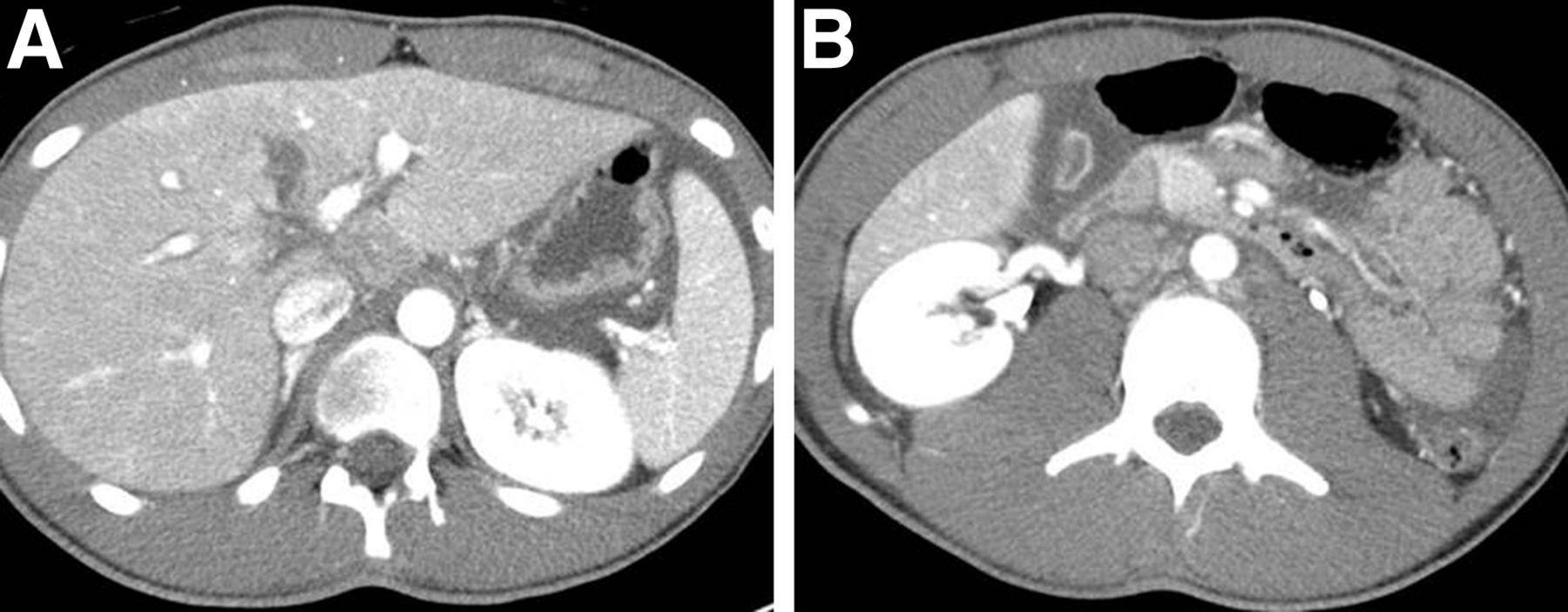
CT images of abdomen/pelvis with contrast demonstrate central hepatic laceration.
Subsequently an endoscopic retrograde cholangiopancreatography with initial cholangiogram confirmed the findings of the HBS (Fig. 3). Sphincterotomy and placement of 2 common bile duct stents were performed. Soon after, a diagnostic laparoscopy further confirmed a bile leak from the left hepatic duct, and a laparoscopic lavage and intraperitoneal drainage were performed. The patient did well postoperatively and was discharged with no extravasation of contrast in the follow-up endoscopic retrograde cholangiopancreatography with cholangiogram after the removal of common bile duct stents.

Endoscopic retrograde cholangiopancreatography with cholangiogram shows accumulation of contrast outside biliary system over inferior left hepatic lobe (yellow arrow). Line of contrast (red arrow) connects this abnormal focal area to left intrahepatic duct.
DISCUSSION
Bile leaks can occur after surgery or trauma. Imaging modalities used to detect bile leaks are CT, endoscopic retrograde cholangiopancreatography, MR cholangiopancreatography (MRCP), ultrasound, and HBS. Among these, only HBS and MRCP, noninvasive studies, can identify abnormal fluid collection as bile. However, there are limitations to emergency MRCP, including lack of readily available MR imaging equipment, technologists, personnel experienced with interpreting MRCP, and higher cost (4). Therefore, HBS is the commonly used modality to diagnose biliary injury (1).
HBS is a highly sensitive imaging modality and useful for early diagnosis of bile leaks. HBS can determine whether a fluid collection seen on ultrasound or CT is of biliary origin (1,2). HBS can determine the rate of leakage and can be used as a follow-up tool (1,2). A common finding of a bile leak is the radiopharmaceutical’s progressive accumulation outside the biliary system, either localized (bilomas) or diffuse. An accurate localization of a bile leak is difficult by HBS because of the lack of anatomic details. However, this localization is important because of the shift in management strategy from very invasive to minimally invasive (3).
This case demonstrates a direct bile leakage sign, bile communication tracks connecting a left intrahepatic duct to a biloma over the inferior left hepatic lobe. This direct sign leads to recognition of an exact bile-leaking site in the left hepatic duct and helps determine a bile leak type. A management approach can be selected on the basis of the bile leak’s type (5). In our case, a less-invasive management was used based on the HBS findings.
Accurate localization of the site of bile leak through a direct sign, bile communication tracks, can be obtained with HBS as shown in this case. Determining the site of a bile leak will further increase opportunities to detect an accurate bile leakage site in improved HBS with SPECT (SPECT/CT). The HBS SPECT/CT provides both anatomic and functional information and overcomes the lack of specificity of CT alone or detailed anatomic information of HBS alone (3).
CONCLUSION
Although the precise site of a bile leak is often difficult to detect with noninvasive techniques, it is possible with HBS. Knowledge of the bile leak site will increase opportunities to detect the direct sign of a bile leak in advanced HBS with SPECT/CT. This is vital given the change in approach regarding management of a bile leak from more invasive to less invasive.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jun. 25, 2015.
- Received for publication January 30, 2015.
- Accepted for publication May 14, 2015.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.