


Abstract
A patient with a history of breast cancer underwent 3-phase 99mTc-methylene diphosphonate (MDP) imaging followed 3 d later by 3-phase 99mTc-sestamibi (MIBI) imaging. During the vascular and blood-pool phases, a lymph node over the right clavicle was seen on both the 99mTc-MIBI and the 99mTc-MDP scans at as early as 30 s and then became hotter. Four months after receiving chemotherapy, the patient achieved a complete response. The lymph node over the right clavicle vanished on ultrasound examination. The similar distribution of the blood-pool phase between the 99mTc-MDP and 99mTc-MIBI scans indicated that 99mTc-MIBI may similarly provide information on vascularization of the lymph node. In addition to indicating vascularization, our 99mTc-MIBI protocol may simultaneously provide information on P-glycoprotein expression important for predicting chemotherapy sensitivity. With information on the resistance of a tumor to drugs and the environment in which it dwells, chemotherapy sensitivity might be predicted more precisely.
The incidence of breast cancer has been increasing, and it can metastasize to lymph nodes and organs (1). Detection of these metastatic lesions depends primarily on ultrasound, MRI, and PET/CT (2). However, 99mTc-sestamibi (MIBI) scans were reported by Shiau et al. (3) as able to detect lymph nodes metastases in patients with non–small cell lung cancer.
99mTc-MIBI imaging is used to predict chemotherapy sensitivity and to map the distribution of multidrug resistance (4,5), which often leads to failure of chemotherapy. During this process, P-glycoprotein acts as an adenosine triphosphate–dependent efflux pump for cytotoxic drugs. A higher P-glycoprotein expression usually indicates a quicker excretion of cytotoxic drugs. 99mTc-MIBI can accumulate in tumor cells and then be excreted by P-glycoprotein. Thus, a tumor with only faint uptake of 99mTc-MIBI likely has high P-glycoprotein expression.
Currently, the 99mTc-MIBI protocol is applied to tumors mainly for calculating washout rate, at a speed of 1 min/frame for 15 min or even longer (6). However, a few studies have focused on the vascular and blood-pool phases of the 99mTc-MIBI scan. Besides P-glycoprotein expression, local vascularity is another important predictor of chemotherapy sensitivity. Therefore, a dynamic 99mTc-MIBI protocol with vascular and blood-pool phases might be useful in predicting chemotherapy sensitivity.
Vascular and blood-pool images are often acquired in the 3-phase 99mTc-methylene diphosphonate (MDP) imaging protocol. The disadvantage of this protocol is its long acquisition time and increased radiation exposure to injectors. Currently, 99mTc-MDP imaging is applied mainly for diagnosing the complex regional pain syndrome (7), osteomyelitis (8), diabetic foot (9), sports-related injuries (10), and so on. But according to a report by Yang et al. (11), 99mTc-MDP imaging was able to incidentally detect soft-tissue masses that were invisible on whole-body scintigraphy.
On the basis of these studies, we modified our 99mTc-MIBI protocol to simultaneously provide information on local vascularization and P-glycoprotein expression. Thereby, with information on the resistance of a tumor to drugs and the environment in which it dwells, chemotherapy sensitivity might be predicted more precisely. In addition, because 99mTc-MDP cannot deposit in soft tissues, its distribution in the vascular and blood-pool phases can be considered a contrast to exclude washout of 99mTc-MIBI in those 2 phases.
In this case report, our 99mTc-MDP and 99mTc-MIBI protocols both had vascular, blood-pool, and delayed phases. A lymph node metastasis over the right clavicle was detected by both. The extent of vascularization and 99mTc-MIBI deposition predicted a good response to cytotoxic drugs. Our follow-up confirmed the sensitivity of the tumor to chemotherapy.
CASE REPORT
Infiltrating duct cancer had been pathologically diagnosed in the right breast of a 55-y-old woman 3 y previously. She then incidentally found a mass over the right clavicle 3 mo previously. The mass had grown rapidly over the previous 10 d. On physical examination, the mass was fixed and had an unclear boundary. The patient’s chest radiograph showed bilateral increased lung markings that were considered bronchitis. Ultrasound showed multiple low-echo areas in the neck and over the right clavicle that were suspected to represent lymph node metastasis.
All 99mTc-MDP and 99mTc-MIBI images were acquired on a dual-head γ-camera (ADAC Laboratories) that was equipped with low-energy, high-resolution collimators. The energy peak was 140 keV, with a window width of ±20%. For vascular and blood-pool scans, the matrix was 64 × 64.
Shortly after intravenous injection of 925 MBq (25 mCi) of 99mTc-MDP, vascular-phase images were acquired at a rate of 3 s per frame for 2 min. Images of the blood-pool phase were then obtained at a rate of 1 min per frame for 6 min. Forty vascular-phase images were overlaid into 8 pictures using the ADAC software package. After 2.5 h, a delayed image was acquired with a scanning speed of 20 mm/min. Three days afterward, a 99mTc-MIBI scan was acquired using the same protocol except that the delayed image was acquired after 1.5 h instead of 2.5 h. All images were reconstructed and displayed with ADAC Scopix imager.
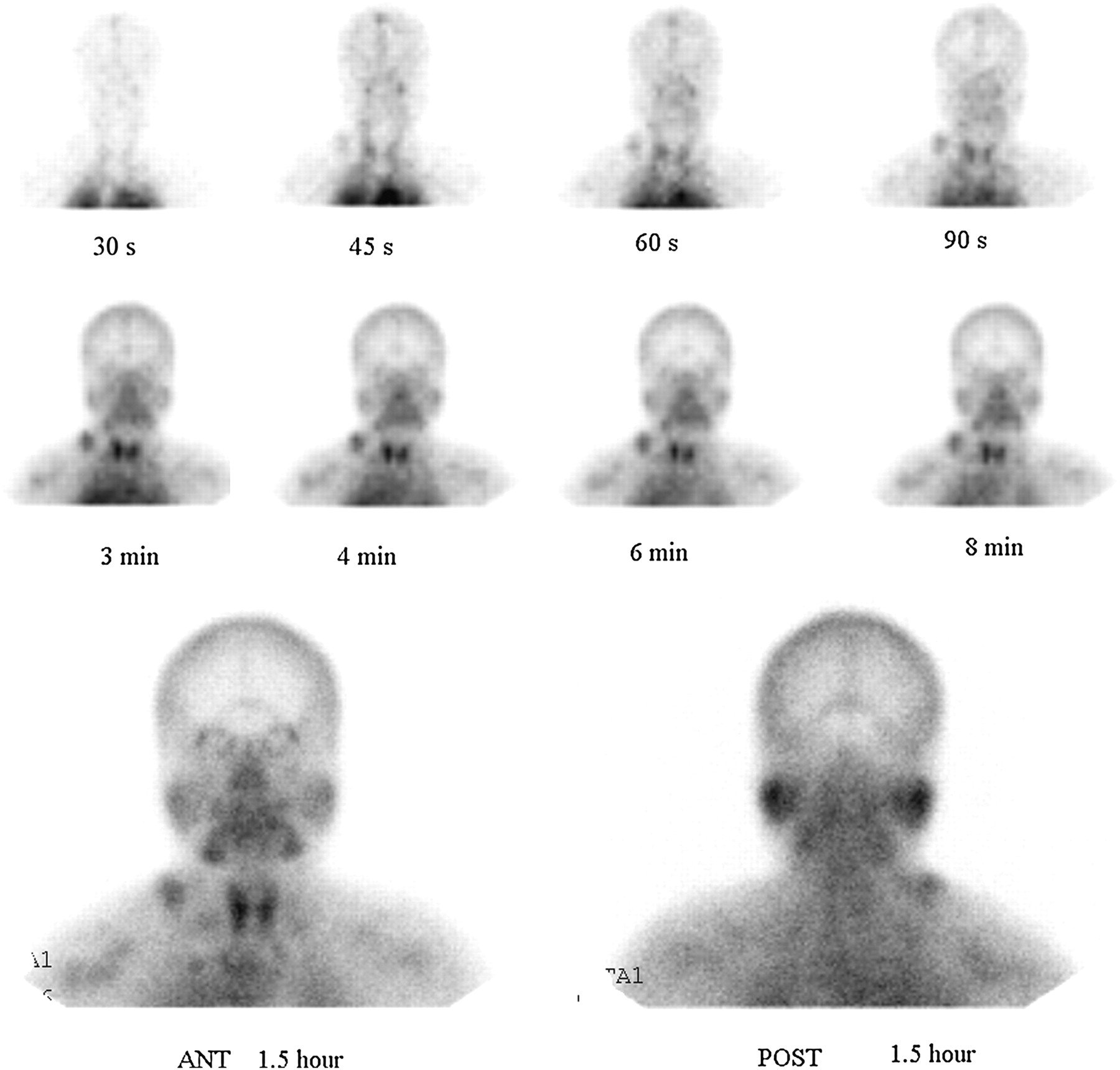
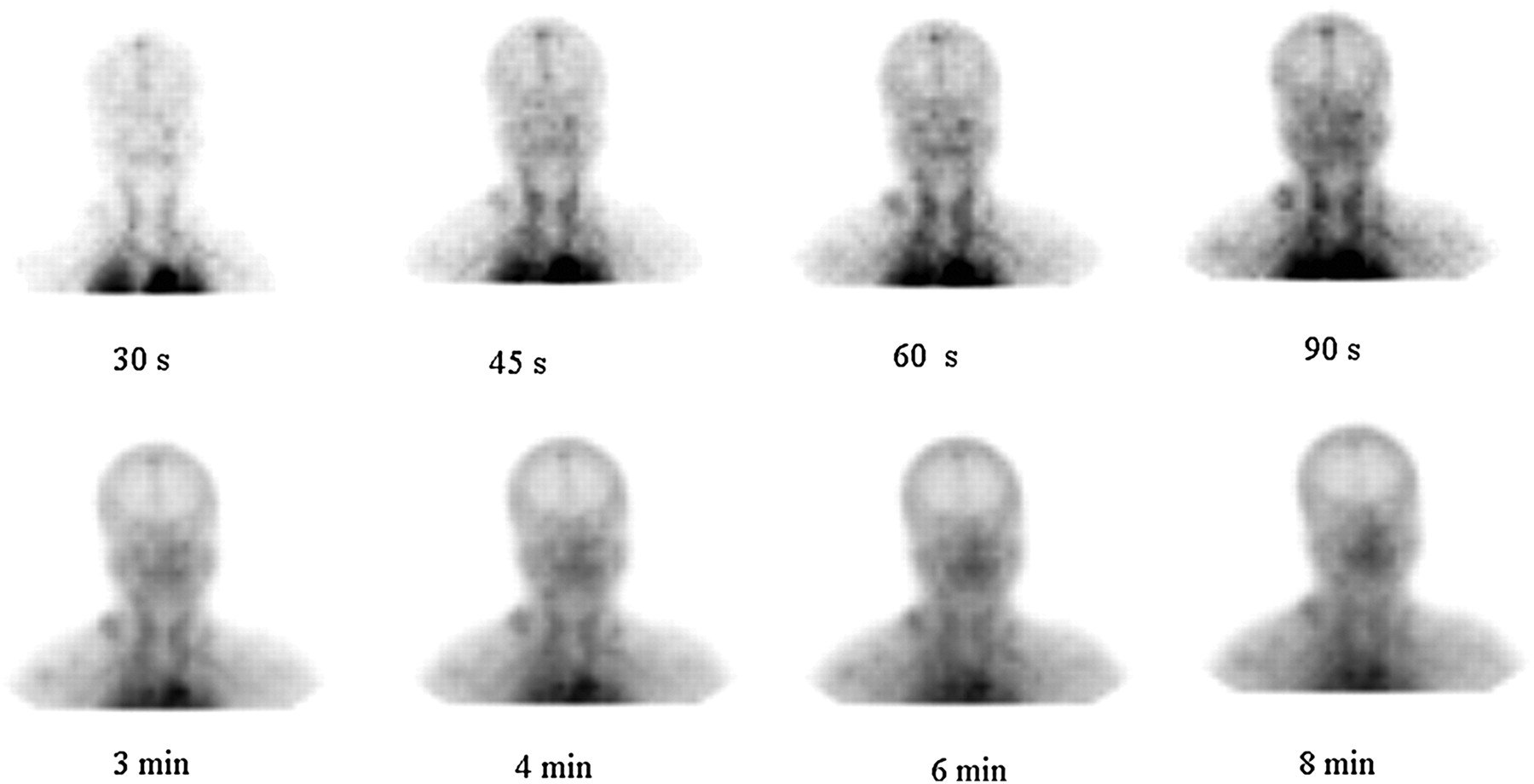
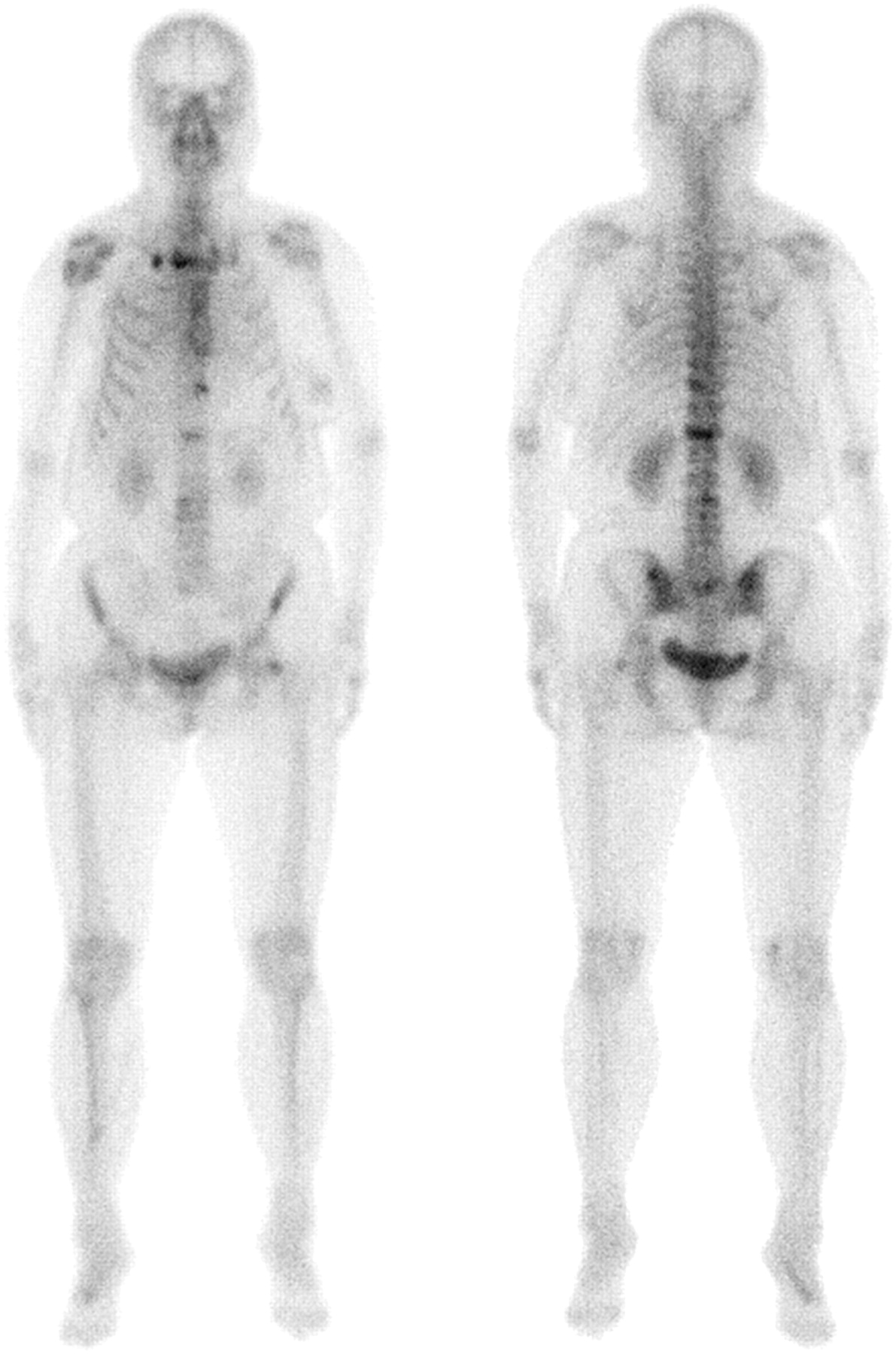
On the vascular and blood-pool images obtained with both 99mTc-MIBI (Fig. 1) and 99mTc-MDP (Fig. 2), a lymph node over the right clavicle was seen at as early as 30 s and then became hotter. The blood-pool images were similar for the 2 tracers. The lymph node was pathologically verified by fine-needle aspiration to be metastasis. On whole-body scintigraphy (Fig. 3), the lymph node did not accumulate 99mTc-MDP, unlike the bone lesions (right second anterior rib, manubrium, ninth to eleventh thoracic vertebrae, and first and third lumbar vertebrae). Overall, the 99mTc-MDP and 99mTc-MIBI scans indicated that the lymph node had an abundant blood supply and low P-glycoprotein expression.
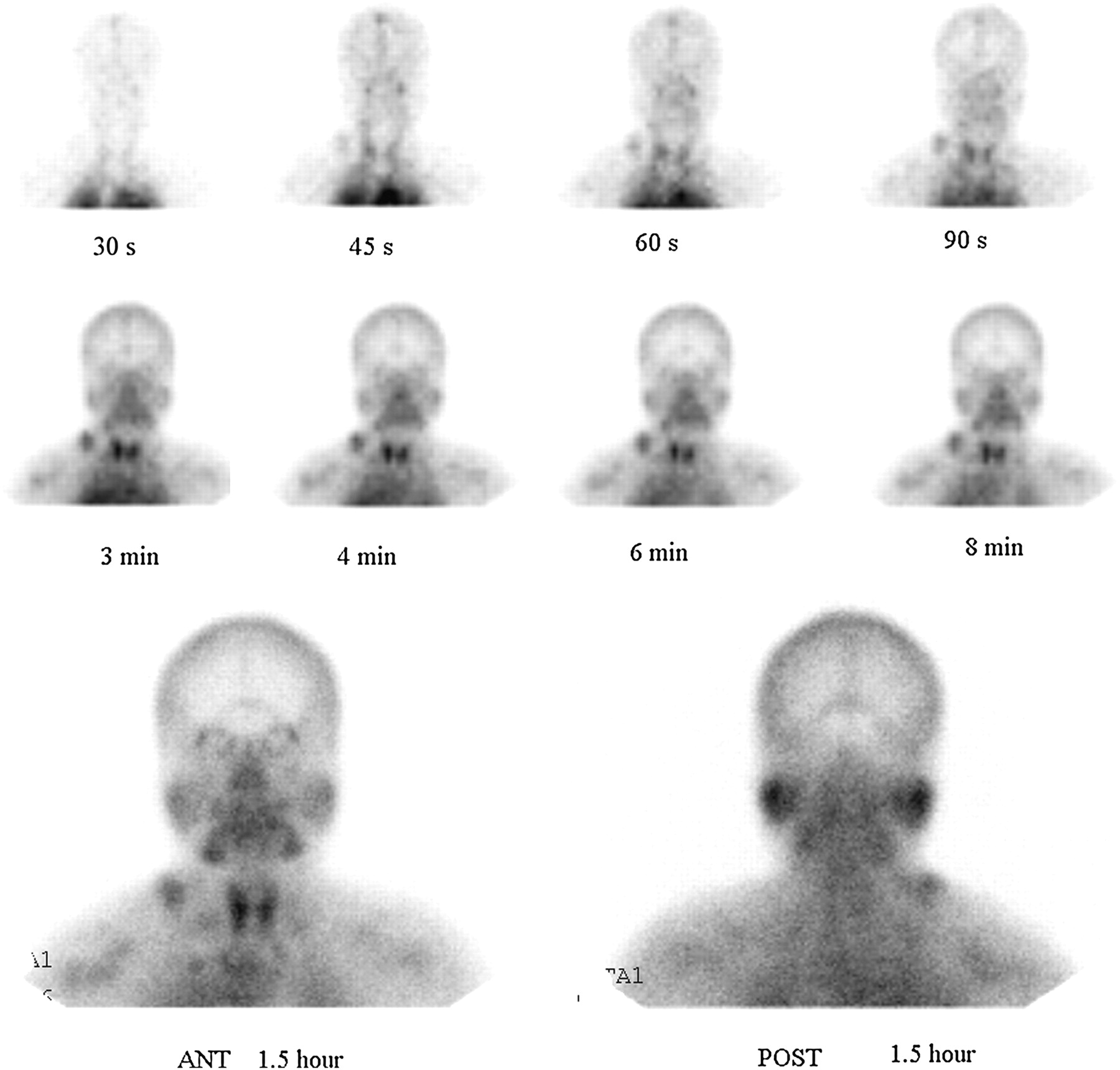
Blood-pool (top), vascular (middle), and delayed (bottom) 99mTc-MIBI images.

Blood-pool (top) and vascular (bottom) 99mTc-MDP images.

Delayed whole-body 99mTc-MDP images.
After undergoing scanning, the patient received a chemotherapy regimen consisting of 4 cycles of doxorubicin and cyclophosphamide. A complete response was achieved 4 mo later. The lymph node over the right clavicle disappeared on ultrasound examination. The extent of vascularization and 99mTc-MIBI deposition had predicted a good response to cytotoxic drugs, which was confirmed on follow-up.
DISCUSSION
Breast cancer cells often invade the systemic circulation through the lymphatics (12). Because of the limited spatial resolution of SPECT scanners and the local vascularization of tumors, vascular and blood-pool phases of 99mTc-MDP imaging often cannot detect these hot foci. Yang et al. and Davenport et al. (11,13) reported several cases in which extraskeletal foci were seen on vascular and blood-pool 99mTc-MDP images. As shown in our case, the metastasized lymph node was visible on the vascular and blood-pool phases of both 99mTc-MDP and 99mTc-MIBI scans. In addition, the 2 tracers were distributed almost identically in the blood-pool phase. Therefore, dynamic scans illustrate local vascularization without regard to the type of tracer before it is deposited into target tissue.
An environment of local vascularization is what enables a tumor to survive. It determines not only the amount of oxygen and nutrients that reach the tumor but also the amount of cytotoxic drugs. Therefore, local vascularization is an important factor in the sensitivity of a tumor to chemotherapy. As shown by other studies, dynamic PET can predict progression-free survival and be used to identify patients who will benefit from a chemotherapy protocol (14). Besides local vascularization, the P-glycoprotein expression of the tumor itself is another factor predicting its sensitivity. The relationship between P-glycoprotein expression and 99mTc-MIBI deposition has been validated by many studies (4,5).
In theory, our 99mTc-MIBI protocol simultaneously reflects the 2 important factors—vascularization and P-glycoprotein expression—that are the subjective and objective aspects, respectively, of chemotherapy sensitivity. As shown in our case, the metastasized lymph node had a good blood supply and low P-glycoprotein expression. These signs portended a good response to chemotherapy, as was verified on follow-up.
99mTc-MIBI imaging has some limits. At first, the spatial resolution of dynamic SPECT is low. Only relative large masses with a plentiful blood supply will be visualized. In addition, dynamic SPECT planar studies are limited by the position of a lesion. Only a mass outside the projection of a hot organ can be visualized during the vascular and blood-pool phases. Although further studies should be performed, our case illustrated the potential value of 99mTc-MIBI imaging in predicting chemotherapy sensitivity. In carefully selected patients, dynamic 99mTc-MIBI imaging may have great value for this use.
To conclude, the 99mTc-MIBI scan might simultaneously provide important information on vascularization and P-glycoprotein expression as an aid in predicting chemotherapy sensitivity. With information on the resistance of a tumor to drugs and the environment in which it dwells, its sensitivity to chemotherapy might be predicted more precisely.
Acknowledgments
Our study was supported by the Natural Science Foundation of Anhui Province of China (grant 090413132). A relative of the patient described in this article gave written informed consent to its publication. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Apr. 13, 2012.
REFERENCES
- Received for publication October 10, 2011.
- Accepted for publication January 10, 2012.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.