


Abstract
When unexpected results are obtained with standard image collection, the nuclear medicine physician must consider many technical factors that may have contributed. When image quality is poor, prior radiotracer administration, among other things, should always be considered. Our case demonstrates how knowledge of patient history and basic principles of nuclear medicine physics allows recognition of the septal penetration artifact. This allows the nuclear medicine physician to tailor the exam to an individual patient and obtain the most useful diagnostic information for the clinician.
In nuclear medicine practice, it is important to understand the source of an unreadable image. Often, a comprehensive understanding of the patient’s clinical history and a fundamental knowledge of the underlying nuclear medicine physics can aid the physician in these situations.
CASE REPORT
A 56-y-old man with a history of metastatic papillary thyroid cancer (follicular variant) presented for a follow-up 123I whole-body scan. The patient gave permission to use the data from his studies for our article. He had undergone thyroidectomy and received external-beam radiotherapy for spinal metastases in the past. Nearly 1 y previously, he had also undergone a single 131I treatment with 5,550 MBq (150 mCi). The intention at the time of his visit was to perform a diagnostic scan before a possible repeated high-dose radioiodine treatment, as his thyroglobulin level had recently been increasing and measured 2,476 ng/mL. According to our routine departmental practice, 92.5 MBq (2.5 mCi) of 123I were administered by a technologist for this diagnostic scan. At 24 h after 123I administration, whole-body scintigrams (Fig. 1) following the standard protocol were obtained. After the initial images had been reviewed, a change was made in the acquisition protocol and a second set of whole-body scintigrams was obtained (Fig. 2). These second images allowed adequate characterization of the tumor burden for the clinician. The patient was treated with the high dose of 131I later that day on the basis of these findings.

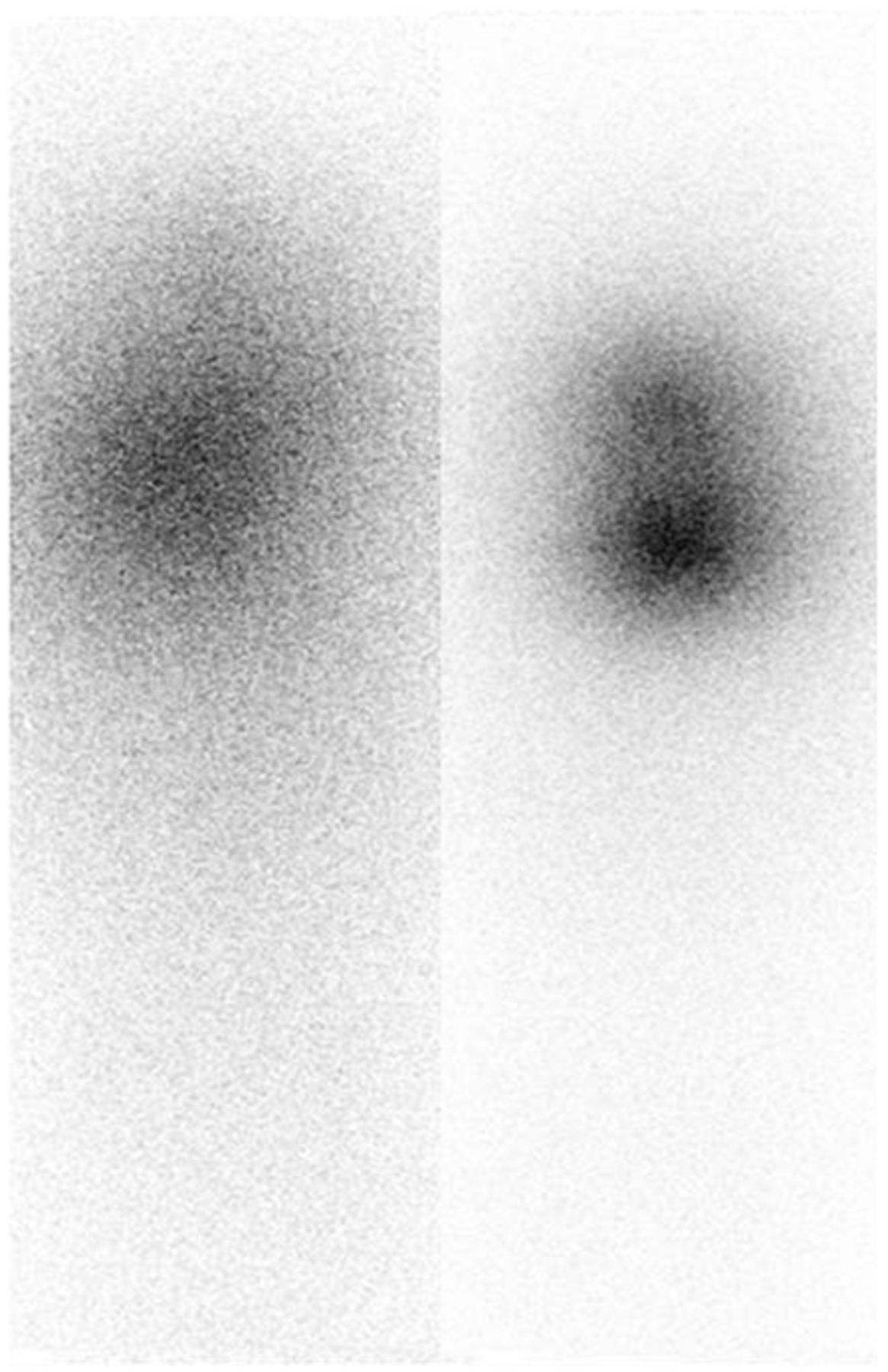
Anterior (left) and posterior (right) views of 123I whole-body scan demonstrate blurred images.

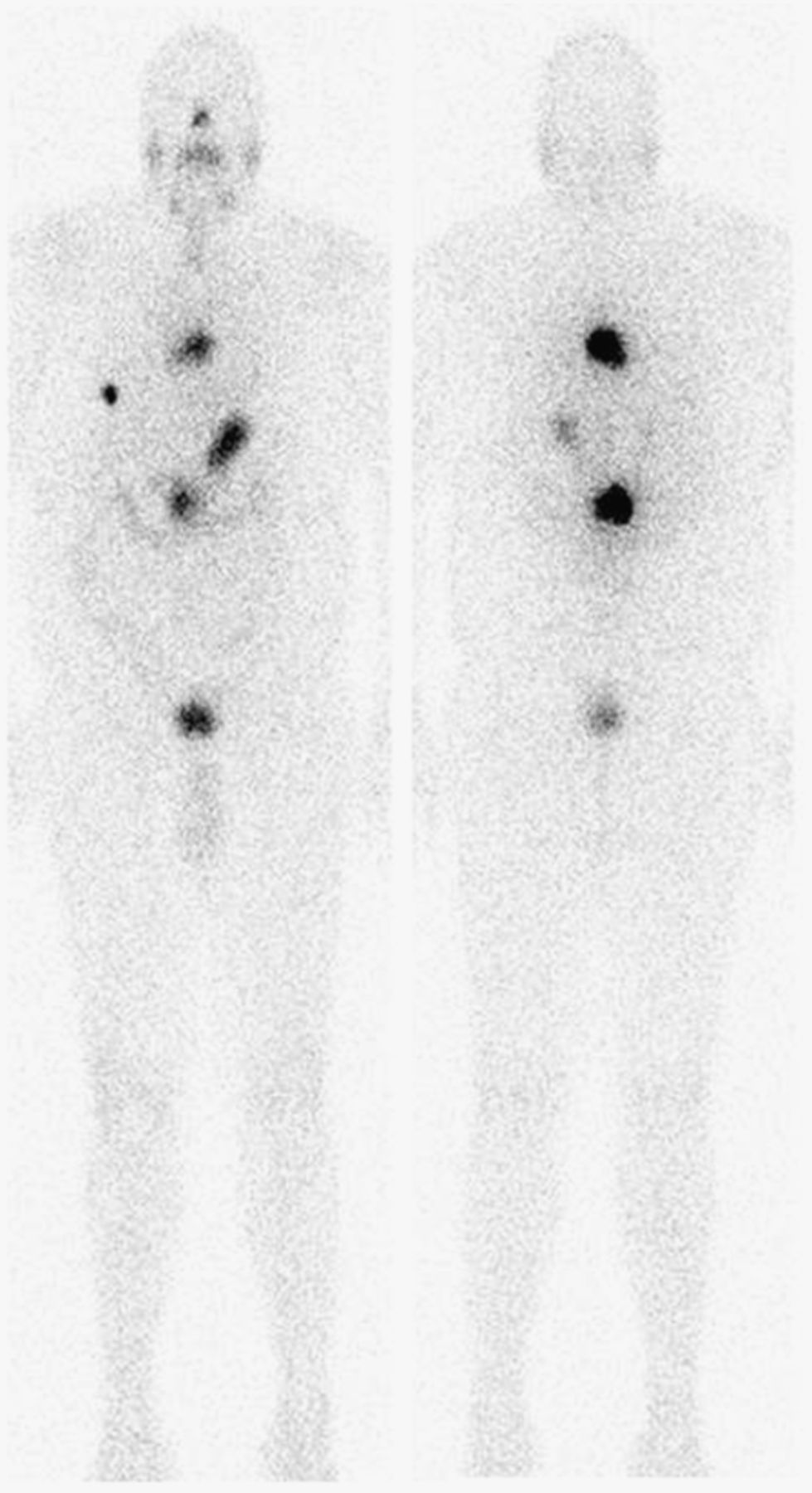
Anterior (left) and posterior (right) images of second 123I scan with medium-energy collimator show new lesion in right hemithorax; persistent metastatic disease at levels T6, L1, and L2; and small area of questionable residual functioning thyroid tissue in neck.
DISCUSSION
The first set of images was clearly nondiagnostic. The images were blurred and had low spatial resolution. Possible technical causes of the blurred images included a camera that was off the photon peak, patient motion, an improper distance between the camera and the patient, and interference from prior radiotracer administration. After reviewing the patient’s history, we found that the patient had received 92.5 MBq (2.5 mCi) of 131I 16 d before this scan. However, he had not been able to return for a diagnostic image after the administration because of a family emergency. The current scan was a repeated order by the referring clinician. Therefore, we hypothesized that increased septal penetration from the previously administered 131I had led to decreased spatial resolution, and the decision was made to switch from a low-energy to a medium-energy collimator. The resolution of the second set of images obtained with a medium-energy collimator was dramatically improved.
Among existing collimators, parallel-hole collimators receive the most use in nuclear medicine studies (1). The parallel holes forming an array perpendicular to the plane of the scintillation crystal serve to prevent scatter and tangential γ rays from reaching the detector crystal. Commonly, 99% of the available photons are absorbed by the collimator septa and are not detected (2). The septal thickness further defines the energy limitation of a collimator. This design allows one to best match the collimator design with radionuclides of differing photon energy. When a high-energy isotope is administered, use of a low-energy collimator results in high-energy photon penetration of the thin septa. This leads to a blurred image or a star artifact (3) because of an increased number of scattered photons and significant degradation of spatial resolution. This effect is observed in the first set of images.
In our particular case, the previously administered 131I (high-energy photon, 364 keV; 8.04-d half-life) had not decayed to a sufficiently low level before the repeated 123I whole-body scintigrams were obtained. A medium-energy collimator was used in the second set of images to decrease the remaining 131I high-energy septal penetration while still allowing for sufficient detection of the lower-energy 123I photons (159 keV). Choosing a collimator properly matched to the available radiation produced acceptable diagnostic images.
The second set of images demonstrated a new lesion in the right hemithorax; a persistent metastatic lesion at the level of T6, L1, and L2; and a small area of questionable residual functioning thyroid tissue in the neck, compared with the previous examination performed 1 y previously. Retrospectively, further image improvements might have been realized through use of a high-energy collimator for the repeated image acquisition.
CONCLUSION
This case highlights the importance of patient clinical history, individual radioisotope energy and decay properties, and collimator design in obtaining useful diagnostic information. A deviation from the standard protocol may be necessary to tailor each examination to the individual patient.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Aug. 28, 2014.
- Received for publication December 18, 2013.
- Accepted for publication April 21, 2014.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.