


Abstract
Balancing image quality with radiation dose is a goal with every diagnostic procedure requiring radiation. Our institution compared the dosing of 99mTc-labeled succimer, commonly referred to as dimercaptosuccinic acid (99mTc-DMSA), to pediatric patients using 2 methods of calculation, body surface area (BSA, the method we used from 2009 to 2010) and body weight (BW, the method we used in 2011). Methods: A retrospective study was conducted in a 230-bed inpatient, tertiary-care academic pediatric hospital to obtain objective data on patients under the age of 17 y who received a renal nuclear medicine procedure with 99mTc-DMSA using a 300,000-count parallel image and four 150,000-count pinhole images. Data collection included patient age, sex, height, weight, calculated activity, assayed activity, administered activity, residual syringe activity, imaging time, and notable patient or equipment factors affecting the procedure. Results: Calculated activities based on BSA were higher than calculated activities based on BW. 99mTc-DMSA adsorption to the plastic syringes was significant, with a range of 3%–82%. Because of the adsorption, an average of 23.7 MBq (SD, ±31 MBq) was added to the patients’ calculated dose when the order was placed. Therefore, assayed activities were significantly higher than calculated activities in both groups. Administered activity correlations to BSA and BW calculations were 0.75 and 0.83, respectively. Administered activities from BSA and BW groups were outside the American College of Radiology (ACR)–recommended guidelines 59% and 45% of the time, respectively. Overall, children less than 2 y old were above the ACR recommendations 80% of the time. There was a poor correlation between administered activity and total imaging time (r = 0.23). Average imaging time overall for 5 planar views was 14.8 min (±7.1 min). Patients receiving less than the ACR-recommended administered activities (<1.85 MBq/kg) had an average increase in imaging time of 4.5 min (±3.4 min). Conclusion: The activity administered to patients was significantly affected by the amount of 99mTc-DMSA activity adsorbed to the syringe. Syringe residual should be considered when standardizing 99mTc-DMSA imaging protocols and calculating patient dose. Although 99mTc-DMSA adsorption was variable, the administered activities correlated with calculated activities. In all but one of our patients, the total imaging time was far less than recommended by the ACR and European Association of Nuclear Medicine guidelines. The study indicates that using the BW calculation of 3.7 MBq/kg resulted in a range of administered activity of 1.85–2.59 MBq/kg. 99mTc-DMSA dosing of 3.7 MBq/kg for pinhole imaging should be appropriate for most studies.
Many variables such as circulation time, metabolic processes, body weight (BW), and size must be considered when determining the activity of a radiopharmaceutical (dose) to be administered to pediatric patients in nuclear medicine (1). Children have a much greater risk of experiencing undesirable health effects from exposure to radiation than adults (2,3). Many attempts have been made to calculate doses for children using body surface area (BSA) or BW (4,5). Because BSA is not readily measured, it is estimated by calculations using height and weight. Using the patient’s BW is easiest and has become the most commonly used method for determining radiopharmaceutical doses in pediatric patients (1). Recent discussions emphasizing the as-low-as-reasonably-achievable principle and the wide variations in pediatric doses have been the driving motivation to establish a standard for every pediatric nuclear medicine procedure. Four guidelines have been published to address pediatric dosing and imaging protocols. Guidelines from the Society of Nuclear Medicine and Molecular Imaging (SNMMI) address minimum and maximum activities based on BW and specific imaging protocols with 99mTc-labeled dimercaptosuccinic acid (99mTc-DMSA) (6). The SNMMI endorsed the North American Consensus Guidelines (NACG), which standardize doses based on BW for 11 nuclear medicine procedures, including 99mTc-DMSA. The NACG addresses dosing based on a fixed activity per kilogram but offers few details on imaging protocols (7). The American College of Radiology (ACR) dosing guideline for 99mTc-DMSA is a range (1.85–3.7 MBq/kg), with a minimum dose of 11.1 MBq (8). The ACR addresses imaging with minimum counts and maximum imaging time but also makes reference to the NACG. The European Association of Nuclear Medicine (EANM) guidelines recommend the use of a published dose card using BW (9). EANM also addresses imaging with minimum counts and maximum imaging time for 99mTc-DMSA (10). Current guidelines for pediatric dosing of 99mTc-DMSA are summarized in Table 1. Our department originally used an age-based method for dosing (neonate, 18.5 MBq; 1–4 y, 37 MBq; 5–10 y, 74 MBq; 11–15 y, 111 MBq), with minimum and maximum doses of 18.5 and 148 MBq, respectively. The dosing method was changed to BSA in 2009 to meet the RIVUR study criteria (11). The rationale was that BSA generally resulted in larger calculated doses and that more counts were needed to obtain good-quality images in infants and small children. In 2011, with the publication of the 2010 NACG, we examined our dosing method and changed to the ACR weight-based method. The ACR guidelines were chosen because they specifically address pinhole acquisition parameters and they include recommended parameters for imaging count and time. The upper activity range of the ACR recommendation was used because patients were not sedated and pinhole collimation requires prolonged imaging times leading to possible motion, which would obscure the presence of defects. The primary aim of this study was to compare the administered 99mTc-DMSA activity based on our department’s 2009–2010 practice of using BSA calculations with that based on our 2011 practice of using BW calculations while taking into account syringe residual activity. The second aim was to compare administered doses with the current ACR dosing recommendations including imaging time. These data can provide clinicians with greater guidance in dosing 99mTc-DMSA in pediatric patients and decreasing overall radiation exposure to patients and the public.
Summary of Guidelines for Dosing 99mTc-DMSA
MATERIALS AND METHODS
99mTc-DMSA prescription records were obtained from a BioRx software dispensing system (Biodose). We examined 368 records for study completion using a combination of dosing logs, picture archiving and communication system (Centricity PACS; GE Healthcare), and the hospital’s health care information system (Meditech). Records with complete information were examined for parallel-hole, pinhole, and total imaging time (Xeleris workstation; GE Healthcare). Inclusion criteria for the study were patients younger than 17 y receiving a renal nuclear medicine procedure with 99mTc-DMSA between January 2009 and December 2011. Exclusion criteria consisted of patients older than 17 y and those with incomplete information. Our facility is a tertiary-care academic pediatric hospital licensed for 230 inpatient beds with approximately 7,000 admissions per year serving all pediatric subspecialties. A research protocol and application was submitted to the campus institutional review board and was approved. Data collected included age, sex, height, weight, imaging protocol, indication, calculated 99mTc-DMSA activity, assayed 99mTc-DMSA activity, administered 99mTc-DMSA activity, residual syringe 99mTc-DMSA activity, imaging time, and notable patient or equipment factors affecting the procedure. From 2009 through 2010, the patient dose was calculated with a method described by Ziessman et al., using Mostellar’s BSA equation and multiplying the pediatric BSA/1.73 m2 by the ACR pediatric maximum activity of 185 MBq (11). The minimum dose used for this period was 18.5 MBq. In 2011, the patient dose was calculated using BW and multiplying by the ACR upper range of 3.7 MBq/kg. The minimum dose used for this period was 11.1 MBq. 99mTc-DMSA was obtained as a unit dose from a commercial radiopharmacy. From January 2009 until February 2011, all doses were dispensed in 1-mL tuberculin syringes (item 309626; BD) in a final volume of 0.3 mL. From February 2011 until the present, all doses were dispensed in 3-mL syringes (item 309572; BD) in a final volume of 0.3 mL. The 99mTc-DMSA syringe was assayed before and after administration to the patient, and the residual was recorded in the dose log book. This residual was used for syringe adsorption calculations. The difference between the pre- and postadministration activity assayed was recorded as the BSA and BW administered activity for each respective period. The protocol consisted of 5 static high-resolution magnified planar images 2–3 h after administration: for kidney size, 1 parallel-hole collimator image including both kidneys for 300,000 counts with the patient supine (Millenium MPR; GE Healthcare), and for cortical defects, 4 pinhole collimator images including left kidney and right kidney posterior views as well as left posterior oblique and right posterior oblique views for 150,000 counts each with the patient prone (Millenium MG; GE Healthcare). Descriptive and inferential statistics were performed. Testing of proportions, χ2 testing of associations, and correlation testing were conducted using Stata statistical software, version 10.1 (StataCorp LP), with an a priori α of 0.05.
RESULTS
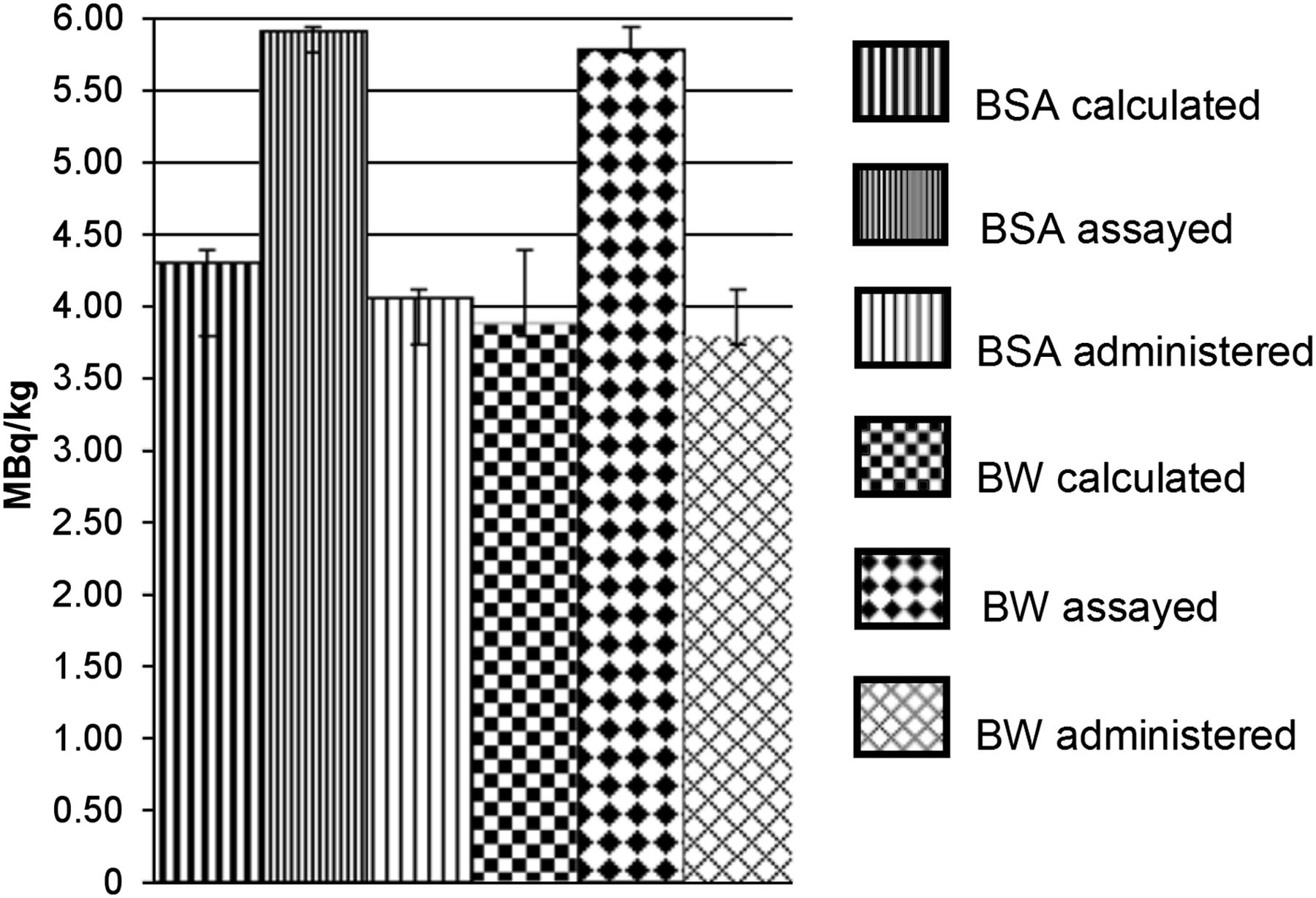
A total of 216 patient studies (47 boys, 169 girls) were analyzed for all parameters. Dose based on BSA was used for 127 studies, and dose based on BW for used for 89 studies. The age range of the patients was 43 d to 16 y (mean, 5.5 ± 4.4 y). Approximately 27% of patients were younger than 2 y, 45% were 2–7 y, and 28% were 8–16 y. Separately, a total of 232 records were analyzed for 99mTc-DMSA syringe residual activity only. Comparisons of average calculated, assayed, and administered activities per kilogram are summarized in Figure 1.

Comparison of average activity per kilogram.
Calculated Activity
Calculated activities based on BSA were higher on average than those calculated on the basis of BW alone. One patient in the BSA calculated group was defaulted to the minimum activity of 18.5 MBq and was not included in the data analysis.
Assayed Activity
Preadministration assay of syringes showed that all were in excess of the calculated amount. The average assayed activity was 21% higher in the BSA group and 24% higher in the BW group than the actual calculated activity. The assayed activity averaged 23.7 MBq (SD, ±31 MBq) in excess of the calculated activity in both groups. In all cases, the technologists added an amount to the calculated activity based on their individual experience to account for the potential of activity left in the syringe.
Administered Activity
The mean activity remaining in the syringe after flushing during patient administration was 30% (±11.5%), with a range of 3%–82%. The time between drawing of the dose and administration to the patient ranged from 8 min to 3.5 h. There was no correlation between the residual activity in the syringe and the length of time in the syringe or between the 2 sizes of syringes used. Administered activity correlations to BSA and BW calculations were 0.75 and 0.83, respectively. Overall, the average administered activity was 3.95 ± 1.98 MBq/kg (BSA group, 4.06 ± 1.58 MBq/kg; BW group, 3.79 ± 2.43 MBq/kg). In the BSA group, 69 patients (54%) were administered activity higher than the ACR upper guideline, whereas 6 patients (5%) received less than the ACR lower guideline. In the BW group, 36 patients (40%) were administered activity higher than the ACR guideline, whereas 4 (5%) received less than the ACR lower guideline. The difference between the 2 groups in the number of patients administered doses higher than the ACR dose guideline was significant (P = 0.036). Overall, 80% of patients younger than 2 y and 55% of the patients aged 2–7 y received a dose greater than 3.7 MBq/kg.
Imaging Time
The first static image of both kidneys averaged approximately 3 min (±1.6 min) for both groups. The subsequent 4 images with a pinhole collimator averaged 11.5 min (±6 min) for both groups. The average total imaging time was 14.8 min (±7.1 min) for both groups. The longest imaging time was 57 min, with the next closest at 37 min. There was a poor correlation between imaging time and administered activity (BSA group, r = 0.29; BW group, r = 0.17). For the 47% of patients receiving doses within the ACR recommendations, the average imaging time was 15.4 ± 7.7 min. For patients receiving less than 1.85 MBq/kg, the imaging time was 19.3 ± 10.5 min (P < 0.001). There were no significant correlations with imaging time and patient weight or age.
DISCUSSION
The average administered activity was significantly lower than the calculated activity and was significantly higher than the ACR guidelines. Forty-seven percent of the patients in this study were within the ACR activity range. If we compare our results with the NACG and EANM guidelines, our doses fell above these recommendations 95% and 90% of the time, respectively. Eighty percent of the patients less than 2 y old and 55% of patients 2–7 y old received a dose greater than the ACR recommendations. 99mTc-DMSA residual syringe activity was significant in both groups and is a well-documented occurrence with radiopharmaceuticals (12). The average residual in the syringe from our data was 30% (±11.5%), with a large range. The activity added to the calculated doses significantly affects patients of lower weight. For example, a patient weighing 6 kg has a calculated dose of 22.2 MBq. From the results of the study, we would expect an assayed amount of 45.9 MBq and an administered activity of 32 MBq (5.3 MBq/kg). The BSA-calculated dose correlations with administered activity were poorer than the BW correlations. This might be explained by the improved experience during the second study period. We were surprised to see no correlation with imaging time and the patient’s weight or age at this time and with these doses. In addition to dose, factors affecting the length of this procedure included use of a pinhole collimator, counts per view, and patient cooperation. The ACR recommendations indicate a corresponding imaging time of 45 min for this protocol. In our population, a pinhole image of over 20 min was associated with motion and restarts, whereas the parallel-hole collimator image in these same patients was noted as being of good quality. In addition, the NACG recommendation for 99mTc-DMSA administered activity is 1.85 MBq/kg. The assumptions used by the societies in constructing the consensus used planar whole-body and SPECT imaging on a dual-detector γ-camera equipped with a high-resolution collimator. They also note that higher administered activities may be required in selected patients (7). Most organs imaged in children are very small compared with adults and must be enhanced through the use of magnification or high-resolution techniques. Images acquired using pinhole collimators require more time than those acquired using parallel-hole collimators. The result is that patient motion may cause an image to be interpreted as poor quality. On the basis of our study, use of the BW calculation with the higher-range ACR recommendation and accounting for 30% syringe residual would yield a patient dose of 1.85–2.59 MBq/kg with a corresponding total imaging time of 18.7 ± 11 min. Once variability of absorption is not a factor, trials for further decreasing dose without sedation will be possible.
CONCLUSION
Reduction of radiation exposure is a key element in building any protocol, but the comfort level and stress of an examination on the patient should also be considered. Each facility must address its radiopharmaceutical dosing protocols and compare them with recommendations. A continuous quality improvement effort must be made to decrease administered activity if possible without loss of image quality. The inclusion of residual activity in the BW calculations or the use of a system that eliminates the activity lost during administration needs further investigation. The practitioner should always be mindful of dose recommendations and the parameters used for those recommendations. In any case, the amount of residual should be accounted for when the administered activity is reported.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank the following staff of the University of Oklahoma Nuclear Pharmacy: Ann Kirkpatrick, PharmD, BCNP, Adam Malek, DPh, BCNP, and Michael Sullens, DPh, BCNP. We also thank the following faculty and staff of the OU Medical Center: Dr. Leann Smith, Kim Brush, and Jean Nelson.
Footnotes
Published online Apr. 22, 2013.
REFERENCES
- Received for publication December 20, 2012.
- Accepted for publication February 26, 2013.





{kind=link}