


Abstract
The objective of the study was to make a quantitative comparison of 24-h thyroid uptake calculated by γ camera–based and thyroid uptake probe–based methods after administration of a diagnostic 131I capsule in patients with benign thyroid disorders. Methods: The study group comprised 66 patients, of whom 26 were male (28–67 y old) and 40 female (20–65 y old). These patients had benign thyroid disorders (primarily hyperthyroidism [thyrotoxicosis]), most of whom had been referred for evaluation before radioiodine treatment. 131I (25 μCi [925 MBq]) was administered, and 24-h thyroid uptake was calculated using a probe-based method and a camera-based method with a medium-energy parallel-hole collimator. The paired t test was used to check the variation in values obtained by these 2 methodologies. Result: Of the 66 patients included in this study, 45 had clinical thyrotoxicosis and 21 had nonthyrotoxic multinodular goiter. In the group with thyrotoxicosis, neck uptake ranged from 40.13% to 97.1% by the probe-based method and 36.89% to 95.9% by the camera-based method. In the group with clinically nonthyrotoxic goiter, neck uptake ranged from 1.4% to 38.4% by the probe-based method and 0.6% to 34.8% by the camera-based method. Paired t testing was performed on both groups of patients, and P values were less than 0.05, showing good agreement within the 2 groups of data. Conclusion: The camera-based method is a good substitute for the probe-based method; though not producing identical results, the former could be used to derive useful quantitative information on thyroid function.
Radioiodine (131I) therapy is an effective and well-tolerated option in patients with hyperthyroidism (thyrotoxicosis) due to Graves disease and thyrotoxic multinodular goiter and in certain cases of nonthyrotoxic multinodular goiter. Before the use of 131I therapy is considered, radioiodine (sodium iodide) uptake scanning is frequently applied in these patients, particularly when the cause of the thyrotoxicosis is in question. Conditions associated with elevated or normal uptake can be distinguished from those associated with near-absent uptake (e.g., painless postpartum thyroiditis, subacute thyroiditis, or ingestion of thyroid hormone) (1–4). The thyroid scan in this clinical context helps especially in determining the presence of nodularity: the uptake pattern in solitary thyrotoxic adenoma generally is focal in the adenoma and suppressed in the surrounding and contralateral thyroid tissue, whereas in thyrotoxic multinodular goiter there are multiple areas of focally enhanced and suppressed uptake. Although 123I is preferred for diagnostic scanning, 131I continues to be used in several developing nations where 123I is currently not available.
Although most academic medical centers estimate thyroid uptake by using a thyroid uptake probe (which is ideal), some do not have this instrument and hence use pertechnetate (99mTcO4−) scanning with a γ camera–based method. 99mTcO4− is trapped by the thyroid but is not organified. This can result in a narrow range of normal uptake and high background activity, but total-body radiation exposure is less since 99mTc does not have a β component. In addition, in nodular disease there may be discordance between radioiodine and 99mTc images, since pertechnetate is not handled by the same physiologic mechanism as iodine. For patients with differentiated thyroid cancer, the usual administered activity is 37–185 MBq (1–5 mCi) of 131I orally, and the neck and entire body are imaged at 48–96 h (5). In this study, we prospectively made a direct comparison of 24-h 131I uptake in the same patient using a camera-based method (with a medium-energy parallel-hole collimator) and a probe-based method in a spectrum of benign thyroid disorders after administration of a 925-MBq (25-μCi) 131I capsule.
MATERIALS AND METHODS
Patient Preparation
The patients included in the study had benign thyroid disorders (primarily thyrotoxicosis), and most had been referred for evaluation before treatment (6–9). The standard precautions for radioiodine scanning were taken (with regard to iodine-containing substances and thyroid medications), including exclusion of pregnant or lactating patients. 131I (925 MBq) was orally administered, and 24-h thyroid uptake was estimated by probe- and camera-based methods.
Study Population
Sixty-six patients undergoing 925-MBq 131I scanning in 2012 or 2013 were included. Twenty-six were male (28–67 y old) and 40 female (20–65 y old). Most had thyrotoxicosis and were undergoing this procedure as a routine step before being considered for 131I therapy. The included patients primarily had Graves disease, thyrotoxic nodular goiter (either an autonomous nodule or thyrotoxic multinodular goiter), or nonthyrotoxic multinodular goiter.
Method for Probe-Based Uptake Calculation
A thyroid uptake probe (Nuclear Chicago) with a flat-field collimator was used to take the neck count. A 925-MBq standard 131I capsule was kept in a neck phantom and counted for 100 s using the probe. The distance between the γ camera collimator and the phantom or neck was taken to be 8 cm (which is the closest possible for all patients). The background count was calculated using a lead neck shield, and the background-corrected count was taken as the true count. The count was taken with the phantom positioned 30 cm from the probe (isoresponse distance). The patient was positioned 30 cm from the probe, and the count was taken for 100 s to obtain the count used to calculate 24-h uptake. The neck was shielded and the count taken for 100 s to obtain the background count. Percentage uptake was calculated using the following formula: .
.
Method for Camera-Based Uptake Calculation
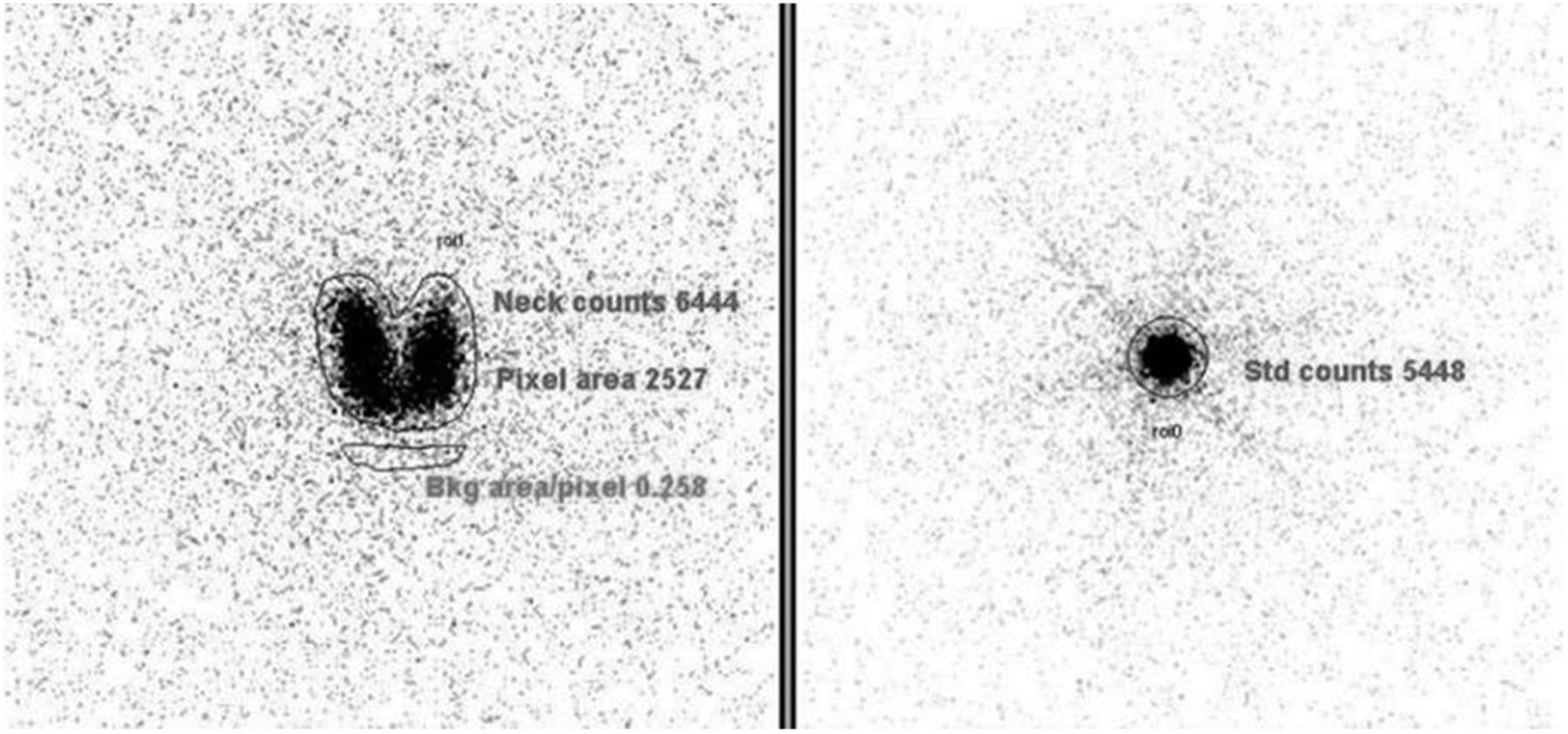
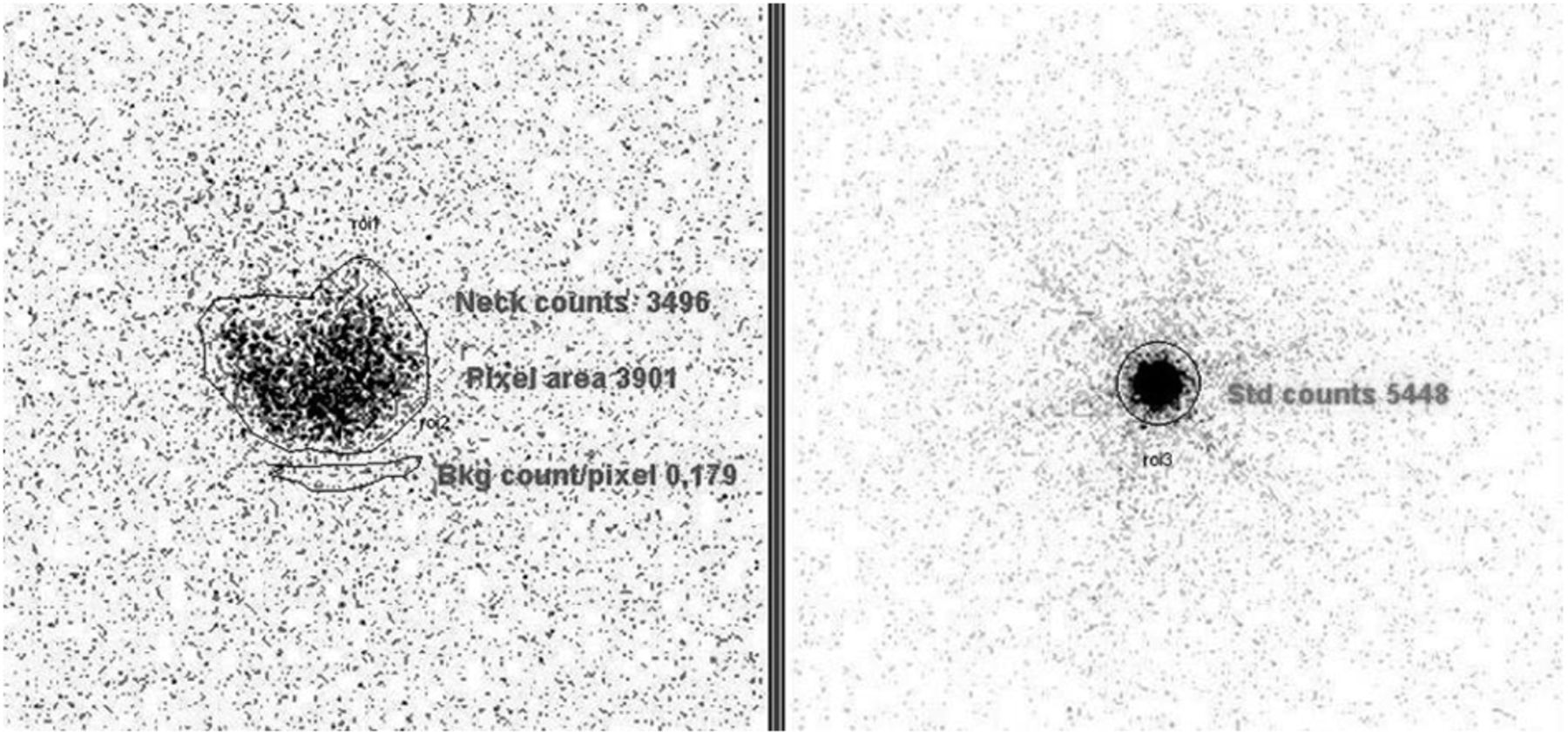
On the same group of patients, the camera-based method was then used to calculate 24-h neck uptake. To obtain the standard counts, the 131I capsule in the neck phantom was scanned for 5 min, and counts were calculated by drawing a region of interest around the capsule and standardizing with scan time. The neck scan was obtained by positioning the patient supine with neck extended. A γ camera with a medium-energy collimator (Infinia; GE Healthcare) was used. The scan was acquired for 5 min with the energy window centered on 364 keV. A region of interest was drawn around the thyroid to get the neck counts, and the total pixel area was noted. A background region of interest was drawn near the thyroid to obtain the average background per pixel (7) (Figs. 1 and 2).

Scintiscan of camera-based uptake in 45-y-old man with diffuse thyrotoxic goiter. Probe-based 24-h 131I uptake was 74.3%, whereas camera-based uptake was 75.9%.
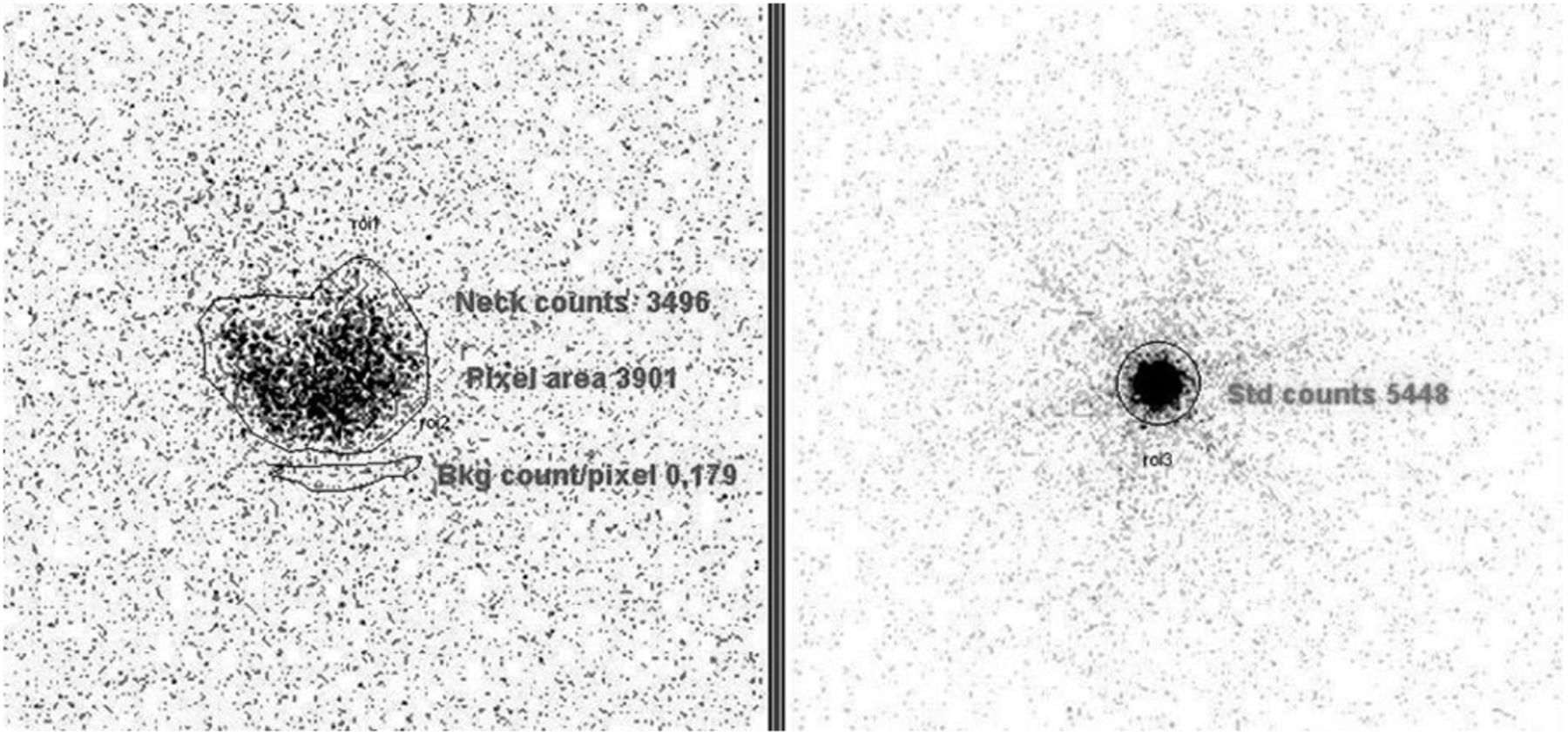
Scintiscan of 24-h 131I uptake in 45-y-old woman with nonthyrotoxic multinodular goiter. Probe-based 24-h 131I uptake was 23.17%, whereas camera-based uptake was 21.7%.
Percentage uptake was calculated using the following formula: .
.
RESULTS
Of 66 patients included in this study, 45 were thyrotoxic and 21 were nonthyrotoxic (Tables 1 and 2).
Data for Nonthyrotoxic Patients
Data for Thyrotoxic Patients
In the thyrotoxic patients, neck uptake ranged from 40.13% to 97.1% (71.9 ± 16.22) by the probe method and 36.89% to 95.9% (70.67 ± 16.62) by the camera method (Fig. 3). In the nonthyrotoxic patients, neck uptake ranged from 1.4% to 38.4% (mean ± SD, 26.3% ± 9.7%) by the probe method and 0.6% to 34.8% (mean ± SD, 25.7% ± 10.5%) by the camera method (Fig. 3). A good correlation coefficient (0.99) was observed between the probe- and camera-based uptake values. Paired t testing on both groups of patients confirmed the good correlation between the probe- and camera-based uptake values (P < 0.05).
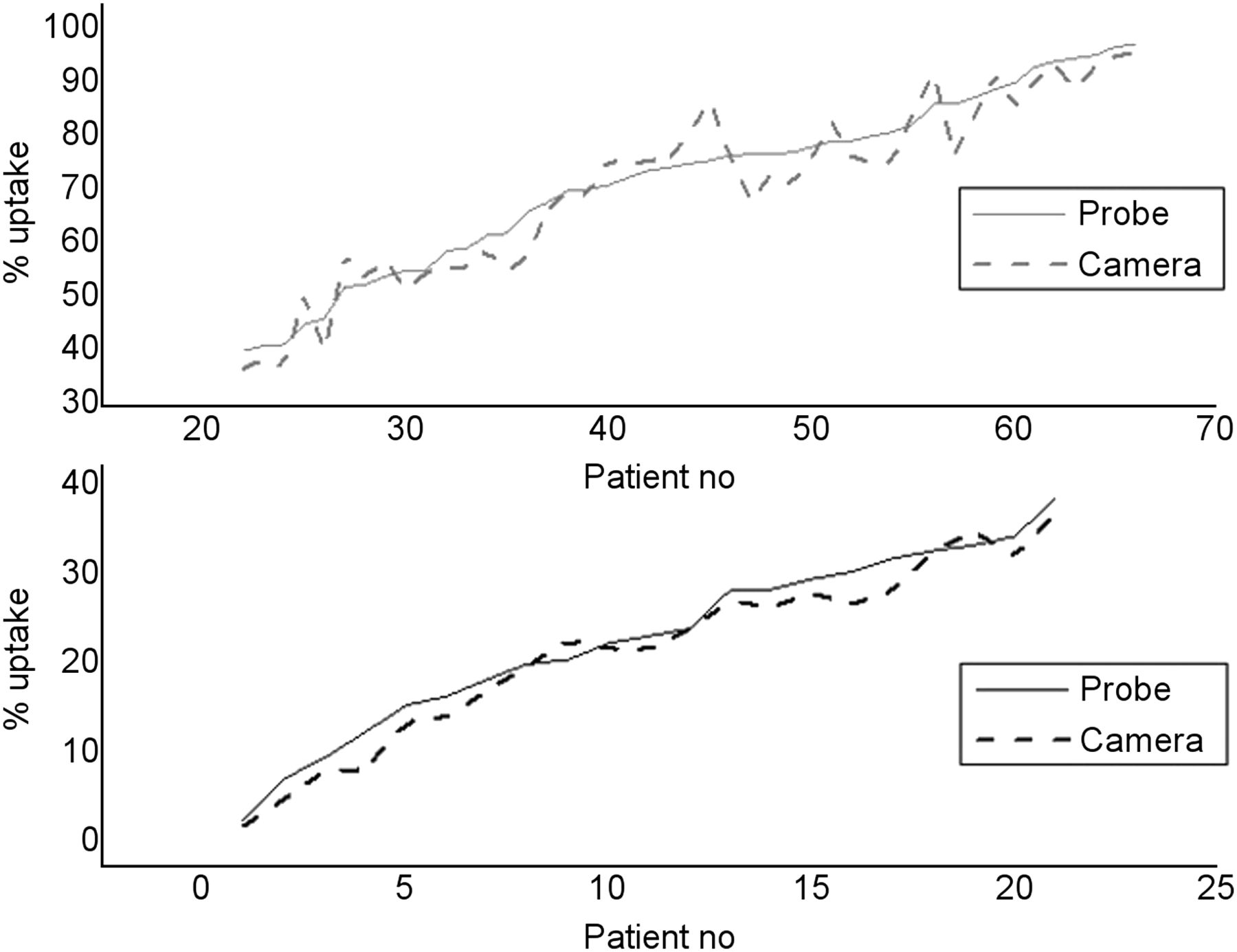
Graphs of probe-based and camera-based uptake calculated in all patients. Neck uptake values calculated by probe and camera are plotted against individual patients in thyrotoxic group (top) and nonthyrotoxic group (bottom). Correlation coefficient of 0.990659 was obtained between the 2 methods when all patients were considered together.
DISCUSSION
Evaluation of thyroid function with radiopharmaceuticals such as 123I, 99mTcO4−, and 131I has been used in various nuclear medicine centers in the work-up before radioiodine therapy. Although the preferred radiopharmaceutical for thyroid uptake and scintigraphic studies is 123I, it is not available in several countries, and 131I is the low-cost, easily available substitute that is widely used. The recommended time of measurement is approximately 24 h after radiopharmaceutical administration, and the standard instrument is a thyroid uptake probe. When a probe is not available, a γ camera with a parallel-hole collimator can be used, but the use of a standardized neck phantom remains necessary. Scanning of 99mTcO4− uptake has also been used in centers that do not have access to 123I or an uptake probe. However, a 99mTcO4− thyroid uptake study is not a substitute for the traditional iodine uptake study, as 99mTcO4− cannot give the true functional information that iodine can provide. Hence, it has been suggested that an approach be validated vis-à-vis the standard 24-h uptake values for appropriate interpretation.
Research studies to this end have been performed by various investigators to validate modifications of the standard recommended procedure. Wasilewska-Radwanska et al. compared 99mTcO4− thyroid uptake measured using a γ probe and a γ camera and observed a good correlation (10). 123I is a better substitute for 131I because of its favorable physical characteristics (11) for imaging. Studies have demonstrated that 4-h 123I uptake can be a substitute for 24-h 131I uptake(11), eliminating the need for patients to visit the center again on the next day. Although 123I gives better imaging and minimum radiation dose to patients, its availability and cost are the challenges and the reason for its limited use in developing countries.
Thyroid uptake calculation using a thyroid probe is the conventional method. In this study we have shown that camera-based 131I thyroid uptake can be a good substitute for the probe-based method. Thyroid uptake values obtained by these 2 methods correlated well (P < 0.05) in both thyrotoxic and nonthyrotoxic patients. In a previous study (12), a similar comparison was undertaken with 123I and a low-energy all-purpose collimator, whereas this study was done with 131I and a medium-energy collimator and the population was more than double that in the previous comparison. We believe that the results of the present study can be particularly useful for centers that do not have a thyroid uptake probe. For want of such a probe, many of these centers use 99mTcO4− uptake scanning for decision making. Furthermore, the uptake calculation and the scanning could be undertaken in the same sitting in these patients.
CONCLUSION
We have shown promising results for camera-based thyroid uptake, which can substitute well for the probe-based methodology. Nuclear medicine centers that do not have a dedicated thyroid probe can use this method to obtain quantitative information in a single scan. However, we recommend that individual centers perform a comparative evaluation and standardization before adoption of the camera-based method into clinical routine.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jun. 26, 2014.
REFERENCES
- Received for publication February 18, 2014.
- Accepted for publication April 18, 2014.





{kind=link}
{kind=link}
{kind=link}