


Article Figures & Data
Figures
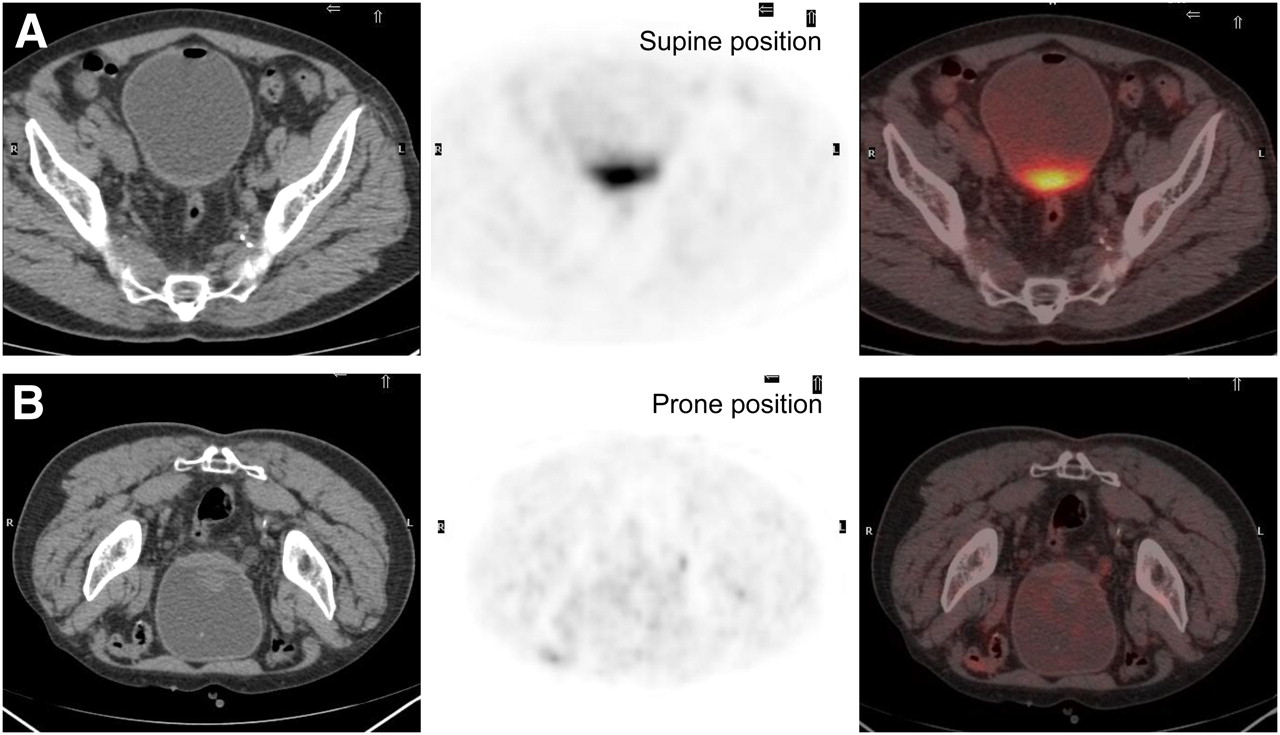
- FIGURE 1.
(A) Supine pelvic acquisition with retrograde filling of urinary bladder. Residual urine in dependent area of urinary bladder shows 18F-FDG activity. (B) Second set of images was acquired with patient prone and shows clearance of residual urinary activity.
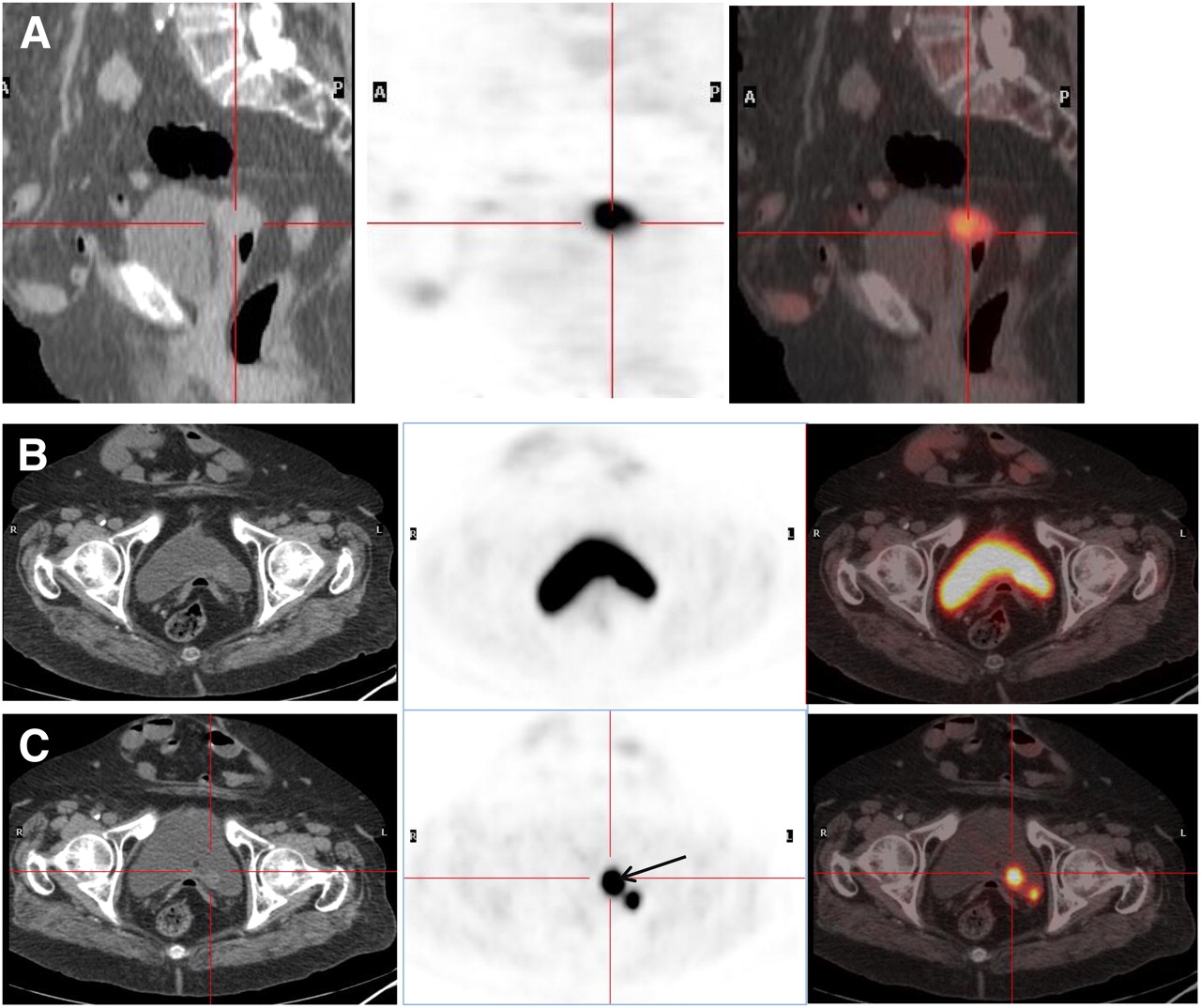
- FIGURE 2.
Patient with invasive colon cancer (sigmoid) that had gynecologic and ureteral involvement and was treated with surgery and chemotherapy. PET was requested because of suspected disease progression (vaginal mass on diagnostic CT scan). Images after retrograde filling of bladder (A and C) show vaginal involvement in sagittal projections (A) and two 18F-FDG foci in posterior bladder wall in axial projections (C) that were missed in standard acquisition (B). Lateral 18F-FDG deposit corresponds to ureter, and medial deposit (arrow), with a nodular lesion on CT image, corresponds to physiologic ureteral junction (false-positive).
- FIGURE 3.
Impact of retrograde filling of urinary bladder in ruling out or verifying bladder involvement. Patient had bladder cancer, and PET was requested for staging. (A) Pelvic axial PET image (right) shows bladder activity in anterior wall corresponding to anterior wall tumor thickening on CT (left). (B) Pelvic axial PET image with retrograde filling shows higher uptake in anterior wall, better defining lesion.
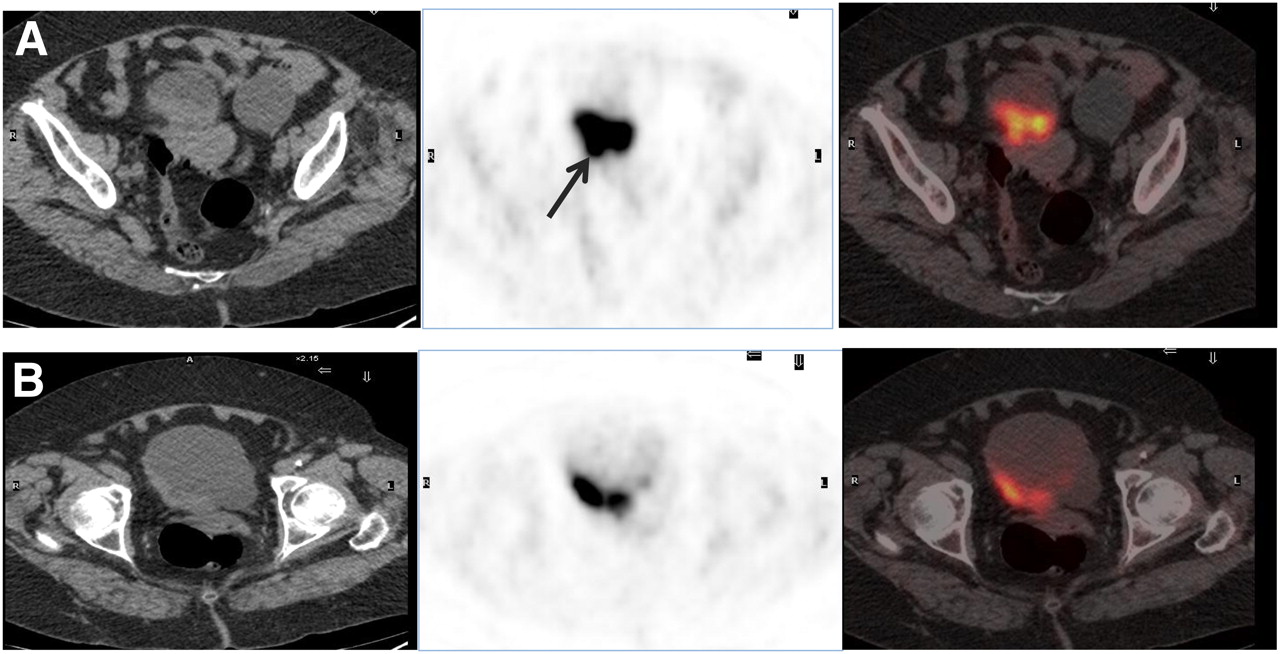
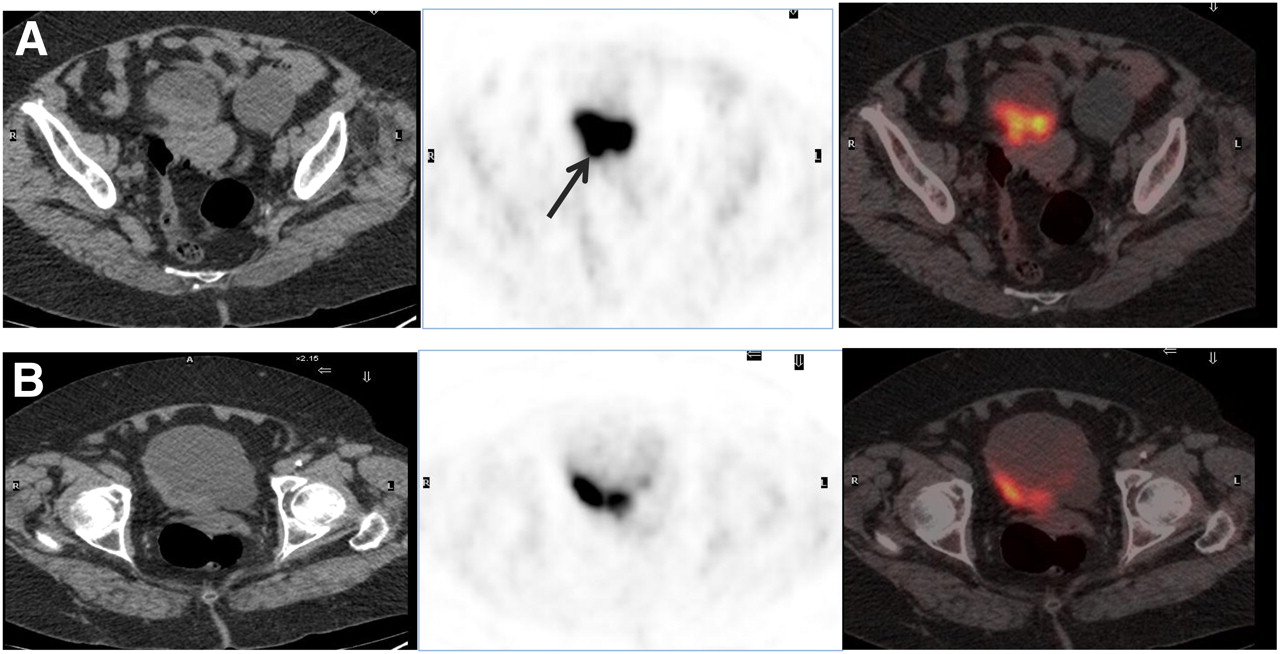
- FIGURE 4.
Impact of retrograde filling of urinary bladder in ruling out or verifying gynecologic involvement. Patient had bladder cancer and was treated with transurethral resection. Diagnostic CT scan showed diffuse bladder wall thickening and hypodense lesion in left ovary. (A) Standard PET image (center) shows uptake in posterior bladder wall, corresponding to wall thickening on CT (left), although image seems to show metabolic involvement of uterus (arrow). (B) Images with retrograde bladder filling better define bladder lesion and exclude uterus involvement. Histopathologic assessment (cystectomy plus hysterectomy) showed only residual bladder cancer.
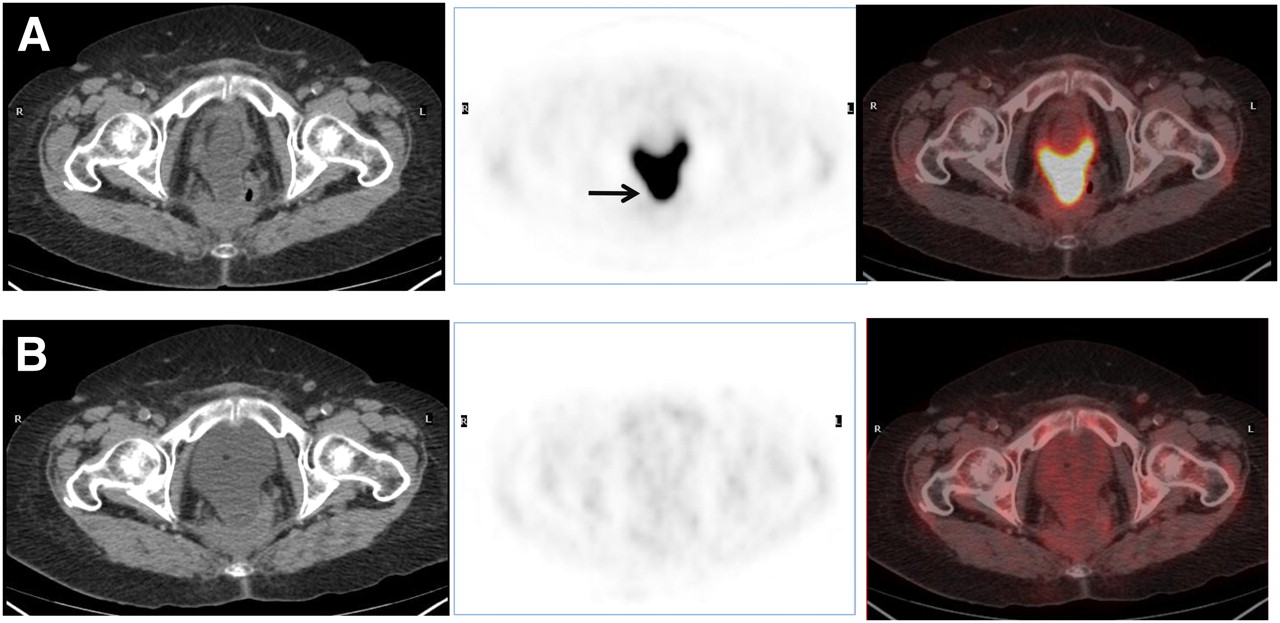
- FIGURE 5.
Impact of retrograde filling of urinary bladder in ruling out or verifying rectal involvement. Patient had surgically treated rectal cancer, and liver metastases were suspected. (A) Standard PET pelvic image (center) shows almost emptied bladder, with posterior extension close to rectal wall (arrow). (B) PET image with retrograde bladder filling shows complete disappearance of bladder 18F-FDG activity, ruling out rectal malignancy.

Tables
Study no. Patient no. Cancer history Age (y) Sex Previous treatment Location of pathology on CT scan Bladder wall thickness PET (+) pelvis PET (+) other location PET (+) bladder PET (+) total Final disease status Classification of pelvis Overall classification 1 1 Cervix (A) 54 F Surgery plus radiotherapy Pelvis Diffuse Cervix No No Yes Recurrence* True-positive True-positive 2 2 Testicle 76 M Surgery Pelvis Posterior lateral wall Spermatic cordon No No Yes Complete remission False-positive False-positive 3 3 Bladder 72 M TUR Pelvis Posterior lateral plus lymphadenopathies Prostate No No Yes Complete remission* False-positive False-positive 4 4 Cervix (A) 50 F Surgery plus radiotherapy — — No No No No Complete remission True-negative True-negative 5 5 Bladder (A) 44 M TUR plus radiotherapy Pulmonary nodules plus pelvis Posterior wall No Mediastinum No Yes Recurrence True-negative True-positive 6 6 Bladder (A) 78 F TUR Pulmonary nodules plus pelvis Diffuse Bladder No Yes Yes Recurrence* True-positive True-positive 7 7 Prostate and bladder (A) 67 M TUR plus radiotherapy Pulmonary nodules plus pelvis Diffuse No No No No Complete remission True-negative True-negative 8 8 Rectal (A) 56 F Surgery, chemotherapy, and radiotherapy Renal (?) No Presacrum No Yes (false-positive) Yes Recurrence* True-positive True-positive 9 9 Uterus (A) 54 F Surgery, radiotherapy, and chemotherapy Pelvis (ascitis) No No No No Yes Complete remission True-negative False-positive 10 10 Bladder and lung 76 M Surgery plus intrabladder chemotherapy Lung mass No No Lung No Yes Surgery True-negative True-positive 11 11 Bladder (A) 76 M TUR, chemotherapy, and radiotherapy Pelvis Right wall No No No No Complete remission True-negative True-negative 12 12 Cervix (A) 75 F Surgery, chemotherapy, and radiotherapy Pelvis (within the bladder) No Cervix–vagina No Yes Yes Recurrence* True-positive True-positive 13 13 Cervix 69 F Surgery Pelvis (vagina) No Vagina No No Yes Recurrence* True-positive True-positive 14 14 Gastric 64 F Surgery Pelvis Anterior–superior wall No No No No Complete remission True-negative True-negative 15 15 Cervix (A) 71 F Surgery, radiotherapy, and chemotherapy Pelvis (cervix) No Cervix Pulmonary solitary nodule No Yes Complete remission* False-positive False-positive 16 16 Prostate 70 M Radiotherapy — — No Bone chemotherapy No Yes Recurrence True-negative True-positive 17 17 Bladder plus urothelial 66 M TUR plus nephroureterectomy No No No No No No Complete remission True-negative True-negative 18 18 Anal (A) 67 F Chemotherapy plus radiotherapy Pelvis (anal nodule) No No No No No Complete remission True-negative True-negative 19 15 Cervix (scan 2) Surgery, radiotherapy, and chemotherapy PET/CT No No Pulmonary solitary nodule ↓ No No Complete remission True-negative True-negative 20 19 Renal plus bladder (A) 59 M TUR — — No No No No Complete remission* True-negative True-negative 21 20 Cervix (A) 41 F Chemotherapy plus radiotherapy Pelvis: MRI (fibrothecoma) No No No No No Complete remission True-negative True-negative 22 21 Bladder (A) 80 M Chemotherapy plus radiotherapy Pelvis Diffuse plus lymphadenopathies Prostate Suprarenal, lymphadenopathies Yes Yes Recurrence True-positive True-positive 23 22 Bladder and lung 74 M UR Lung mass No Bladder Lung Yes Yes Staging* True-positive True-positive 24 5 Bladder (scan 2) TUR plus radiotherapy — — No No No No Complete remission True-negative True-negative 25 5 Bladder (scan 3) TUR plus radiotherapy — — No No No No Complete remission True-negative True-negative 26 1 Cervix (scan 2) Chemotherapy plus radiotherapy — — Pelvic masses No No Yes Progression True-positive True-positive 27 1 Cervix (scan 3) Surgery plus radiotherapy Pelvis (masses) No Pelvic masses No No Yes Recurrence True-positive True-positive 28 23 Ovarian mass 64 F —† Pelvis (ovarian mass) No No No No No Staging* True-negative True-negative 29 24 Sigmoid colon IV (A) 73 F Surgery plus chemotherapy Pelvis (vaginal mass) No Vagina Lymph node Yes (false-positive) Yes Staging* True-positive True-positive 30 25 Bladder 79 F TUR Pelvis Anterior wall Yes No Yes Yes Recurrence True-positive True-positive 31 26 Colon IV (A) 48 F Surgery plus chemotherapy Liver No No No No Yes Recurrence True-negative True-positive 32 27 Bladder 50 M Partial resection‡ — — No No No No Complete remission True-negative True-negative 33 28 Cervix 55 F Chemotherapy plus radiotherapy — — No No No No Complete remission True-negative True-negative 34 29 Urothelial (A) 63 F Nephroureterectomy plus chemotherapy Pelvis Diffuse Ureter–bladder junction Suprarenal Yes Yes Recurrence* True-positive True-positive 35 30 Ovarian IV (A) 44 F Surgery plus chemotherapy Pelvis (pelvic mass) — Pelvic mass Lymph node No Yes Recurrence True-positive True-positive 36 31 Rectal (A) 67 F Surgery Liver — No Liver plus lymph node No Yes Recurrence True-negative True-positive 37 32 Uterus 56 F Surgery — — Cervix No No Yes Complete remission* False-positive False-positive 38 33 Rectal (A) 76 F Surgery, chemotherapy, and radiotherapy Pulmonary nodules — No Lung No Yes Recurrence True-negative True-positive 39 34 Uterus (A) 73 F Surgery — — No No No No Complete remission True-negative True-negative 40 35 Bladder and lung 81 M —† Lung mass — Bladder Lung Yes Yes Staging* True-positive True-positive 41 36 Bladder 76 M Surgery, radiotherapy, and chemotherapy Pelvis Diffuse Bladder No Yes (false-positive) Yes Hemorrhagic cystitis False-positive False-positive 42 37 Unknown origin tumor 47 M —† Lung nodule plus lymphadenopathies No No Lung plus lymph node No Yes Staging True-negative True-positive 43 38 Rectal (A) M Surgery, chemotherapy, and radiotherapy — — No No No No Complete remission True-negative True-negative





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.