


Abstract
The purpose of this paper is to briefly explain report 160 of the National Council on Radiation Protection and Measurement and the significance of the report to medical imaging as a whole and nuclear medicine specifically. The implications of the findings of report 160 have had repercussions and will continue to affect all of ionizing radiation medical imaging. The nuclear medicine community should have an understanding of why and how report 160 is important. After reading this article, the nuclear medicine technologist will be familiar with the main focus of report 160, the significant change that has occurred since the 1980s in the ionizing radiation exposure of people in the United States, the primary background source of ionizing radiation in the United States, the primary medical exposure to ionizing radiation in the United States, trends in nuclear medicine procedures and patient exposure, and a comparison of population doses between 2006 and the early 1980s as outlined in report 160.
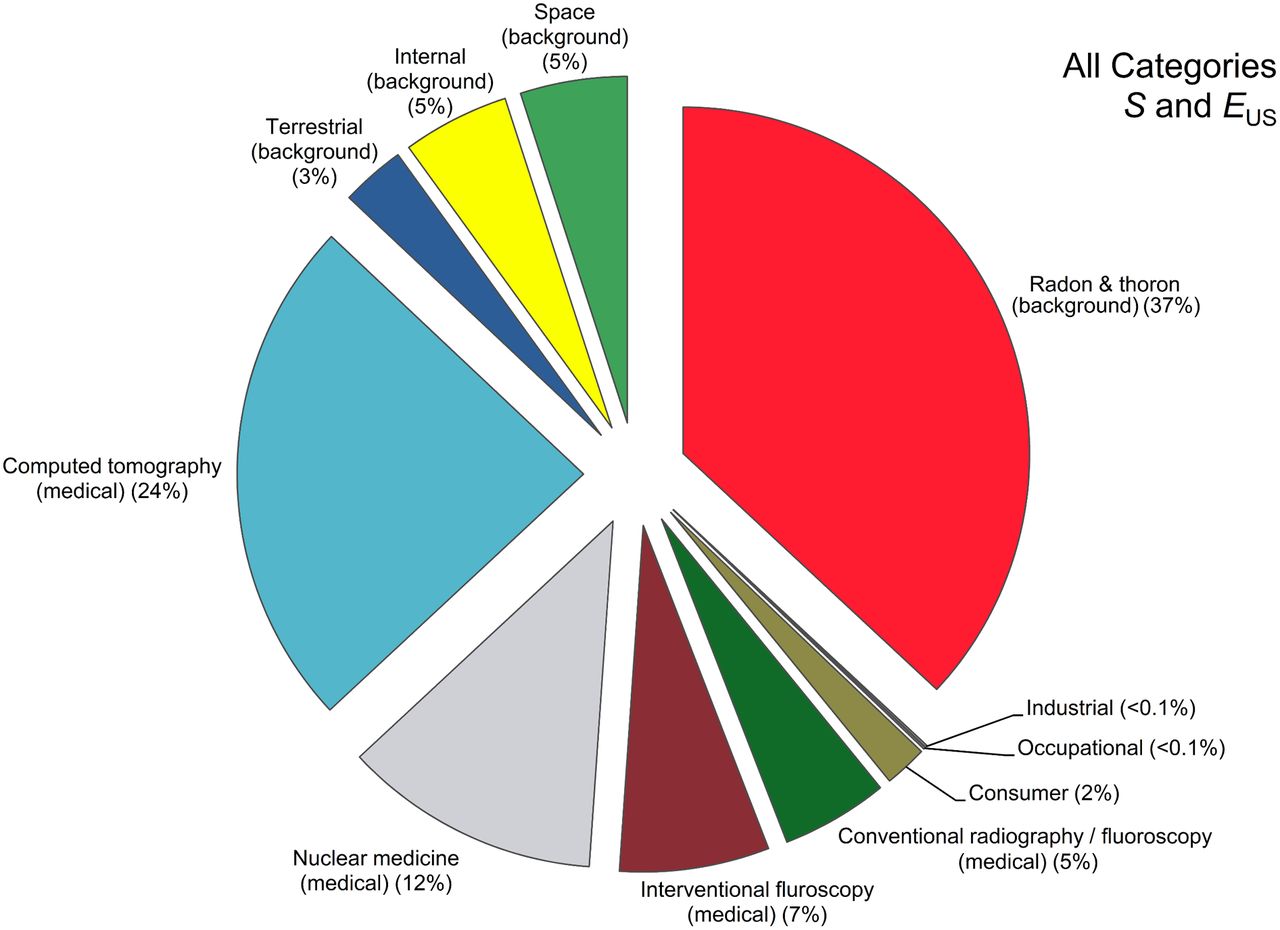
The National Council on Radiation Protection and Measurements (NCRP) periodically produces reports as recommendations to the general public on specific topics. Report 160, released in March 2009, is entitled “Ionizing Radiation Exposure of the Population of the United States” (1). This was an update of report 93, which was on the same topic and was released in 1987. Report 160 followed the 2006 release of another report, Health Risks from Exposure to Low Levels of Ionizing Radiation: BEIR VII Phase 2 (2), by the National Research Councils’ Committee to Assess Health Risks from Exposure to Low Levels of Ionizing Radiation. BEIR VII, an update of 1990’s BEIR V, concluded that ionizing radiation damage can never be determined to be 100% repairable in human DNA and thus reaffirmed the linear nonthreshold dose response for ionizing radiation, classifying it as a human xenobiotic. The linear nonthreshold dose-response model states that no matter how small the dose received, the maximum response is always possible. As pertains to ionizing radiation effects in humans, this model would mean that cancer induction is a chronic effect and that death is the worst possible response. The importance of report 160 was its focus on the dramatic increase in radiation exposure in the United States between the 1980s data of report 93 and the 2006 BEIR VII data of report 160. The expected average radiation exposure in the United States was around 3.6 mSv (360 mrem) in the 1980s but jumped to 6.2 mSv (620 mrem) in 2006 (3). The entire report focused on what caused this increase (Fig. 1; Table 1).

Chart showing effective dose to U.S. population in 2006 from all categories. S = person-Sv; EUS = effective dose per individual in United States. (Reprinted with permission of (1).)
Basis for Person-Sv (S) and Effective Dose per Individual in United States (EUS) in 2006, with Medical Exposure Being 3 mSv
CHANGE IN IONIZING RADIATION EXPOSURE TO U.S. POPULATION SINCE 1980S
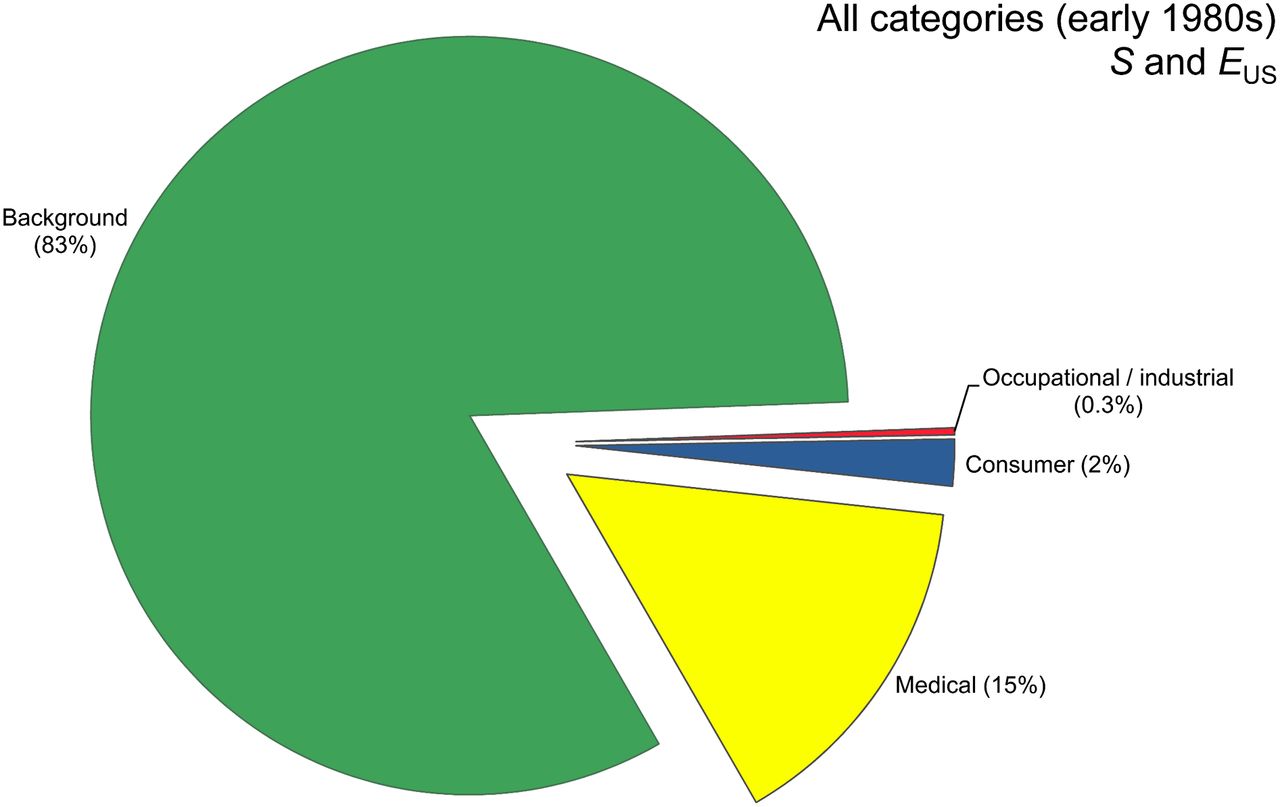
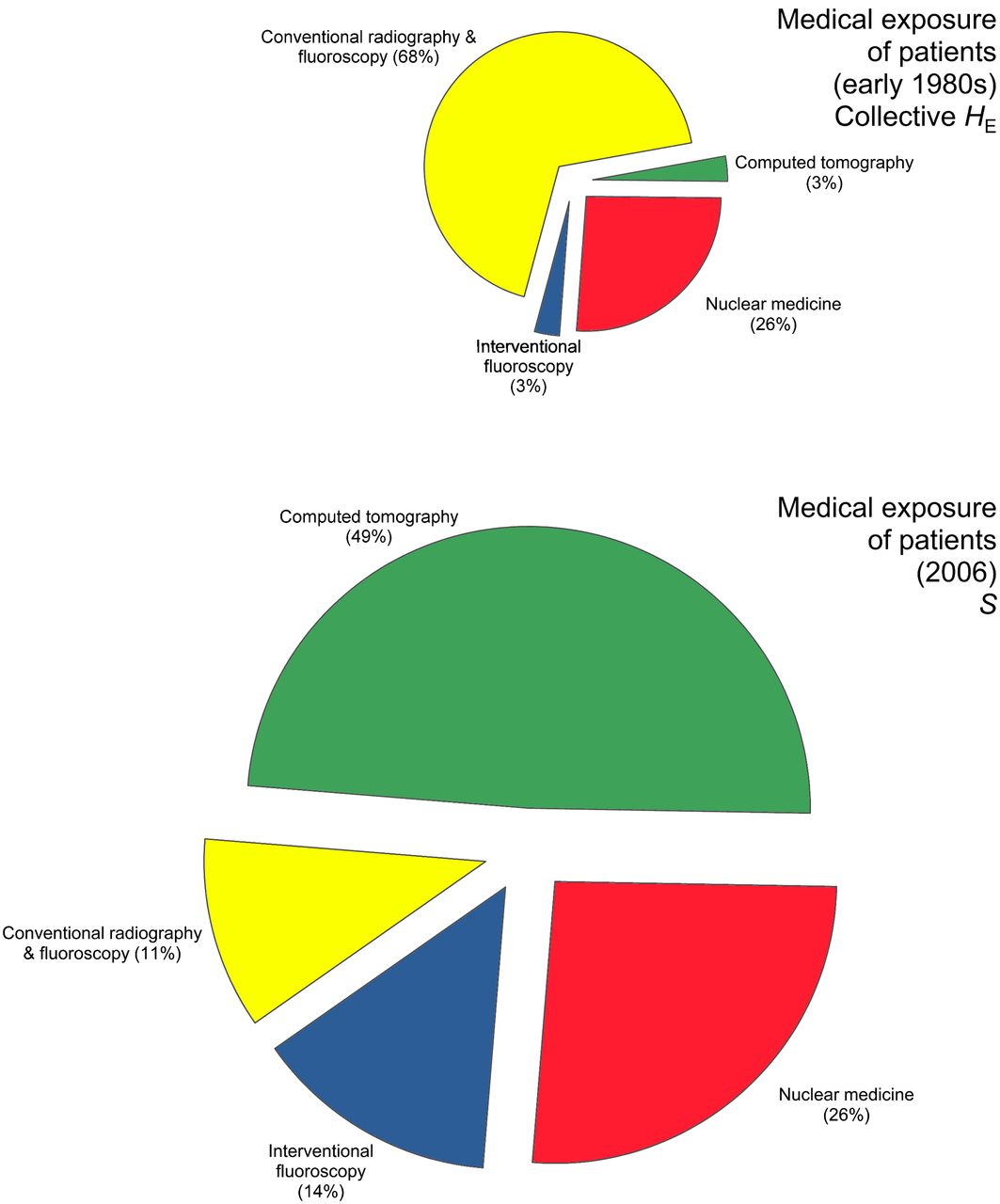
Although report 160 was released in 2009, most of the data were actually from 2006. The findings indicate that the only significant change in ionizing radiation exposure in the United States was an increase in medical exposure to the average U.S. citizen. Other categories—including radon in homes; consumer products; industrial, security, educational, and research sources; and occupational exposure—did not increase significantly. Therefore, medical exposure accounted for most of the approximately 72% increase in ionizing radiation exposure (2.6 mSv [260 mrem]) between the two reports. This increase has raised and continues to raise concerns from the general public and the scientific community about reducing exposure to ionizing radiation during medical procedures. Medical exposure went from 15% of all exposure in the 1980s to 48% of all exposure in 2006 (Fig. 2) (1,2).
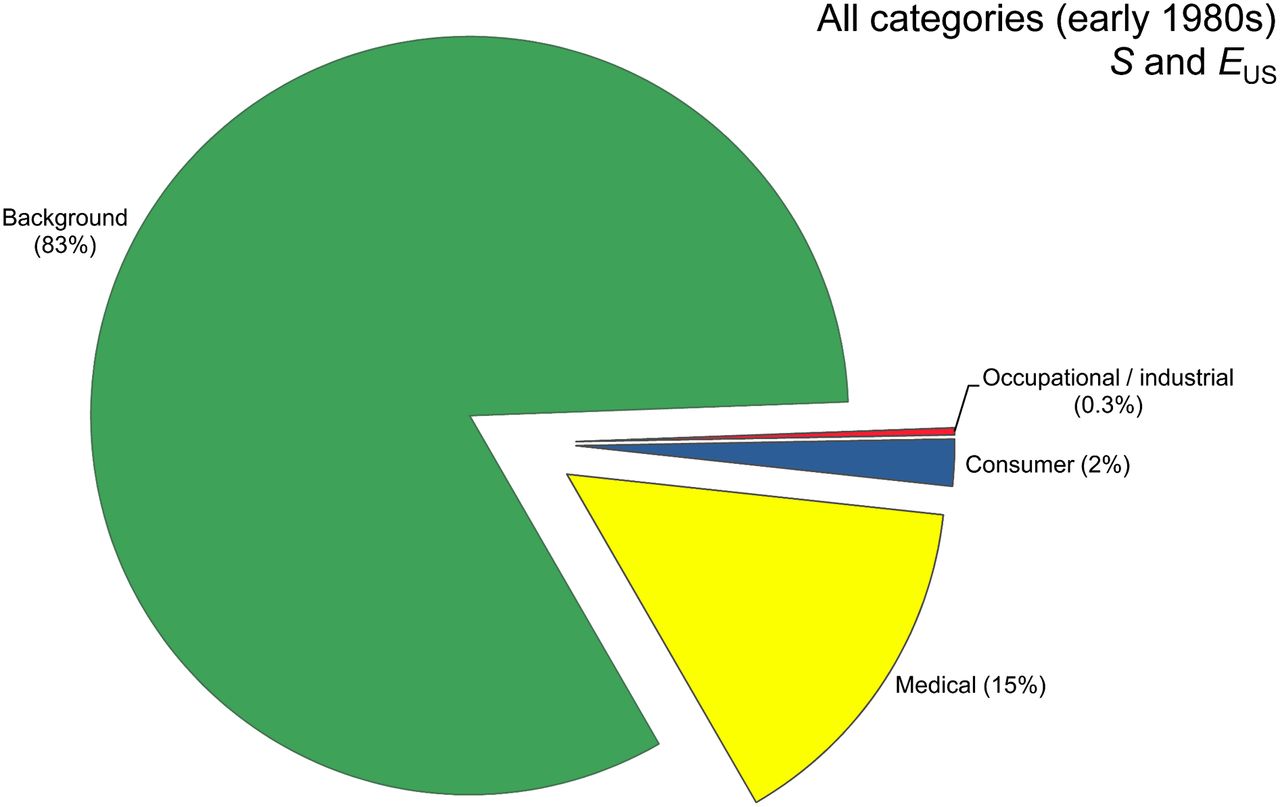
Chart showing exposure of U.S. population in early 1980s. When compared with these data, data from 2006 showed marked increase in medical exposure from 15% to 48%. S = person-Sv; EUS = effective dose per individual in United States. (Reprinted with permission of (1).)
PRIMARY BACKGROUND SOURCE OF IONIZING RADIATION IN UNITED STATES
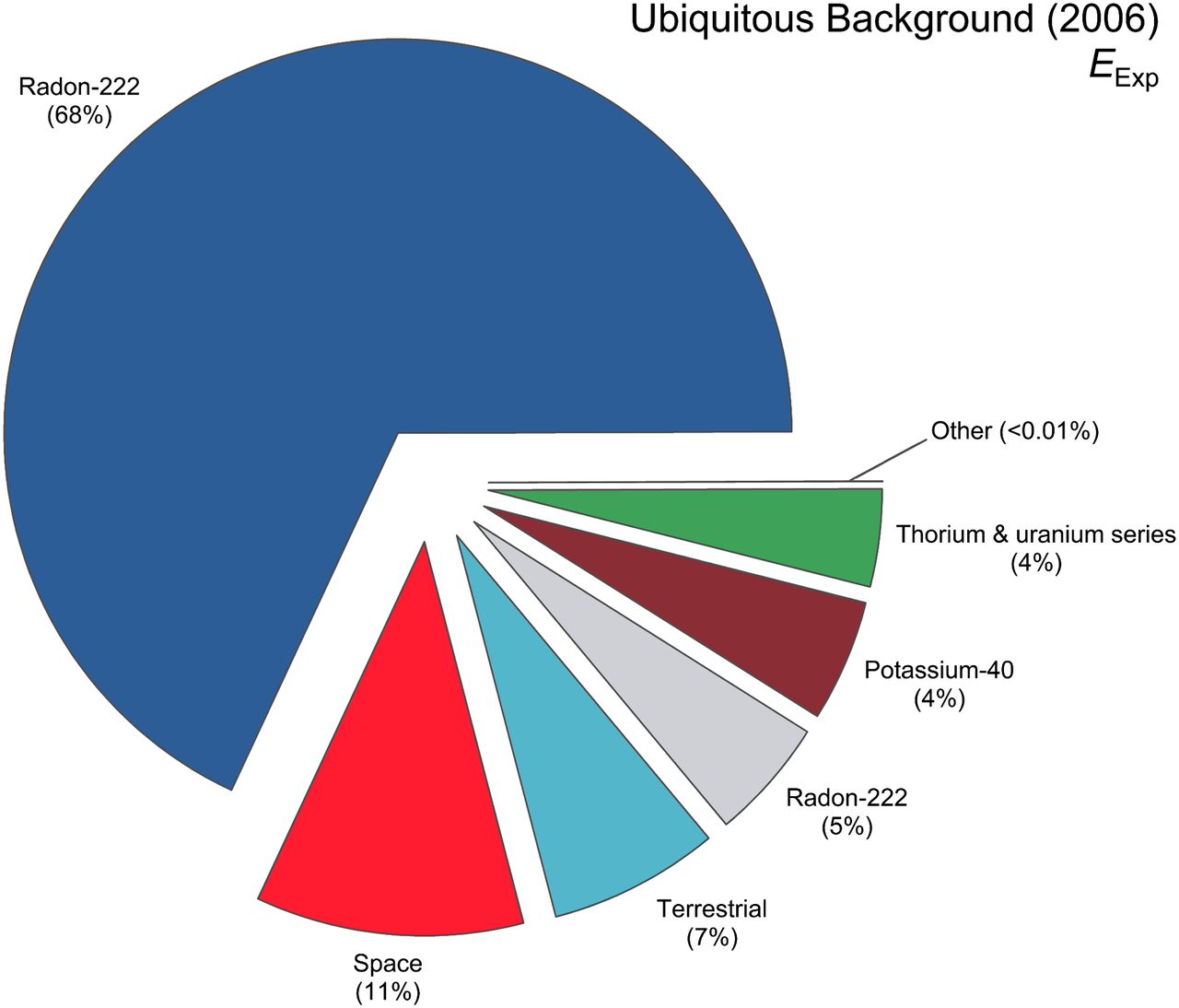
The primary background source of ionizing radiation in the United States is radon in homes, accounting for approximately 68% of exposure. The U.S. Environmental Protection Agency indicates that radon is the second most frequent cause of lung cancer after cigarette smoking, causing an estimated 21,000 lung cancer deaths per year in the United States. Radionuclides in the body account for approximately 14% of background ionizing radiation. Radioisotopes such as 40K and 210Po are examples. Any radioactive isotopes in the soil that are incorporated into the food chain can end up in the human body. Cosmic rays from space account for approximately 11% of background ionizing radiation. These can include cosmic ray bursts from the sun that are not filtered out by the earth’s magnetic field. Terrestrial sources account for approximately 7% of background ionizing radiation and can include building materials such as marble, granite, and bricks that have radioactive trace components naturally incorporated into them from mother earth.
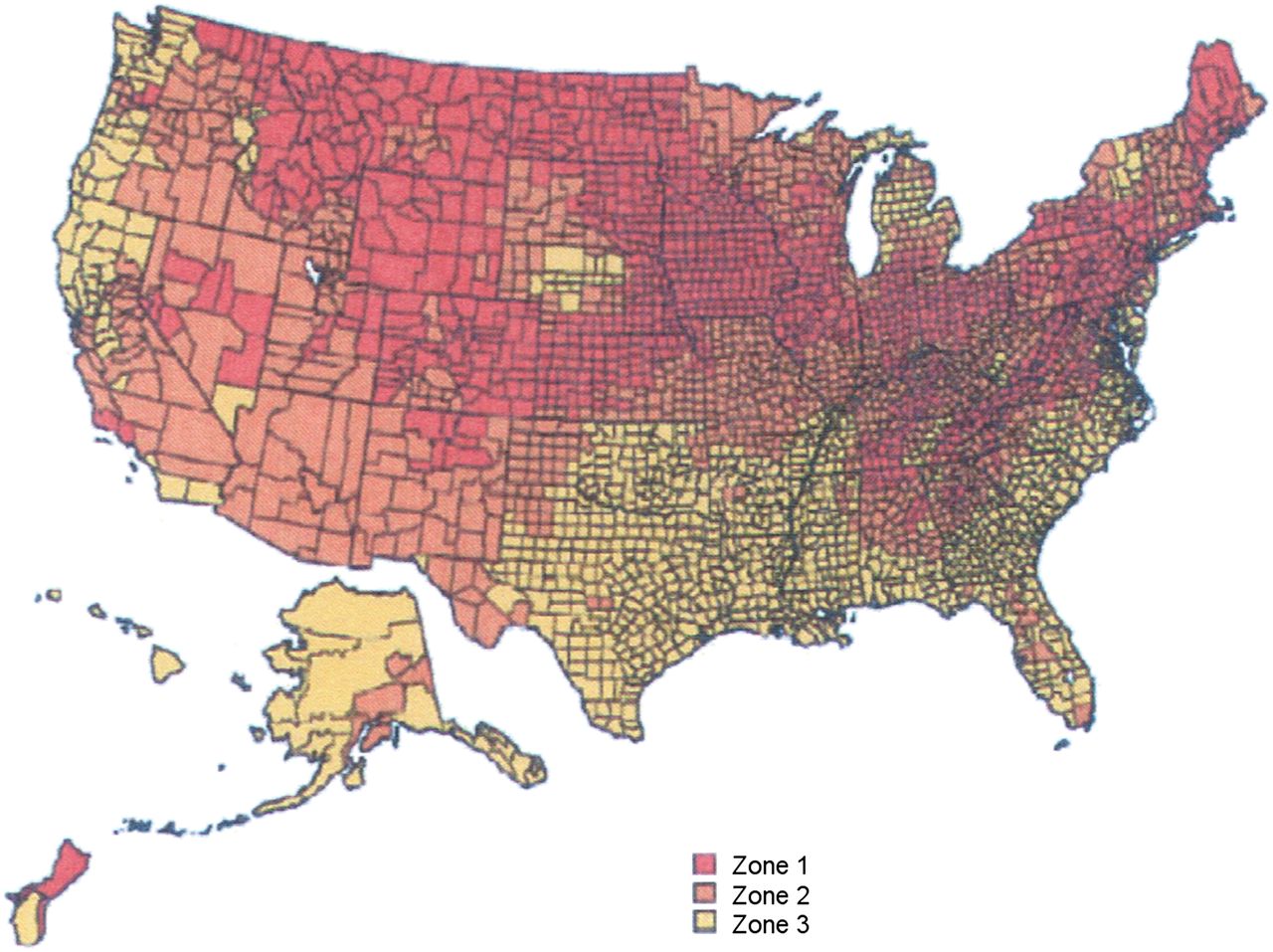
Radon is by far the greatest contributor of background ionizing radiation, with the amount greatly varying with local terrain. An example is given in Figure 3 (NCRP 160 Figure 3.14) from the Environmental Protection Agency, but generally, a hilly or mountainous terrain is naturally more inclined to have a possibility of increased radon exposure. Homes should be checked to see if radon is seeping into the house through the foundation and building up within poorly ventilated areas. Even if a home is found to have high levels of radon, mitigating factors, such as proper ventilation, can reduce exposure to below the level of 0.148 Bq/L (4.0 pCi/L) of air suggested by the Environmental Protection Agency. One insidious way exposure can occur is through radon dissolved in water, which can come through pipes from a distant source and be inhaled in the vapors that form during showering or bathing. All homes should be checked for radon using commercially available kits from local home building supply stores (Figs. 3–5) (1,4).

Overall contribution from different sources of background radiation to U.S. population. EExp = average effective dose for the exposed group for 2006. (Reprinted with permission of (1).)
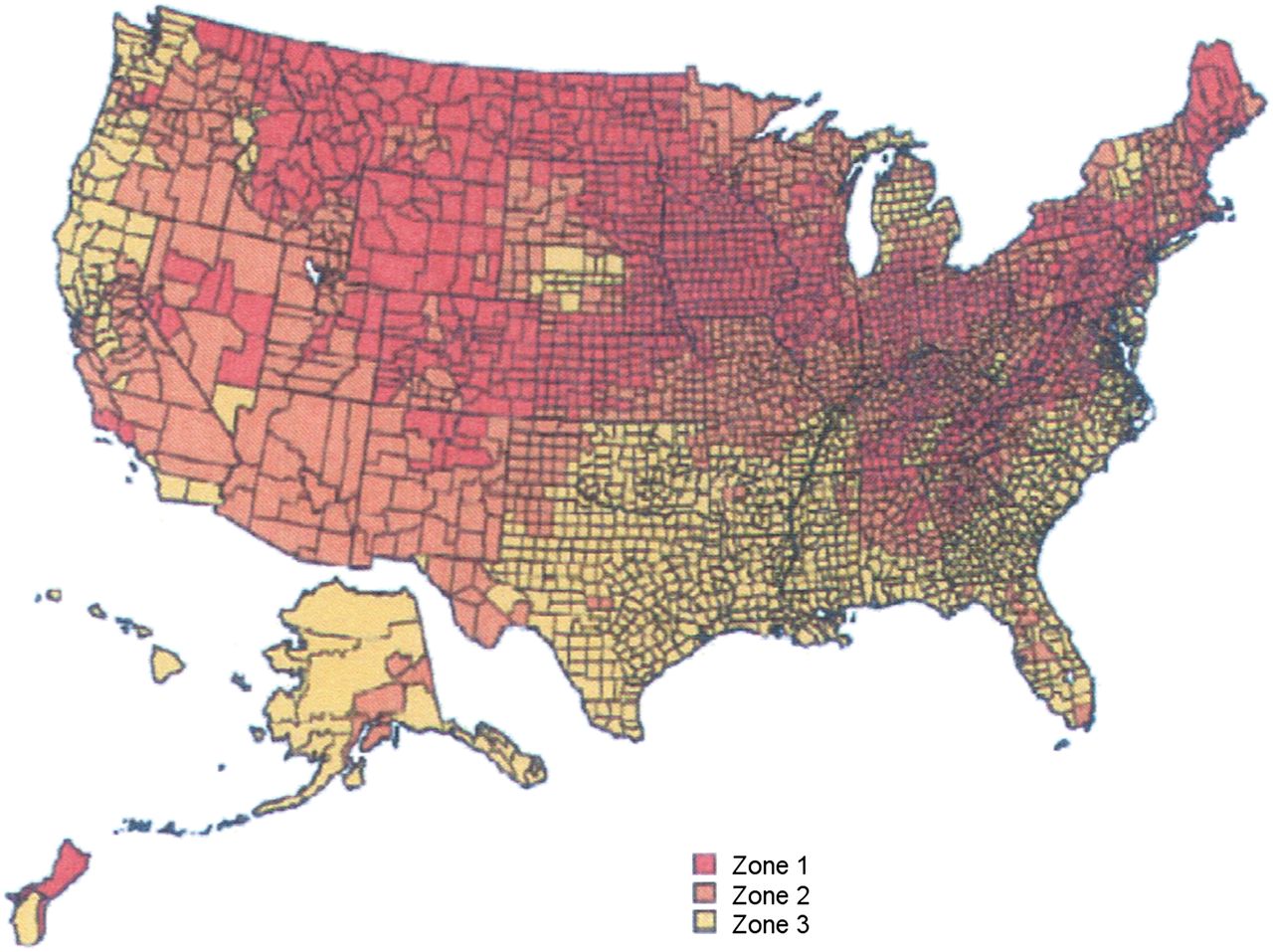
Relative radon amounts by county in United States. Red counties are >148 Bq m−3; orange counties are 74–148 Bq m−3; yellow counties are <74 Bq m−3. (Reprinted with permission of (1).)
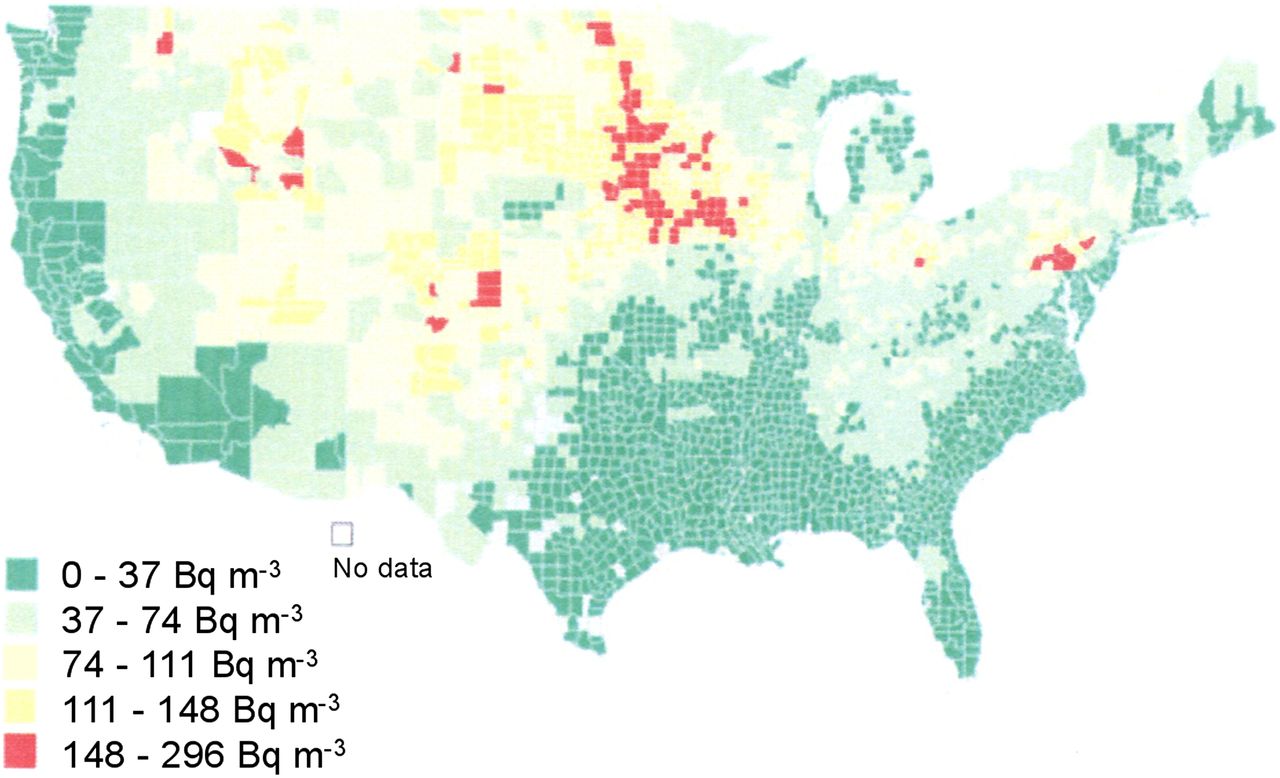
Radon concentrations predicted by Lawrence Berkley National Laboratory. Actual amounts per household depend on many factors, including ventilation. (Reprinted with permission of (1).)
PRIMARY SOURCE OF MEDICAL EXPOSURE TO IONIZING RADIATION IN UNITED STATES
Report 160 found that the biggest increase in exposure to ionizing radiation in U.S. citizens was from medical procedures. Specifically, CT was by far the greatest contributor, at 49% of all medical exposure. Nuclear medicine procedures came in second, accounting for 26% of all medical exposure. Interventional fluoroscopy accounting for 14%, and conventional radiography and fluoroscopy accounting for the remaining 11%. Exposure resulting from radiation therapy was not included in report 160 because such exposure was considered part of a treatment process. The number of CT procedures per year in the United States rose from 18.3 million in 1993 to 62 million in 2006—an approximately 239% increase. This large increase is due to several factors including better technology and throughput and diagnostic reliability. The ever-increasing slice thicknesses—from 16 to 32 to 64 to 128 and even greater—has given an ever-increasing resolution but has traditionally also meant an ever-increasing ionizing radiation dose to the patient. Concern about this exposure has led the public and the scientific community to take CT dose reduction techniques seriously, finally resulting in the stabilization of slice thickness increases seen a few years ago (Table 2; Fig. 6) (5,6).
Estimated CT Dose Contribution per Scan Type with Estimated Effective Dose to Patients
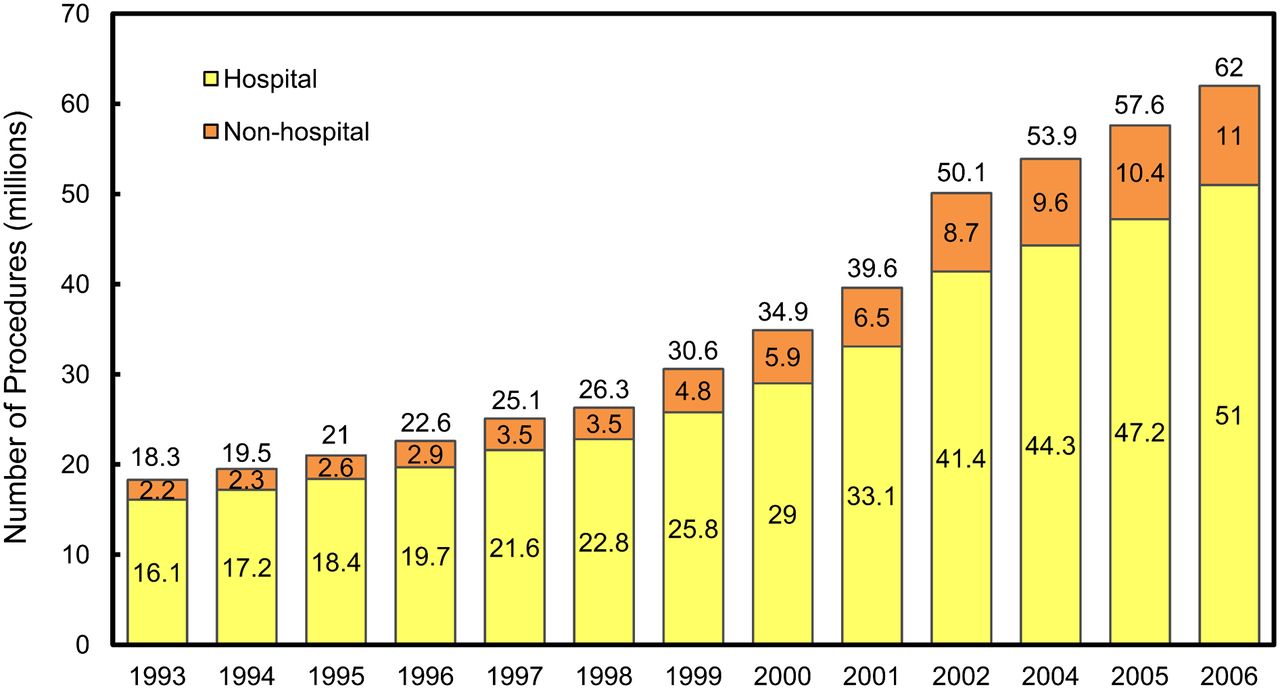
Number of CT procedures per year in United States from 1993 to 2006. (Reprinted with permission of (1).)
TRENDS IN NUCLEAR MEDICINE PROCEDURES AND PATIENT EXPOSURE
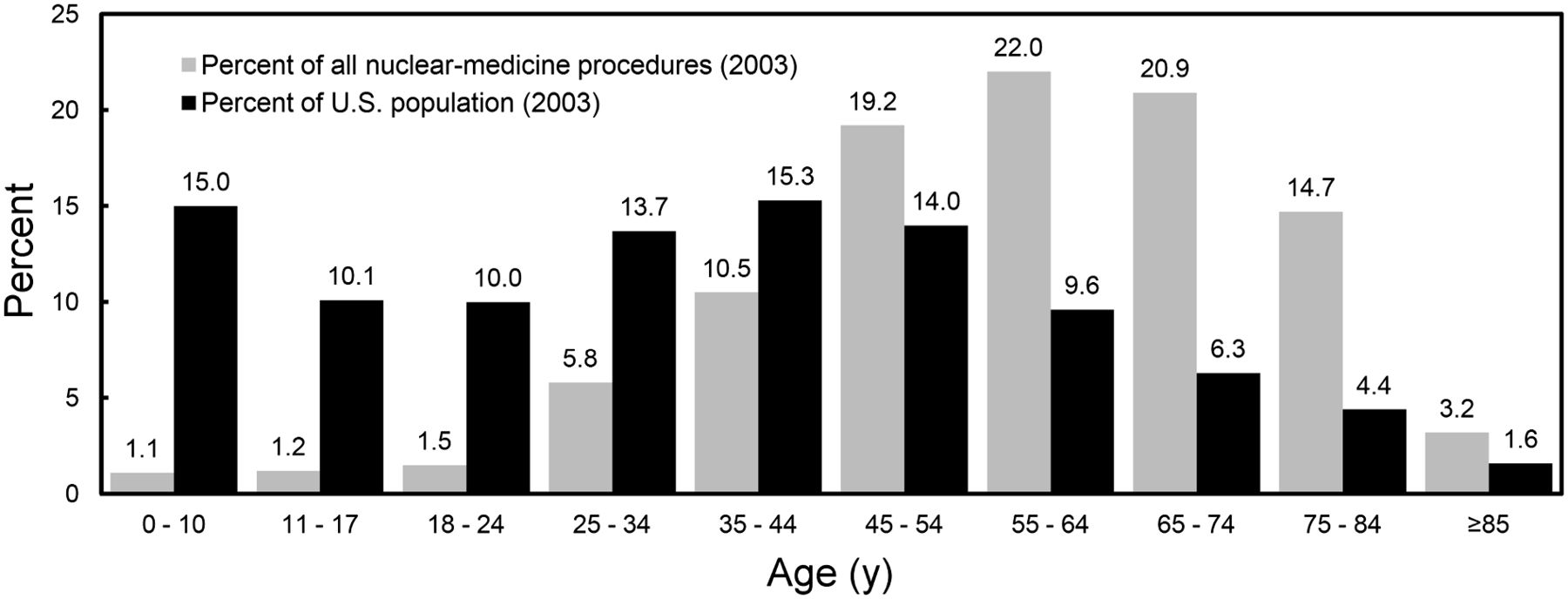
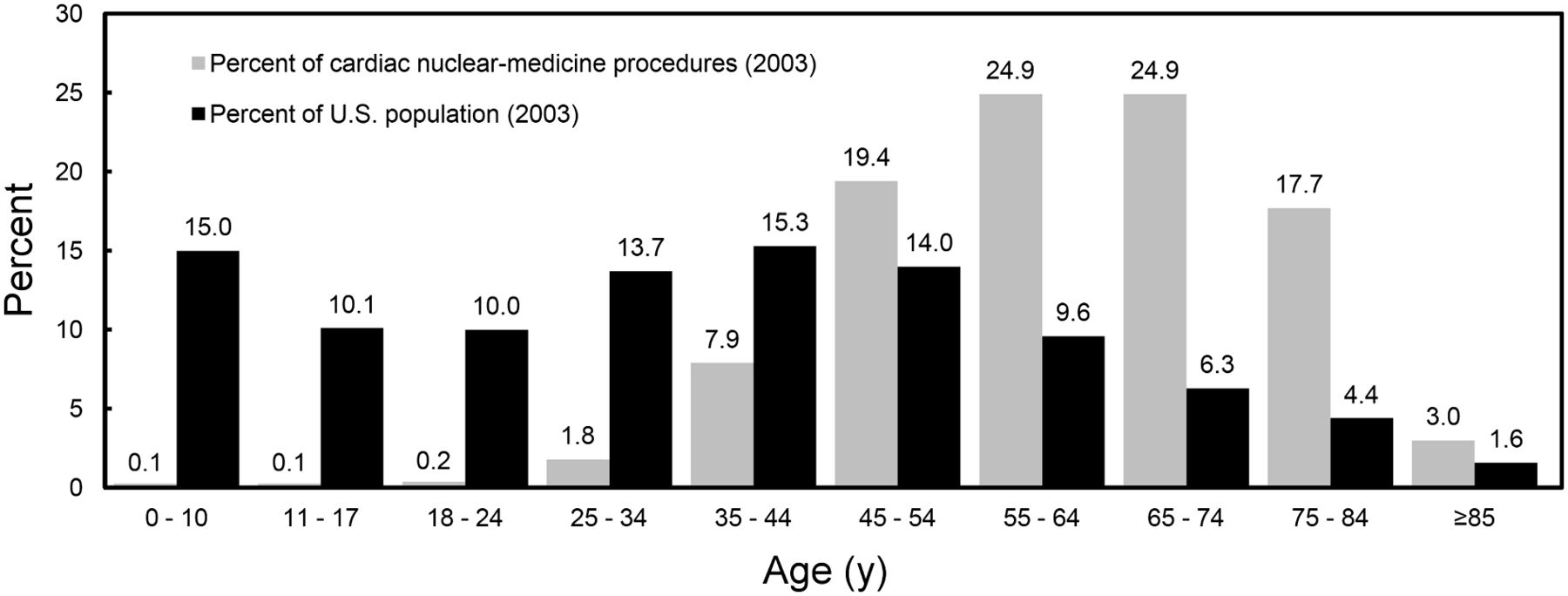
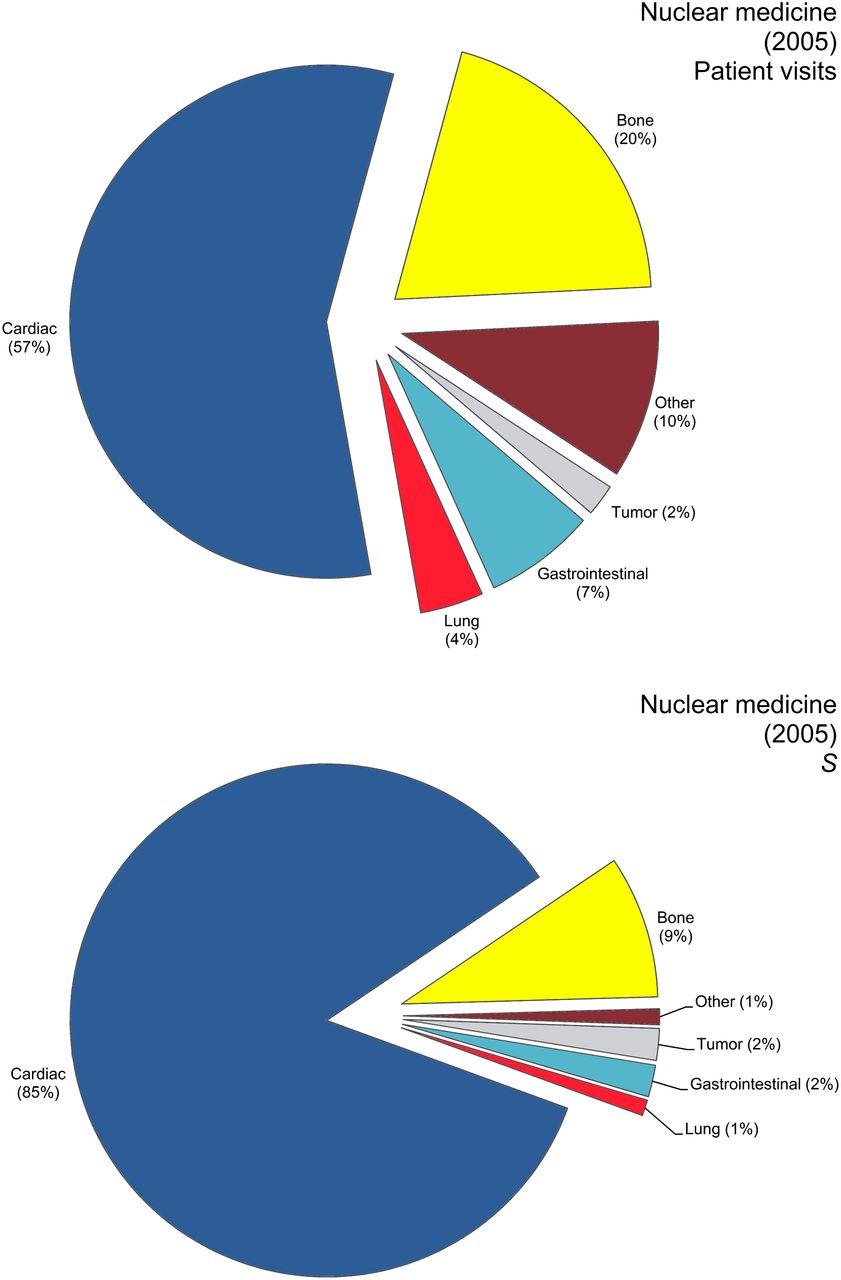
How did the annual number of nuclear medicine procedure in the United States change between the 1970s and 2006? How did the characteristics and age distribution of patients change during that time? How did the approximate effective dose estimates of nuclear medicine procedures change? Report 160 addressed all these questions. In comparing data from 1972 and 2006, the report revealed that there were 15.7 nuclear medicine examinations or visits per 1,000 people in 1972 but 60.3 million in 2006, an approximately 284% increase. The annual number of nuclear medicine procedures during that time increased from about 3.3 million to 18.1 million, or approximately 448%. Report 160 also analyzed the types of nuclear medicine procedures that have been most common throughout the years. In the 1970s, the most common procedure was the brain scan. In the 1980s, a virtual tie was seen between bone scans and gastrointestinal procedures, with lung scans coming in third. In the early to mid 2000s, a nearly 2.5-fold increase in cardiac scans occurred, and the cardiac scan continues to be the most commonly performed nuclear medicine procedure. A distant second-place procedure is the bone scan, but cardiac scans are seen at a rate approximately 3 times greater than bone scans. Report 160 also analyzed the average age of patients having nuclear medicine procedures, specifically for 2003 and with regard to cardiac procedures alone and all nuclear medicine procedures together. For both cardiac procedures and all procedures, the largest group was the 55- to 64-y age group. In nuclear cardiology alone, the 65- to 74-y group was just as large as the 55- to 64-y group, and the 45- to 54-y group was smaller. However, for all nuclear medicine procedures together, the 65- to 74-y group was smaller than the 55- to 64-y group, followed by the 45- to 54-y group.
As far as effective dose estimates for nuclear medicine procedures are concerned, report 160 indicated that nuclear cardiology perfusion 99mTc-sestamibi/201Tl studies resulted in an effective dose per procedure of 17.7 mSv. The total collective effective dose for all nuclear medicine procedures in 2005 (the year analyzed by the NCRP 160 committee) was approximately 220,500 person-Sv. Nuclear cardiology procedures were 85.2% of this total (187,915 person-Sv for cardiac procedures [187,915/220,500 person-Sv × 100% = 85.2%]). Bone scans came in second, at 9.3%.
Concerns were expressed in report 160 about trends in medical imaging, including the use of CT scans for pulmonary imaging and an effective dose of about 5 mSv for a CT lung scan versus about 2.5 mSv for a nuclear medicine lung scan. In addition, PET/CT imaging was mentioned as possibly greatly increasing the effective dose to about 40 mSv per patient, depending on the type of imaging (e.g., diagnostic, scout, blank, or attenuation correction) (Figs. 7–10; Table 3) (7–12).
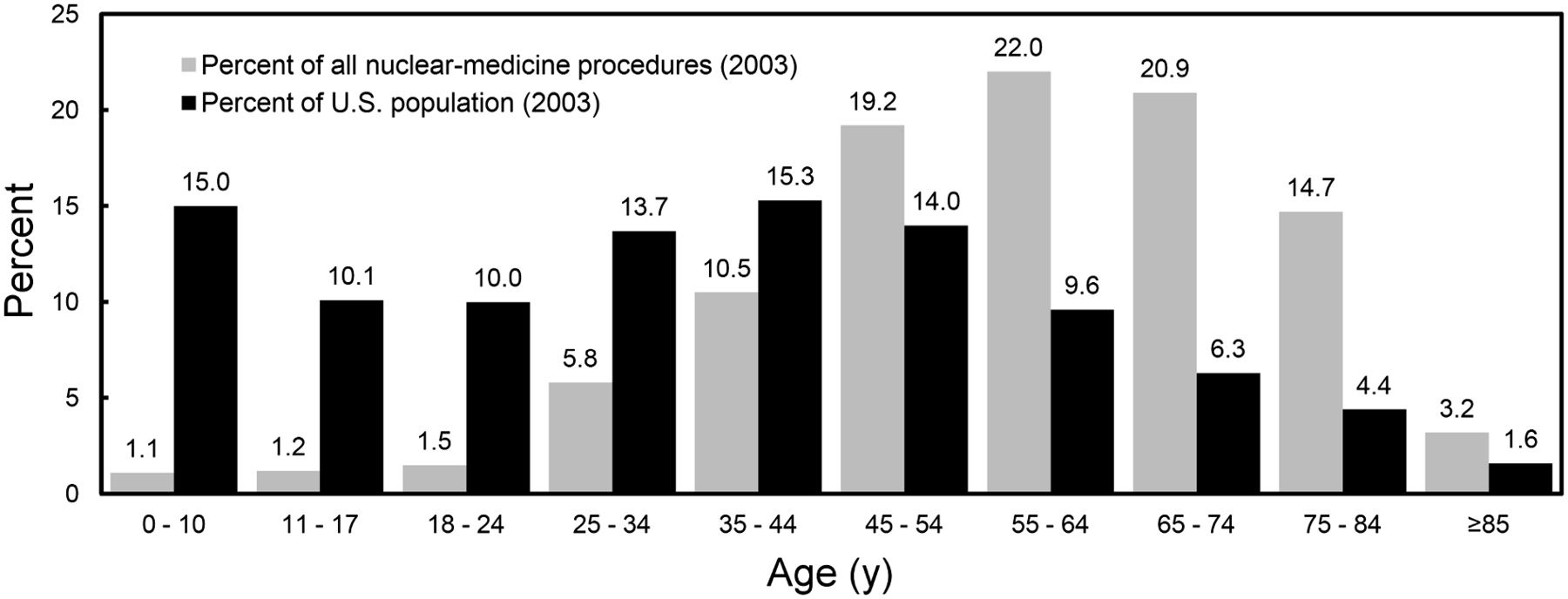
Age stratification of nuclear medicine examinations in 2003 snapshot showing that most patients were in 40- to 74-y age range. (Reprinted with permission of (1).)
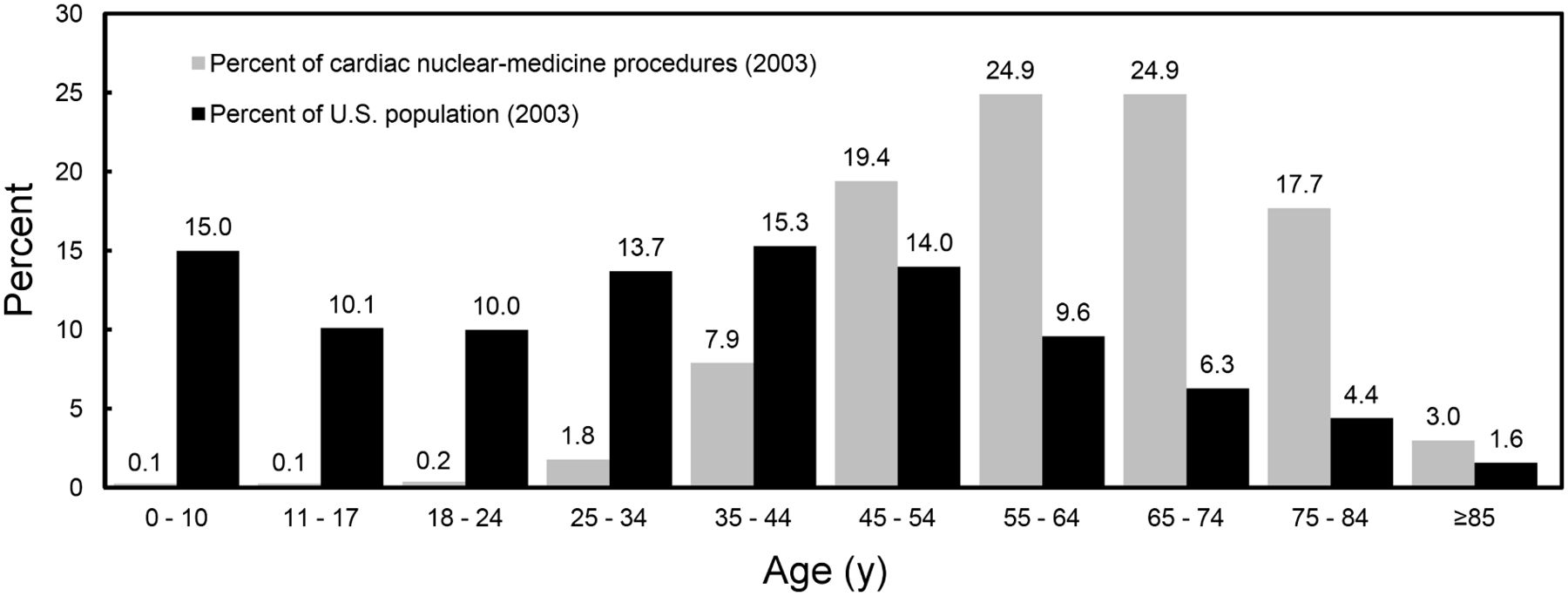
Age stratification of nuclear medicine cardiac examinations in 2003 snapshot showing that most patients were in 40- to 74-y age range. (Reprinted with permission of (1).)
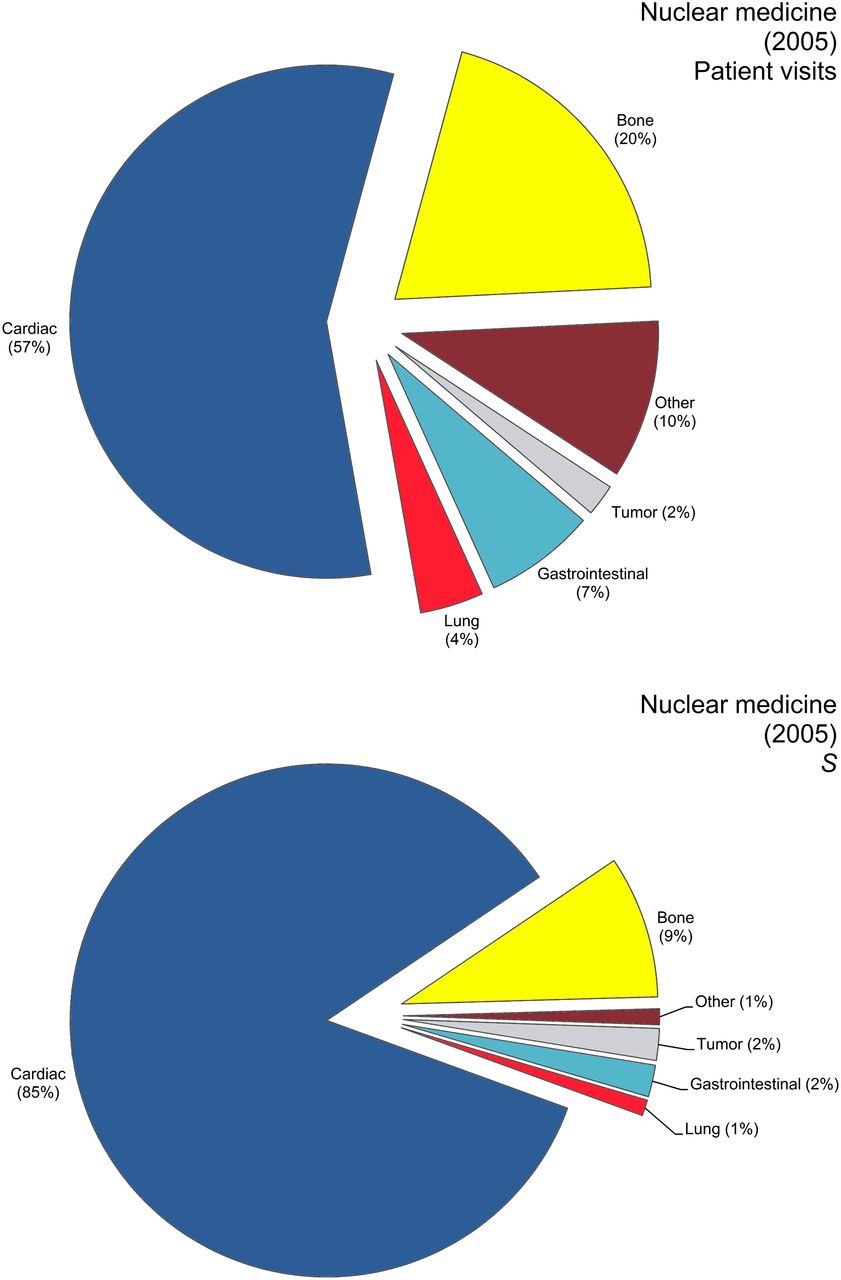
Charts of number of nuclear medicine patient visits and procedures in 2005 showing that most were for nuclear cardiology. S = person-Sv. (Reprinted with permission of (1).)

Comparison of medical procedures between early 1980s and 2006 showing marked increase in CT procedures from 3% to 49%. HE = effective dose equivalent; S = person-Sv. (Reprinted with permission of (1).)
Summary of Collective Effective Dose Estimates for Nuclear Medicine Procedures in 2005 Showing That Most Scans Were for Nuclear Cardiology
SUMMARY OF FINDINGS OF REPORT 160
In report 160, the main finding of importance for medical imaging using ionizing radiation is the dramatic increase in dose to the public between the 1980s and 2006. Essentially, although background exposure did not change, exposure of the general public to ionizing radiation increased some 33% solely because of the increase in medical imaging procedures. In the 1980s, medical procedures accounted for 15% of all exposure, whereas in 2006 they accounted for 48%. The increase was led primarily by increased use of CT imaging, followed by nuclear cardiology procedures. This finding has driven campaigns such as Image Gently and, more recently, Image Wisely, which advocate, respectively, reduction of ionizing imaging exposure in children and reduction of unnecessary imaging in adults. In addition, efforts have been made to optimize dose, improve technology, and thus reduce the exposure of patients during medical imaging procedures that use ionizing radiation. For example, PET/MR has the advantage of offering valuable diagnostic information while exposing the patient to a lower total dose than PET/CT or SPECT/CT (Fig. 11; Table 4) (7–12).
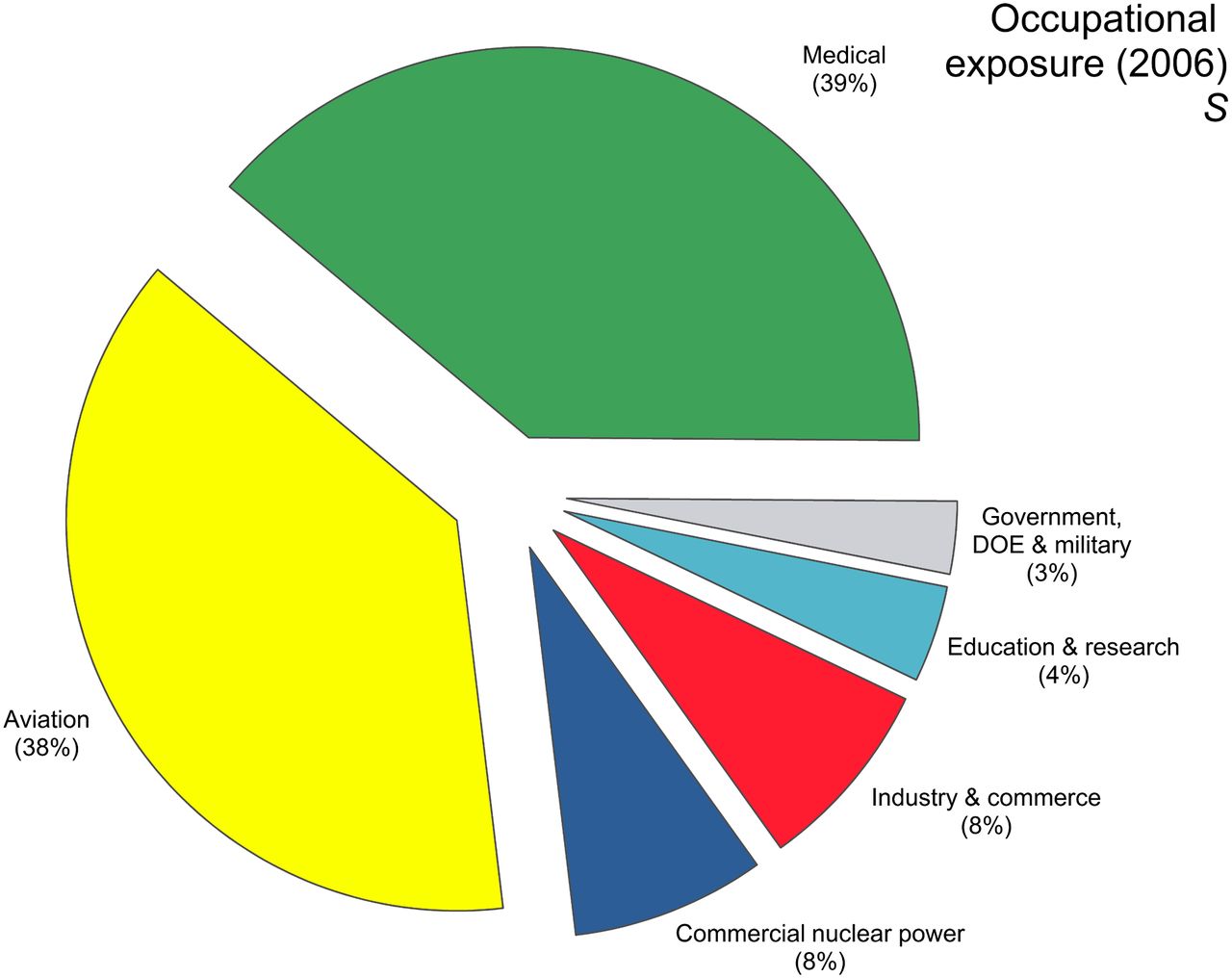
Chart showing contribution of medical exposure (39%) to occupationally exposed individuals. DOE = Department of Energy; S = person-Sv. (Reprinted with permission of (1).)
Collective U.S. Exposure (Dose) from Selected Modalities and Comparison Between Early 1980s and 2006
CONCLUSION
This brief look at NCRP report 160 has emphasized the fact that the average exposure of the general U.S. population to ionizing radiation increased from 3.6 mSv in the 1980s to 6.2 mSv in 2006. Although background rates of ionizing radiation have remained stable over this time, radon is still the primary agent of concern regarding background exposure. There has been a significant increase in exposure to ionizing radiation resulting from medical procedures—an increase led by CT, with nuclear cardiology coming in second. This finding has brought about efforts to optimize dose and decrease exposure during scans. Such exposure was beginning to become a possible issue, as cumulative exposure to patients from several procedures during a single hospital visit was beginning to affect the benefit-versus-risk balance of medical imaging. Efforts such as the formation of the Image Gently and Image Wisely campaigns continue to help curb the increase in ionizing radiation exposure from medical imaging.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Guest Editor: Danny A. Basso, University Hospital, Augusta, Georgia
↵* NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNMMI WEB SITE (http://www.snmmi.org/ce_online) THROUGH DECEMBER 2015.
Published online Oct. 31, 2013.
REFERENCES
- Received for publication July 3, 2013.
- Accepted for publication September 16, 2013.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- CHANGE IN IONIZING RADIATION EXPOSURE TO U.S. POPULATION SINCE 1980S
- PRIMARY BACKGROUND SOURCE OF IONIZING RADIATION IN UNITED STATES
- PRIMARY SOURCE OF MEDICAL EXPOSURE TO IONIZING RADIATION IN UNITED STATES
- TRENDS IN NUCLEAR MEDICINE PROCEDURES AND PATIENT EXPOSURE
- SUMMARY OF FINDINGS OF REPORT 160
- CONCLUSION
- DISCLOSURE
- Footnotes
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- Patient Shielding in Radiography
- Development of Simple Methods to Reduce the Exposure of the Public to Radiation from Patients Who Have Undergone 18F-FDG PET/CT
- Anthropomorphic left ventricular mesh phantom: a framework to investigate the accuracy of SQUEEZ using Coherent Point Drift for the detection of regional wall motion abnormalities
- Work history and radioprotection practices in relation to cancer incidence and mortality in US radiologic technologists performing nuclear medicine procedures
- Shielding in Medical Imaging and Radiation Therapy
- Randomized Controlled Trial of Radiation Protection With a Patient Lead Shield and a Novel, Nonlead Surgical Cap for Operators Performing Coronary Angiography or Intervention