


Abstract
Secondary tumoral calcinosis is a rare disorder that is most prevalent in patients with chronic renal failure. It is characterized by lobular densely calcified masses confined to the soft tissue, generally at the extensor surface of a joint in the anatomic distribution of a bursa. We describe a case of a 38-y-old man undergoing dialysis who presented with pyrexia of unknown origin and raised inflammatory markers but was otherwise asymptomatic. A 67Ga scan was performed, on which an incidental diagnosis of secondary tumoral calcinosis was made.
Secondary tumoral calcinosis is rare, even in patients with chronic renal failure, and is usually clinically symptomatic well before any imaging is contemplated. This case demonstrates the utility of 67Ga scintigraphy in the work-up of pyrexia of unknown origin. As well as excluding gallium-avid renal cyst infection, the scan in this case showed multiple sites of secondary tumoral calcinosis, which is the likely cause of the persistent low-grade fever and raised inflammatory markers. 67Ga is not usually a first-line imaging investigation for secondary tumoral calcinosis but can show uptake due to the inflammatory process present in and around the masslike deposits of secondary tumoral calcinosis.
CASE REPORT
A 38-y-old man was referred to the nuclear medicine department from the renal dialysis unit. He had a 3-mo history of persistent low-grade fever with raised C-reactive protein levels on his blood tests. His septic screen for inflammatory disease processes, however, was negative. The patient also had a significantly raised parathyroid hormone level, despite a subtotal parathyroidectomy in 2007, and a raised phosphate level. The patient had autosomal dominant polycystic kidney disease with end-stage renal failure and was attending dialysis 3 times a week. In the past, he had been noncompliant with dialysis treatment and with taking phosphate-binding medication. Urinary tract ultrasound was undertaken to exclude an infective renal focus. The ultrasound showed swirling matter in one of the left renal cysts. A 67Ga scan was subsequently arranged to exclude infection within this cyst as a potential cause of the patient's fever and raised C-reactive protein level.
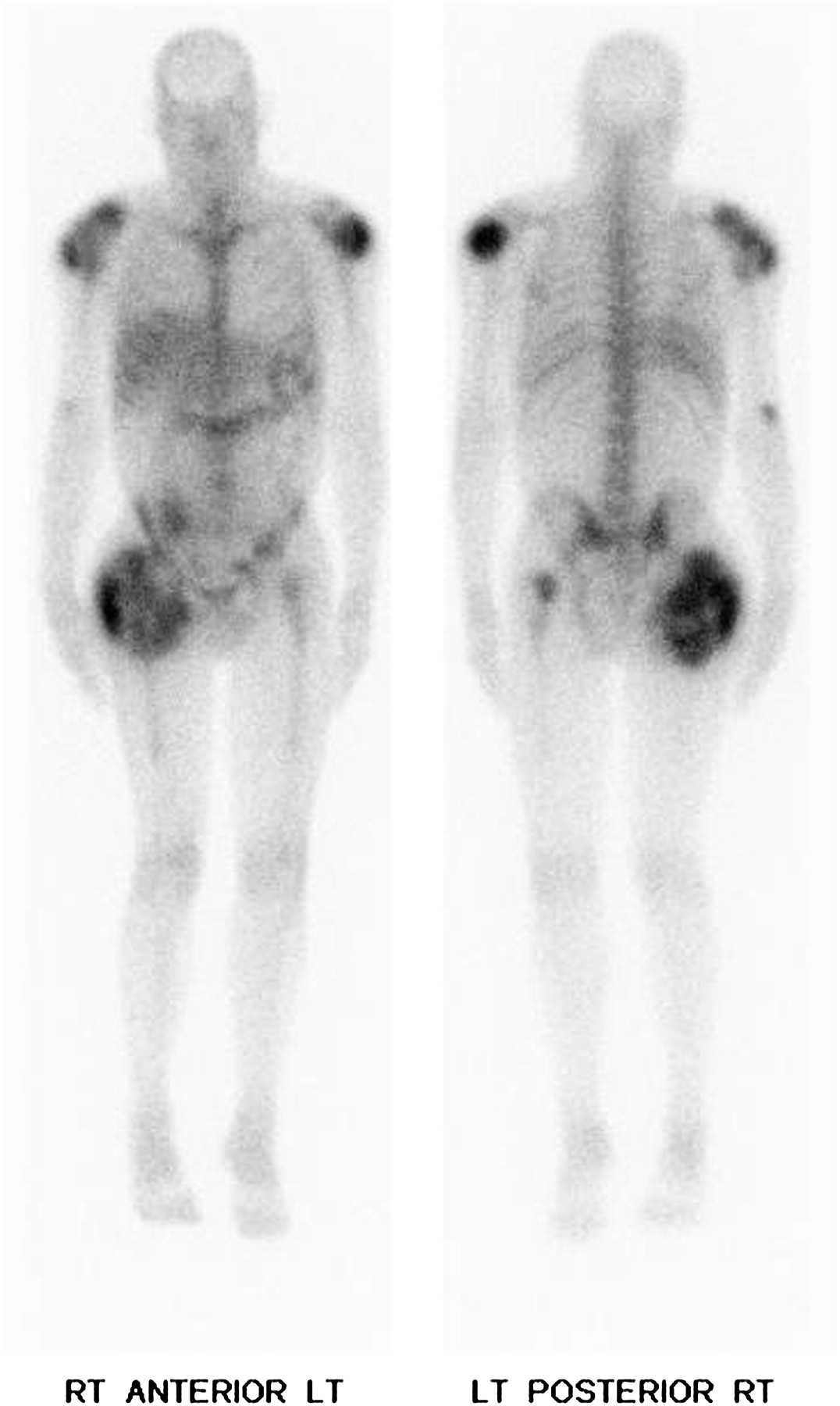
The 67Ga scan (Fig. 1) showed moderate-to-large areas of abnormal intense 67Ga soft-tissue accumulation around both the shoulders and the right hip, with small areas of accumulation also seen posteriorly in the left proximal thigh and right elbow. These corresponded to multiple areas of flocculent and expansile, masslike calcification on SPECT/CT (Fig. 2). In some locations, these masses were infiltrating into the adjacent muscles. The appearance was consistent with secondary tumoral calcinosis, which can be seen in the setting of chronic renal failure. There was no convincing evidence of abnormal 67Ga accumulation within the renal cysts to suggest that they were infected. Plain radiographs (Fig. 3) were also obtained to better demonstrate the areas of calcification seen on the 67Ga SPECT/CT scan.
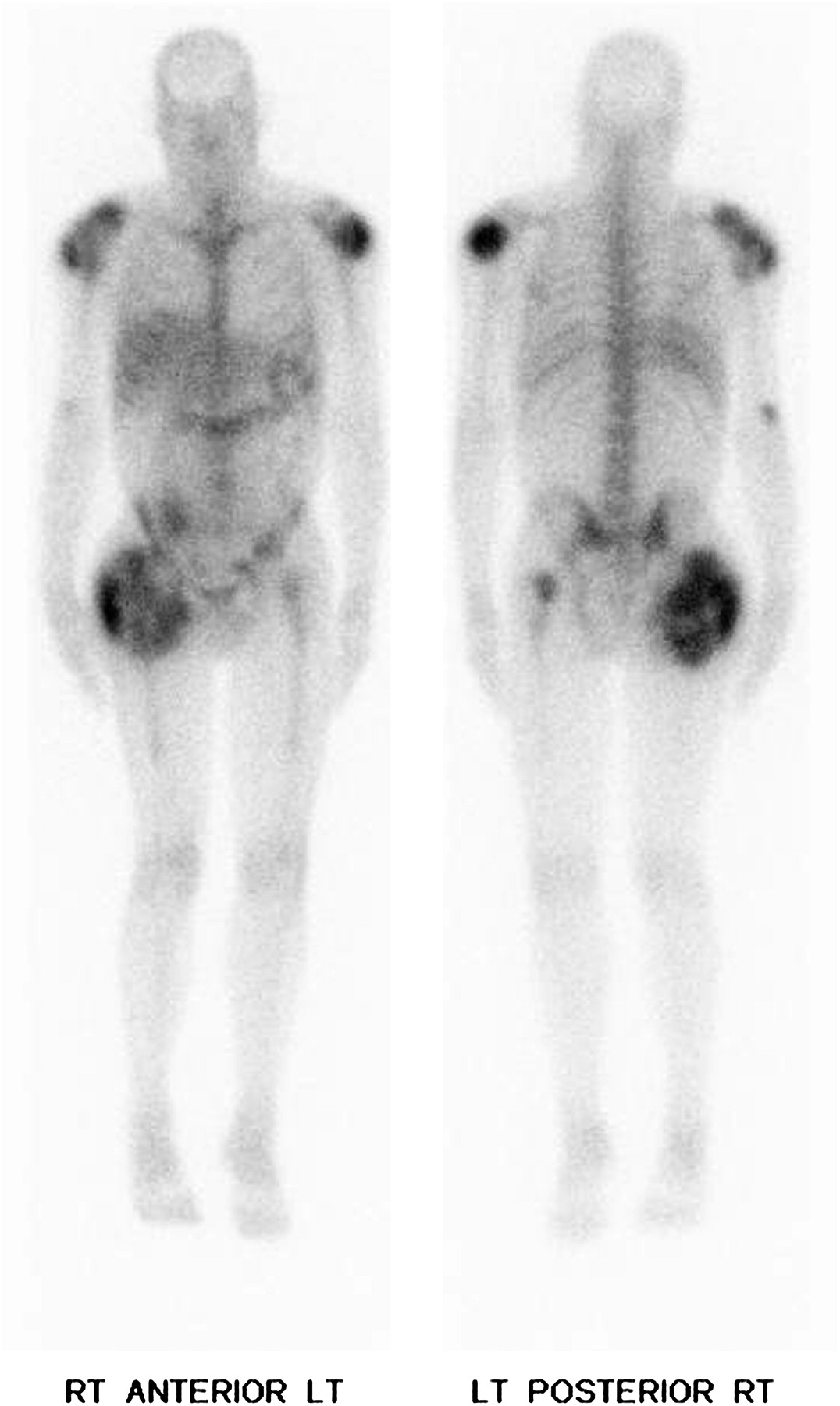
67Ga whole-body scan obtained at 48 h showing areas of increased activity in both shoulders, right elbow, and both hips.

67Ga whole-body fused SPECT/CT coronal images obtained at 48 h showing 67Ga uptake corresponding to areas of calcification in both shoulders and hips.
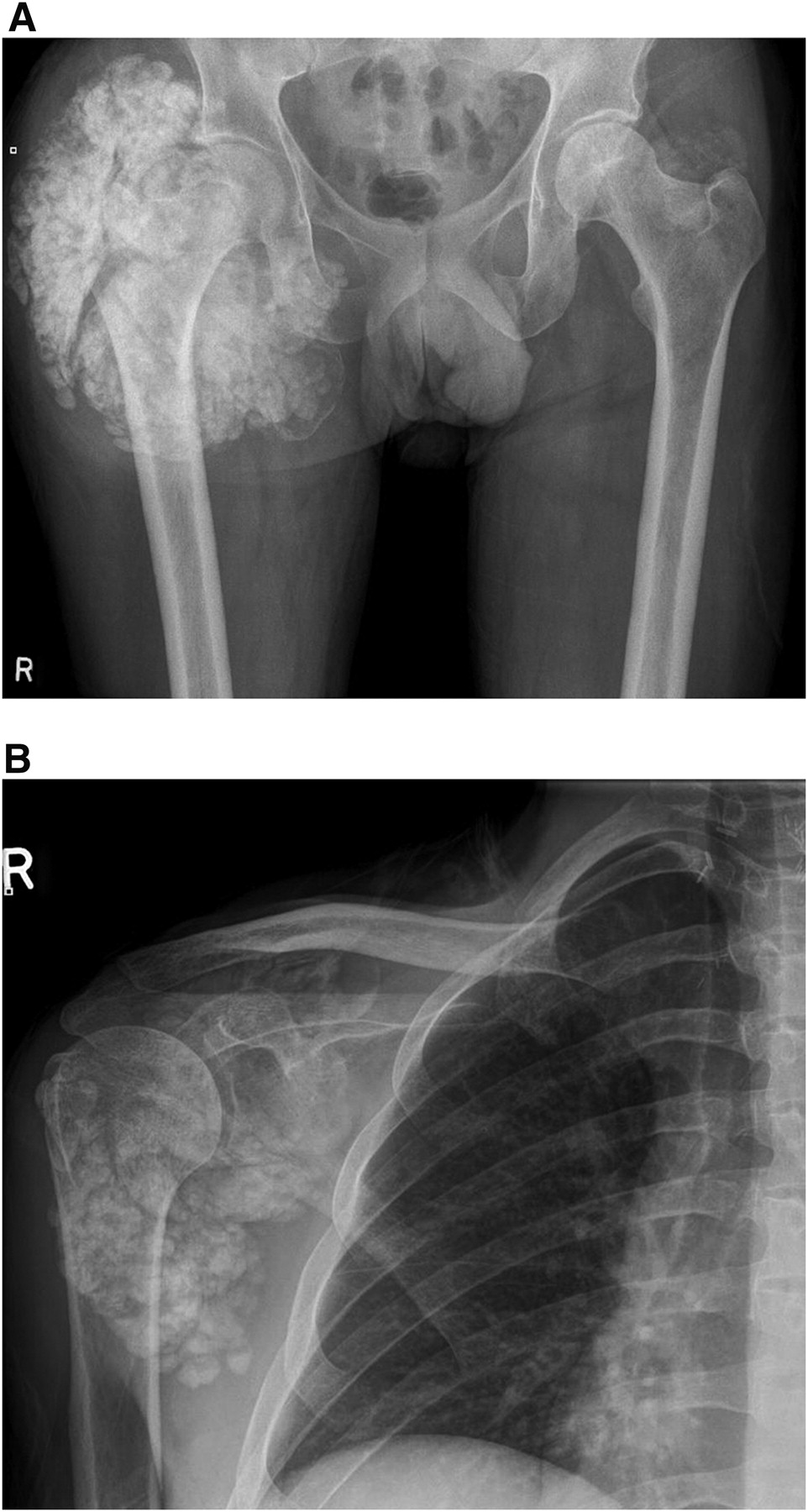
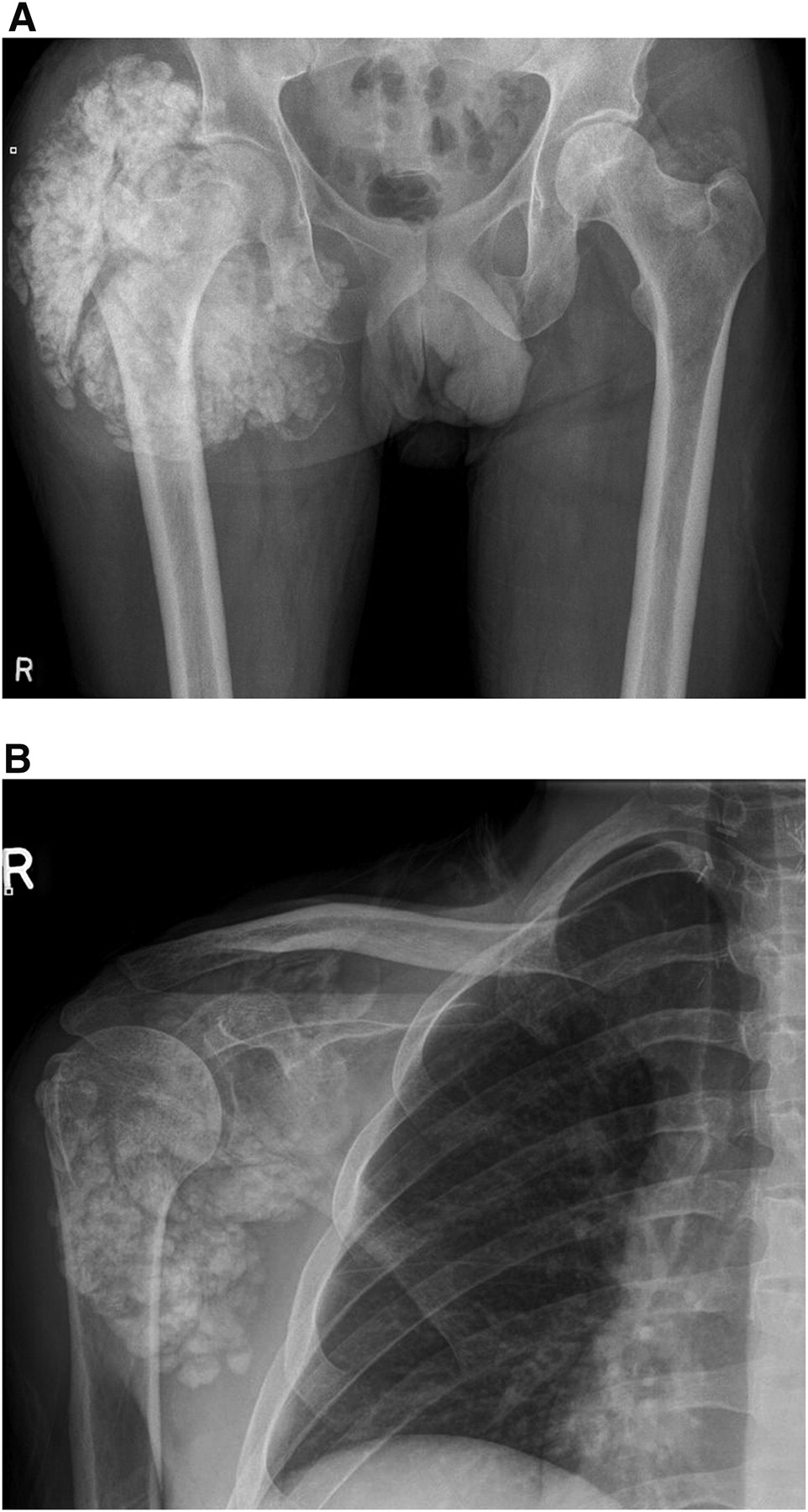
(A) Pelvis radiograph showing calcification in and around both hips. (B) Right shoulder radiograph showing calcification in and around shoulder joint.
After the scan results were known, the treating physician increased the number of dialysis hours and altered the patient's phosphate-binding medication regimen in an attempt to facilitate compliance. Routine work-up for renal transplantation continued.
On follow-up 6 mo later, the patient was again found to have been suboptimally compliant with a vast range of phosphate-binding medications, mainly because of unpleasant side effects. The patient, however, had been more compliant with attending dialysis treatment. The patient's most recent CT scan (Fig. 4) showed progression of the secondary tumoral calcinosis around the hips, particularly the right hip, which showed secondary erosive changes in the posterior aspect of the right femoral greater trochanter. He was also being investigated for raised parathyroid hormone levels.

CT transverse slice showing secondary erosive change in posterior aspect of right femoral greater trochanter.
DISCUSSION
Tumoral calcinosis is usually asymptomatic and is characterized as lobular densely calcified masses confined to the soft tissue, generally at the extensor surface of a joint in the anatomic distribution of a bursa (1).
There are generally 2 categories of tumoral calcinosis: primary tumoral calcinosis, which has 2 subgroups—normophosphatemic tumoral calcinosis and hyperphosphatemic tumoral calcinosis—and secondary tumoral calcinosis.
Primary tumoral calcinosis tends to be hereditary, affecting approximately half a sibling group because of a GALNT3 autosomal recessive gene mutation that induces metabolic dysregulation of phosphate. It occurs most commonly in people of African descent.
Secondary tumoral calcinosis displays the characteristics of tumoral calcinosis but is usually associated with other medical conditions, most commonly chronic renal failure. Although soft-tissue calcification in renal dialysis patients is not uncommon (secondary to calciphylaxis and heterotopic ossification), the prevalence of periarticular masses in this population is rare (∼0.5%–1.2%) (2). Tumoral calcinosis deposits can be solitary or, more frequently, multiple. The most common sites are the hip, shoulders, elbows, hands, and feet. The calcific deposits vary in growth rate and usually remain asymptomatic until large enough to cause mechanical limitation and pain due to compression of underlying nerves. Late-stage cases may present with ulceration and sinus tract formation, with exudation of the chalky or milky residue (3).
Secondary tumoral calcinosis can be diagnosed by radiographic findings in combination with patient history. The radiographic appearance is of rounded, cystic, and multilobular calcifications in a periarticular distribution (1). CT, MRI, and scintigraphic bone scans are the predominant imaging modalities on which secondary tumoral calcinosis is diagnosed.
Disease processes that can mimic tumoral calcinosis and complicate diagnosis include calcinosis universalis, calcific tendonitis, synovial sarcoma, osteosarcoma, myositis ossificans, and tophaceous gout (1).
The pathogenesis of secondary tumoral calcinosis in chronic renal failure is believed to be secondary to decreased production of 1-α-hydroxylase in the kidney, resulting in an inadequate conversion of calcidiol to calcitriol (the bioactive form of vitamin D). Reduced glomerular filtration rate results in phosphate retention, and this hyperphosphatemic state leads to hypocalcemia. The parathyroid hormone levels are elevated in a feedback mechanism in response to the hypocalcemic state. Thus, the combination of secondary hyperparathyroidism and vitamin D deficiency results in an elevated calcium phosphate product and predisposes to calcinosis in soft tissues (3).
Kidney transplantation—by stopping the pathogenesis of the disease process in patients with chronic renal failure—is the gold standard in the resolution of secondary tumoral calcinosis. The cessation of this process then allows the body to reabsorb the deposits already present. Secondary tumoral calcinosis before transplantation is managed by phosphate depletion—both by restricting phosphate intake by diet and by administering oral phosphate binders, intensifying the dialysis treatment program, and, in patients with a high parathyroid hormone level, excising the parathyroid and treating with calcimimetic agents (4). Surgical excision of the tumor is sometimes undertaken for cosmetic purposes and symptomatic relief; the deposits can recur after surgery. Radiation therapy and systemic steroid therapy have been used in the past but have been reported as being ineffective (1).
The mechanism of 67Ga uptake in cases of infection and inflammation is not completely understood. A commonly accepted theory suggests binding of the 67Ga to serum transferrin after intravenous injection. The gallium–transferrin complex binds to a cell surface transferrin receptor and is taken into the cell by absorptive endocytosis. This complex is then transported to the lysosome, where gallium is released and binds to acceptor proteins, possibly to ferritin and also lactoferrin. In inflammation, 67Ga has a greater affinity for lactoferrin, which is released from degranulated neutrophils. Uptake in chronic infection has been attributed to uptake of the gallium–lactoferrin complexes by macrophages (5).
Although the 67Ga scan did not demonstrate infective accumulation within the renal cysts in this patient, it did show increased uptake in the areas of the body where secondary tumoral calcinosis was subsequently shown to be present. It has been extensively reported that gallium localization in tumoral calcinosis may relate to active calcification within an inflammatory focus (6). There has been an equally large number of reports of tumoral calcinosis presenting clinically as pyrexia of unknown origin with or without other constitutional symptoms (7). Fever of unknown origin can be a concern to patients on a transplant waiting list, as an active fever can delay a life-saving transplantation operation.
REFERENCES
- Received for publication January 7, 2011.
- Accepted for publication January 25, 2011.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Related Articles
Cited By...
- No citing articles found.