


Abstract
Preoperative injection of radiocolloid for axillary sentinel node biopsy in breast cancer is uncomfortable for patients. This study evaluated the reliability of radiocolloid injection as determined by sentinel node identification rate and positive sentinel node biopsy rate, after the patient has been anesthetized in the operating room as compared with preoperative injection. Methods: After institutional review board approval, a retrospective cohort of patients with breast cancer who underwent sentinel node biopsy from January 2005 through December 2010 was evaluated for analysis. Patients who received intraoperative injection of radiocolloid were compared with those who received their injection preoperatively. Patients with incomplete pathologic staging or having received neoadjuvant chemotherapy were excluded. All patients received radiocolloid injections into the retroareolar tissue; some also received intradermal injection directly over the tumor. All injections contained 37 MBq (1 mCi) in 0.5 mL of filtered (0.22-μm) 99mTc-sulfur colloid. Results: Over the 6-y study period there were 904 sentinel node biopsy procedures, and 165 patients were excluded from analysis. Of the 739 sentinel node biopsies that were analyzed, 647 had preoperative injection of radiocolloid and 92 had intraoperative injection. The overall sentinel lymph node identification rates were similar for the 2 groups: 93.5% for the preoperative injection group and 94.6% for the intraoperative injection group (not statistically significant). The identification rates remained comparable for both groups when analyzed by T stage of the tumor. The average number of sentinel lymph nodes removed was similar between preoperative and intraoperative injection: 2.60 and 2.70 nodes, respectively. The overall rates of positive sentinel nodes were comparable for the 2 groups: 25.6% for the preoperative injection group and 26.4% for the intraoperative injection group (not statistically significant). When analyzed by T stage, the positive sentinel node rates remained similar between the 2 groups. Conclusion: The sentinel lymph node identification rate of 94.6% for the intraoperative injection group was similar to other published sentinel lymph node identification rates (96%–100%). The positive sentinel lymph node rate was also comparable to that of published series. Intraoperative injection of radiocolloid for axillary sentinel node biopsy appears equivalent to preoperative injection and is a less painful experience for breast cancer patients.
For breast cancer, the axillary nodal status has been crucial in determining the prognosis and indication for adjuvant systemic chemotherapy and adjuvant locoregional radiation therapy. Routine axillary nodal staging with axillary dissection, however, has not affected survival but has been associated with increased risk for ipsilateral upper-extremity lymphedema. To avoid nontherapeutic axillary dissection and reduce the incidence of lymphedema, axillary sentinel node biopsy has become the standard of care for axillary nodal staging of breast cancer. With sentinel node biopsy, only a few axillary nodes are selected and excised for pathologic evaluation rather than the anatomically directed axillary dissection. The preparation for sentinel node biopsy most frequently requires a preoperative injection of radiocolloid. A handheld radiation probe is then used intraoperatively to identify any radioactive sentinel nodes for excision.
To permit sufficient time for the injected radiocolloid to travel from the injection site to the axillary sentinel node, the radiocolloid is injected before the patient is anesthetized for the operation. Because the injection of radiocolloid is directed into the ipsilateral breast and frequently into the retroareolar space, the procedure is visibly uncomfortable for most patients. To reduce the pain experienced, some investigators have proposed performing the radiocolloid injection after the patient has undergone anesthesia. This study sought to determine whether injection of the radiocolloid once the patient has been anesthetized is comparable to preoperative injection for sentinel lymph node identification.
MATERIALS AND METHODS
This was a noninferiority retrospective study. The primary objective was to compare the sentinel node identification rate between patients with intraoperative injection of radiocolloid and those with preoperative injection. The hypothesis was that the identification rate of sentinel nodes in patients with intraoperative injection is not lower than the rate in those with preoperative injection. The secondary objective was to compare the positive sentinel node rate between preoperative and intraoperative injection. After we received institutional review board approval to collect data, we identified eligible patients through the Massey Cancer Center patient registry. The inclusion criterion was any patient who underwent sentinel node biopsy for breast cancer at Virginia Commonwealth University Health System (VCUHS) from January 1, 2005, through December 31, 2010. Patients whose records were incomplete with regard to breast cancer stage and sentinel biopsy were excluded. Patients who were treated with neoadjuvant chemotherapy before sentinel node biopsy were also excluded.
Injection with 37 MBq (1 mCi) in 0.5 mL of filtered (0.22-μm) 99mTc-sulfur colloid is used for sentinel node mapping at VCUHS. The site of radiocolloid injection for sentinel node localization varies among the 5 surgical oncologists who were active during the study period. All surgeons inject in the subareolar location; some surgeons also include peritumoral or intradermal injection of the radiocolloid. All but one surgeon usually injects the radiocolloid agent before anesthesia in the preoperative holding area. One surgeon routinely injects after induction of anesthesia in the operating room; other surgeons occasionally follow this procedure as well. Five milliliters of isosulfan blue (Lymphazurin; Covidien) are also routinely injected before surgical incision for visual localization of the sentinel nodes. Intraoperative audio localization of the sentinel node uses the C-Trak Automatic Analyzer system and the OmniProbe with collimator (Care Wise Medical Products Corp.).
Sentinel nodes are defined as hot and blue, hot but not blue, or not hot but blue. A hot sentinel node is defined a one having a count at least 10 times greater than the background count. The term hot is further defined as nodal tissue with more than 10% of the ex vivo count of the hottest sentinel node. The count value of each sentinel node itself is not routinely recorded otherwise. For this study, we based the sentinel lymph node identification rate on identification of at least one sentinel node in a patient who underwent sentinel node biopsy, and we obtained the pathologic T stage (pT) and pathologic N stage from the pathology record of the surgical specimen.
The statistical hypothesis was that the sentinel node identification rate with intraoperative injection (p1) would not be lower than the sentinel node identification rate with preoperative injection (p0). On the basis of clinical experience, the acceptable identification rate in patients with preoperative injection was set at 95% and a rate 85% or lower was considered unacceptably low. Therefore, the null hypothesis, H0, was p0 – p1 ≥ 10%, and the alternative hypothesis, H1, was p0 – p1 < 10%. With use of a 2-proportion z test, a minimum total of 118 patients with 59 in each group was deemed sufficient to gain 80% power at a type I error of 0.05. The Fisher exact test was used to compare the 2 injection groups in terms of binary demographic characters, the identification rate overall and by pT, and the rate of positive sentinel nodes overall, by pT, and by axillary dissection. The 2-sample t test was used to compare the number of sentinel nodes by pT and numeric demographic characters. A 2-sided type I error of 5% was used for each test to define statistical significance. Statistical analysis used Prism 5.0 (GraphPad Software Inc.). In addition, a biostatistician reviewed all statistical analyses.
RESULTS
We identified for analysis 904 sentinel node biopsies that were performed for breast cancer at VCUHS between January 1, 2005, and December 31, 2010. Of these, 35 were excluded because of incomplete information about the operation and cancer stage. A further 130 were excluded because the patients had received neoadjuvant chemotherapy before the sentinel node biopsy. The remaining 739 sentinel node biopsies were included in this analysis, with 647 having received preoperative injection of radiocolloid for localization and 92 having received intraoperative injection. The average age of the study population was 56.8 y: 57.1 y in the preoperative injection group and 53.4 y in the intraoperative injection group. As expected, most patients were women (733 of the 739 biopsies). There were more Caucasian patients in the preoperative group (60.0% vs. 34.8%) and fewer African-Americans (37.9% vs. 62.0%); the difference in ethnicity was statistically significant in both study groups (P < 0.0001). There were also more T1 tumors in the preoperative injection group (65.5% vs. 51.1%; P = 0.0104) and fewer T2 tumors (22.1% vs. 32.6%; P = 0.0345). When the T1 tumors were subdivided into Tm, T1a, T1b, and T1c, only the T1c distribution was statistically different (36.5% vs. 21.7%; P = 0.0049); there were more T1c tumors in the preoperative injection group (Table 1).
Patient Demographics
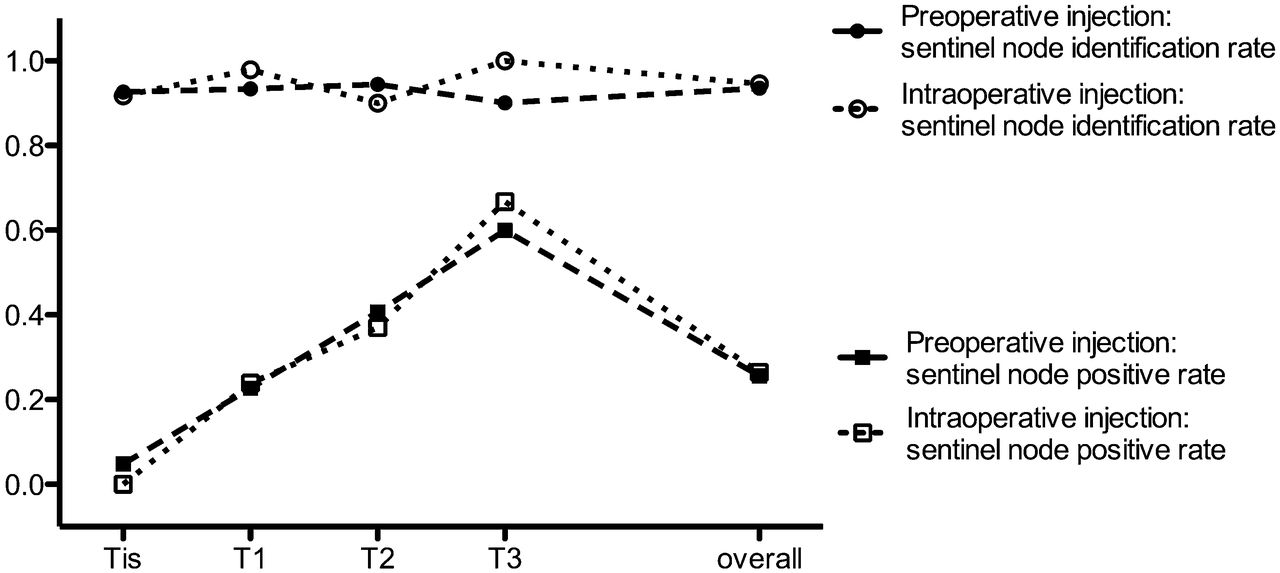
The overall sentinel lymph node identification rates were comparable in the 2 groups (Fig. 1), 93.5% for the preoperative injection group and 94.6% for the intraoperative injection group (not statistically significant). When analyzed by ethnicity, the identification rate of sentinel nodes in African-American women (92.7% and 91.2%) and Caucasian women (94.1% and 100%) did not significantly differ between the preoperative and intraoperative injection groups. The identification rate remained equivalent for both groups when analyzed by the pT of the tumor: 92.6% vs. 91.7% for Tis, 93.4% vs. 97.9% for T1, and 94.4% vs. 90.0% for T2 in the preoperative group vs. the intraoperative group. Similarly, the average number of sentinel lymph nodes removed did not differ between the preoperative and the intraoperative groups: 2.60 nodes versus 2.70 nodes overall, 2.22 nodes versus 2.91 for Tis, 2.66 nodes versus 2.89 for T1, and 2.62 nodes versus 2.30 for T2 (Table 2).

Sentinel node biopsy: preoperative vs. intraoperative injection.
Sentinel Node Identification
The overall rates of positive sentinel nodes were comparable in the 2 groups (Fig. 1), 25.6% for the preoperative injection group and 26.4% for the intraoperative injection group (not statistically significant). There was also no difference in the rate of biopsies positive for a sentinel node in African-American women (21.3% and 28.1%, respectively) or Caucasian women (25.8% and 18.8%, respectively) between the preoperative and intraoperative injection groups. When analyzed by pT, the positivity rate remained similar: for T1 tumors, 22.7% in the preoperative group versus 23.9% in the intraoperative group; for T2 tumors, 40.7% versus 37.0%, respectively (Table 3).
Sentinel Node Malignancy Rate
In the preoperative injection group, 42 patients had no sentinel node identified, 39 of whom went on to axillary dissection. Of these 39, 12 were found to have nodal metastasis, for a positive axilla rate of 30.8% on dissection. In the intraoperative injection group, all 5 patients in whom no sentinel node was found went on to axillary dissection. Of these 5, 3 had axillary nodal metastasis, for a positive axilla rate of 60.0% on dissection. These differences are not statistically significant.
DISCUSSION
The ability to perform selective axillary dissection for breast cancer through axillary sentinel lymph node biopsy has transformed the surgical care of patients with breast cancer. As a result, the incidence of nontherapeutic axillary dissection and its morbid consequences has been reduced. Radiocolloid detection is considered by most breast surgeons to be essential for sentinel lymph node biopsy. When a handheld radiation probe is used intraoperatively, audio signaling facilitates the detection of the radioactive sentinel node in the axilla. The agent used, 99mTc-sulfur colloid, has an average diameter of about 0.2 μm; larger particles may be too large for lymphatic mapping. Only the axilla is explored for sentinel mapping in breast cancer, as axillary nodal staging remains an essential component in guiding breast cancer care. Although breast cancer can metastasize to the internal mammary nodes, the overall incidence is low and the instances of internal mammary node metastasis without axillary metastasis are even lower (1). Routine sampling of the internal mammary nodes has largely been abandoned.
The use of radiocolloid for operative identification of the sentinel node has, however, introduced a new morbidity: the pain associated with the preoperative retroareolar injection. Chandler et al. reported that in 35% of patients, the injection of radiocolloid was associated with significant pain, which occurred regardless of the use or timing of anesthetic cream (2). In a study of 39 patients randomized to treatment groups receiving topical lidocaine/prilocaine cream versus placebo before radiocolloid injection, the addition of local anesthesia failed to reduce the perceived pain associated with the injection (3). In a prospective randomized study of 140 patients, the addition of 1% lidocaine to the radiocolloid solution decreased the perceived pain but was associated with detection of fewer sentinel lymph nodes, even though the overall rate of sentinel node identification did not change (4). Radowsky also noted that providers tended to underestimate the level of pain the patients experienced when the patient reported the highest pain rating (5). Clearly, if the injection of radiocolloid can occur after the patient has been anesthetized in the operating room, the pain of radiocolloid injection will be eliminated.
The concern about intraoperative injection of radiocolloid is whether there would be sufficient time for the radiocolloid to travel from the injection site to the sentinel lymph nodes. Injection of radiocolloid the day of the biopsy appears to be equivalent to injection the day before, in terms of the false-negative sentinel node rate and the number of sentinel nodes identified (6). A study by Wondergem et al. of 117 patients who underwent radiocolloid injection and lymphoscintigraphy 1 and 2 h later suggests decreased sentinel lymph node localization at 1 h when compared with 2 h. At 1 h, lymphoscintigraphy localized a sentinel node in 79.5% of patients, with an increase to 95.7% at 2 h (7). However, localization by lymphoscintigraphy may not be as sensitive as that by operative exploration using a handheld probe and blue dye. Although lymphoscintigraphy can detect sentinel nodes outside the axilla, nonaxillary nodal activities would not be surgically relevant because only the axilla is explored at surgery.
Other surgical groups have reported their experience with intraoperative injection of radiocolloid for sentinel node biopsy. Layeeque et al., in performing 96 sentinel node biopsies using 39.6 MBq (1.07 mCi) of unfiltered 99mTc-sulfur colloid and blue dye injected intraoperatively into the retroareolar location, found a sentinel node localization rate of 97% (8). Zogakis et al., in performing 122 sentinel node biopsies using 37–74 MBq (1–2 mCi) of filtered 99mTc-sulfur colloid and isosulfan blue (also injected intraoperatively into the retroareolar location), had a 99.2% identification rate (9). Thompson et al. reported an identification rate of 96% for 252 patients with intraoperative injection of 4 mL of unfiltered 99mTc-sulfur colloid (37 MBq [1 mCi]) and isosulfan blue (10). Dauphine et al. prospectively randomized 100 patients into a preoperative injection group and 100 into an intraoperative injection group who received 5 mL of filtered 99mTc-sulfur colloid (18.5 MBq [0.5 mCi]) and blue dye. The 2 groups had equivalent sentinel lymph node identification rates: 96% for preoperative injection and 100% for intraoperative injection (11). Dixon et al. reported a similar identification rate of 98% for 163 sentinel node biopsies using 0.5 mL of 99mTc sulfur colloid (25 MBq [0.68 mCi]) and blue dye intraoperatively injected into the retroareolar location (12). Johnson et al. expanded an experiment of Layeeque et al. (8) to include 775 sentinel node biopsies with 37 MBq (1 mCi) of 99mTc sulfur colloid, mostly without blue dye. The sentinel node identification rate remained excellent at 98.6% (13). The VCUHS study has found equivalent sentinel lymph node identification rates for both groups, 93.5% for preoperative injection and 94.6% for intraoperative injection. The rate of sentinel lymph node identification with intraoperative injection at VCUHS appears similar to that of the previously mentioned publications (96%–100%).
Despite the acceptable sentinel node identification rate, there naturally remain concerns that the identified node may not represent the oncologic sentinel lymph node. Without all patients undergoing axillary dissection, the true false-negative sentinel node biopsy rate cannot be determined. However, an analysis of the positive sentinel node biopsy rate with published pTs suggests comparability between the 2 techniques. Stell et al. compared the incidence of positive sentinel lymph nodes between 102 patients with preoperative injection of radiocolloid and that of 112 patients with intraoperative injection. The 2 groups had equivalent tumor characteristics and incidence of positive sentinel lymph nodes, 20.6% for preoperative injection versus 19.6% for intraoperative injection (14). The VCUHS study also shows no statistical difference in the overall positive sentinel node biopsy rate between preoperative injection (25.6%) and intraoperative injection (26.4%). This study, however, has fewer T1 and more T2 tumors in the intraoperative injection group (51.1% are T1 and 32.6% are T2) than in the preoperative injection group (65.5% are T1 and 22.1% are T2). The study of Stell et al. did not break the patient population into ethnic groups but did have an equivalent distribution of tumor stage. When analyzed by pTs, the sentinel node positive rate did not differ between the intraoperative and preoperative injection groups for T1 (23.9% vs. 22.7%) or for T2 (37.0% vs. 40.7%). In addition, the 23.9% positive sentinel node biopsy rate for T1 and 37.0% for T2 with intraoperative injection in the VCUHS series are comparable to those of other intraoperative injection series. Zogakis et al. reported 16.8% positive sentinel node biopsies for T1 and 44% for T2 (9). The series of Thompson et al. had an 11% positive sentinel node biopsy rate for T1 and 25% for T2 (10). The positivity rate of the VCUHS experience with intraoperative injection of T2 tumors falls neatly between those of Zogakis and Thompson, and the positivity rate of T1 tumors exceeds both, thus decreasing the chances of a false-negative sentinel node biopsy.
Because the study was not prospective and randomized, there are several limitations. First, the 2 study groups may not be comparable because they differed demographically. How the difference in ethnicity might affect the outcome remains unclear, but once the findings were stratified by ethnicity, there did not appear to be any difference in sentinel node identification or positive sentinel nodes. Second, there was no standardization of injection site for sentinel node biopsy; according to the surgeon’s preference, some patients underwent peritumoral or intradermal injection as well as retroareolar injection. Randomized studies, however, have endorsed the retroareolar injection site, used in all studied patients, as reliable (15–18). Because the injection site has not appeared to affect sentinel node identification in the literature, differences in injection site may not be significant. Third, the time from radiocolloid injection to surgical incision was not quantified for any of the studied patients. Empirically, there is about an hour from injection to incision for the preoperative group and 15 min for the intraoperative group. Finally, there was no true-negative control for analysis, leaving the possibility that despite equivalence of observed sentinel node identification rate, the true sentinel node identification rate might be different. Tumor stage–matched analysis of positive sentinel node biopsy, which appears comparable between the 2 groups, was used instead. Despite the limitations of this study, the findings do support those of other published studies endorsing equivalence between intraoperative and preoperative injection of radiocolloid for sentinel node biopsy in breast cancer.
CONCLUSION
Intraoperative injection of radiocolloid appears to produce an acceptable sentinel node biopsy identification rate, compared with that of preoperative injection. The main benefit is the reduction of discomfort, as the injection of radiocolloid occurs under operative anesthesia. An additional benefit is a 1-step process, as the patient would present for a combined sentinel node injection, sentinel node mapping, sentinel node biopsy, and breast surgical therapy. Currently, many surgical practices for breast cancer arrange for sentinel node radiocolloid injection the day before the operation to facilitate morning sentinel node biopsy and to minimize any delays in the start of surgery. Intraoperative injection would still require that the radiocolloid be available for injection the morning of the operation. The implementation of intraoperative injection requires a partnership among the department of surgery, the department of nuclear medicine, and the operating room services to maintain radiation safety standards.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Jenni Brumelle, PhD, for her scientific review of the manuscript.
Footnotes
Published online Nov. 14, 2013.
REFERENCES
- Received for publication July 16, 2013.
- Accepted for publication October 17, 2013.





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.