


Abstract
The purpose of this study was to assess the feasibility of selective pelvic PET/CT with retrograde bladder irrigation in evaluating pelvic pathologies. Methods: Thirty-eight patients (22 women and 16 men), with a mean age of 61 y (range, 41–81 y) and a neoplastic background (most of them of pelvic pathology), were assessed with PET/CT. The most prevalent findings were urothelial (14 cases), gynecologic (12 cases), and rectal (7 cases) cancers. All but 3 patients had undergone previous surgical procedures or radio- or chemotherapy. Twenty-two patients had suspected pelvic pathology on a previous diagnostic CT scan. All the patients underwent a standard PET/CT protocol (from head to upper thighs) 60 min after the intravenous injection of 370 MBq of 18F-FDG. Additional delayed pelvic PET/CT images were acquired with a filled-bladder technique. Both series of images were assessed by 2 experienced observers. A lesion was classified as malignant if it showed a standardized uptake value greater than 2.5 or, in the case of subcentimetric lesions, any uptake greater than background activity that persisted or increased on delayed pelvic imaging. All lesions were evaluated histologically or by clinical follow-up. Results: Twenty-seven of 43 studies were categorized as pathologic using PET/CT. Nineteen studies showed abnormalities in the pelvis; the findings of 5 of these studies were false-positive. Ten studies showed pathologic 18F-FDG uptake in the bladder wall; in 7 of these studies the uptake was found to be true-positive on histopathologic examination. The sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of PET/CT in the pelvic assessment were 100%, 83%, 74%, 100%, and 76%, respectively. The retrograde filling reduced the interference with physiologic urinary accumulation of 18F-FDG in patients with possible pelvic lesions; no false-negative results were documented. Conclusion: In 18F-FDG PET studies, retrograde filling of the urinary bladder is recommended to assess bladder wall lesions and malignancies in other pelvic locations.
Several investigators have considered 18F-FDG PET of no utility in the detection of kidney, ureter, bladder, and prostate tumors (1–7). Because 18F-FDG is not reabsorbed as glucose, the limitation of 18F-FDG PET has been attributed to glomerular filtration and urinary excretion (8). Furthermore, high 18F-FDG activity in the urinary bladder is especially a problem in the evaluation of gynecologic tumors.
On the other hand, previous treatments or diagnostic procedures such as biopsy, radiotherapy, systemic chemotherapy, and intravesical agents (e.g., bacille Calmette–Guérin) can cause circumferential bladder wall thickening, mimicking bladder cancer (9). The pooled activity in the urinary bladder makes the evaluation of these bladder wall lesions difficult or even impossible.
Several methods have been used in an attempt to palliate this situation, with controversial results. Some approaches based on the continuous or not continuous irrigation of the urinary bladder have not been sufficiently effective in reducing bladder activity because the kidneys continuously fill the bladder with urine containing high concentrations of 18F-FDG (10,11). Other approaches have been successful in eliminating image artifacts originating from the kidneys, ureters, and bladder using diuretics, intravenous saline infusion, and a bladder catheter, but the studies were not focused on bladder cancer, for which radiotracer excretion is a major limitation (12,13).
The aim of our work was to evaluate the ability of retrograde bladder irrigation to clarify pelvic pathology. We also assessed the diagnostic and therapeutic impact of this procedure in those patients in whom PET/CT pelvic lesion evaluation was complicated.
MATERIALS AND METHODS
Patients
From March 2007 until June 2009, 38 patients (22 women and 16 men), with a mean age of 61 y (range, 41–81 y), were prospectively studied, following the inclusion criteria referred to in the “Methodology” section. Most of the patients had a pelvic neoplastic background: urothelial (14 cases), gynecologic (12 cases), rectal (7 cases), prostate (2 cases), and testicle (1 case). Twenty-two patients had locally advanced pelvic neoplasms. Two patients had nonpelvic tumors (tumor of unknown origin and gastric cancer).
All but 3 patients underwent surgical procedures or radio- or chemotherapy. Nine of 13 patients with bladder cancer underwent previous transurethral resection. The mean time between the completion of therapy or surgery and the diagnostic CT and PET/CT scans was 21 mo (1–96 mo).
Forty-three PET/CT studies were performed, for the following reasons: to investigate suspected recurrence (21 studies), perform postsurgical staging or restaging (13 studies), and evaluate response to treatment or follow-up (9 studies).
Twenty-two patients had suspected pelvic pathology on a previous diagnostic CT scan; wall thickening (6 focal and 6 diffuse) was the most prevalent indicator. The mean time between the diagnostic CT and PET/CT scans was 4 wk, except for 3 patients, for whom the interval was between 4 and 8 mo.
All patients fasted (except for water and medications) for a minimum of 4 h before the 18F-FDG PET study. Patients’ serum glucose levels were checked to ensure the readings were less than 180 mg/dL.
Methodology
PET/CT was performed at 60 min after the intravenous injection of 370 MBq of 18F-FDG, following a standard protocol (from head to the upper thighs, 3 min/bed position, 3-dimensional mode). The study was reviewed, and if any difficulty occurred in the evaluation, a second PET/CT scan was obtained using the filled-bladder technique. The inclusion criteria for this procedure were as follows: indeterminate or equivocal foci in gynecologic organs or rectum close to the bladder wall; neoplasm in pelvic organs close to the bladder, to rule out involvement by continuity; or radiologic alterations suggestive of malignancy in the bladder wall.
The additional pelvic PET/CT images were obtained using the filled-bladder technique, within 2 h after the standard acquisition. After voiding, a catheter was inserted under aseptic conditions and the patient was invited to stand up to complete the voiding. Then, the bladder was irrigated with 200–250 mL of physiologic saline, with the patient supine. After irrigation and immediately before the focal acquisition, patients rotated their pelvis to mix the possible remnants of urine with the normal saline solution. Whenever it was necessary to clarify an accumulation in the dependent area of the urinary bladder, a third set of images was acquired with the patient prone (Fig. 1).
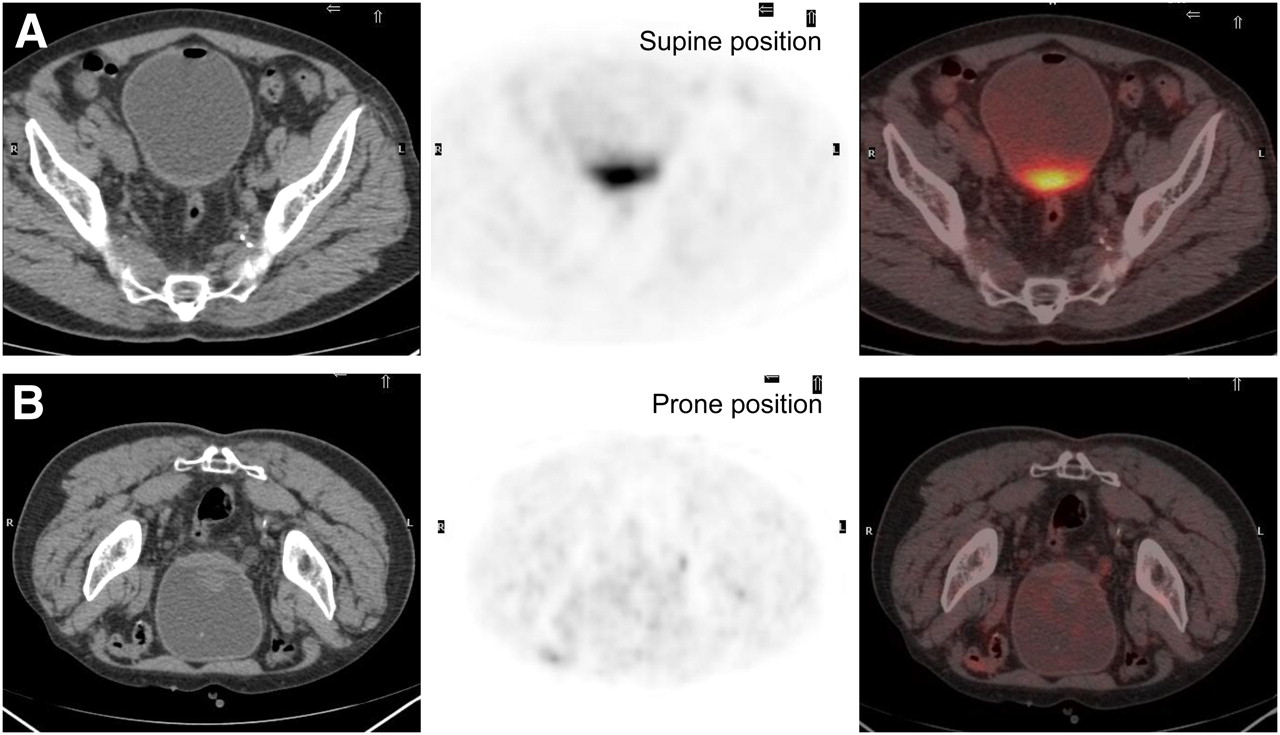
(A) Supine pelvic acquisition with retrograde filling of urinary bladder. Residual urine in dependent area of urinary bladder shows 18F-FDG activity. (B) Second set of images was acquired with patient prone and shows clearance of residual urinary activity.
Analysis of Images
Both series of images were assessed by 2 experienced observers. The filling of the urinary bladder was considered optimal if most of the urinary 18F-FDG activity disappeared and suboptimal if residual urinary activity was significant. A lesion was considered malignant if it showed a standardized uptake value greater than 2.5 or, in the case of subcentimetric lesions, any uptake greater than background activity that persisted or increased on delayed pelvic imaging. A pelvis was considered positive if any pathologic uptake was detected in this location. Furthermore, the bladder was carefully evaluated to rule out or verify malignancy, to establish the utility of the filled-bladder technique.
The diagnostic impact of filled-bladder PET/CT in ruling out or verifying bladder, gynecologic, or rectal involvement, and in better defining disease detected on standard PET/CT, was evaluated. An imaging study of the patient as a whole was considered pathologic if any pathologic location was detected, integrating both studies (standard acquisition and pelvic acquisition with filled bladder). Pathologic locations in the bladder and other pelvic organs, and the additional value of the filled-bladder image with respect to standard PET/CT images, were assessed. Also evaluated was the impact, on the final interpretation, of cases in which the filled-bladder technique had not been beneficial and cases in which technique had been suboptimal. Lastly, the therapeutic impact of the PET/CT final report with respect to the initial diagnosis was evaluated.
Final Diagnosis
All pathologic locations were evaluated histologically or by clinical follow-up of at least 12 mo.
Statistical Analysis
Statistical diagnostic parameters such as sensitivity, specificity, positive and negative predictive values, and accuracy were calculated for the assessment of pelvic pathology and overall evaluation.
RESULTS
The results are shown in Table 1. Twenty-seven of 43 studies were categorized as pathologic using PET/CT. Nineteen studies showed pathology in the pelvis, with 12 studies showing pathology exclusively in this location.
Distribution of Patients and Results
Malignancy was diagnosed in 21 patients, 14 of whom had malignant results in the pelvis. Thus, 6 of the results were false-positive: 5 in the pelvis. Those 5 were caused by inflammatory or physiologic processes, including 1 case of hemorrhagic cystitis in a patient with a permanent urinary catheter, 2 cases of cervical uptake in patients who underwent endometrial surgery (4 wk and 20 mo before PET/CT), 1 case of prostate hyperplasia, and 1 spermatic cordon interpreted as pathologic.
The maximum standardized uptake value (SUVmax) in all the false-positive lesions was higher than 2.5. The location with the lowest uptake was the cervix (SUVmax, 4.4), and the location with the highest uptake was the bladder (related to hemorrhagic cystitis; SUVmax, 10.5). All the locations showed an increase in SUVmax on delayed PET/CT scans using the filled-bladder technique.
Pathologic 18F-FDG uptake was detected in the bladder wall in 10 patients. After histopathologic examination, the uptake was found to be true-positive for 7 patients and false-positive for 1 patient (the patient with hemorrhagic cystitis). In the other 2 patients, the uptake corresponded to locally advanced colorectal cancers with vaginal and presacral involvement. PET/CT was requested for staging and follow-up, respectively, and showed that the uptake was probably associated with the bladder wall, but histologic assessment showed no impairment of the wall. Figure 2 shows 1 of these partial false-positive results.
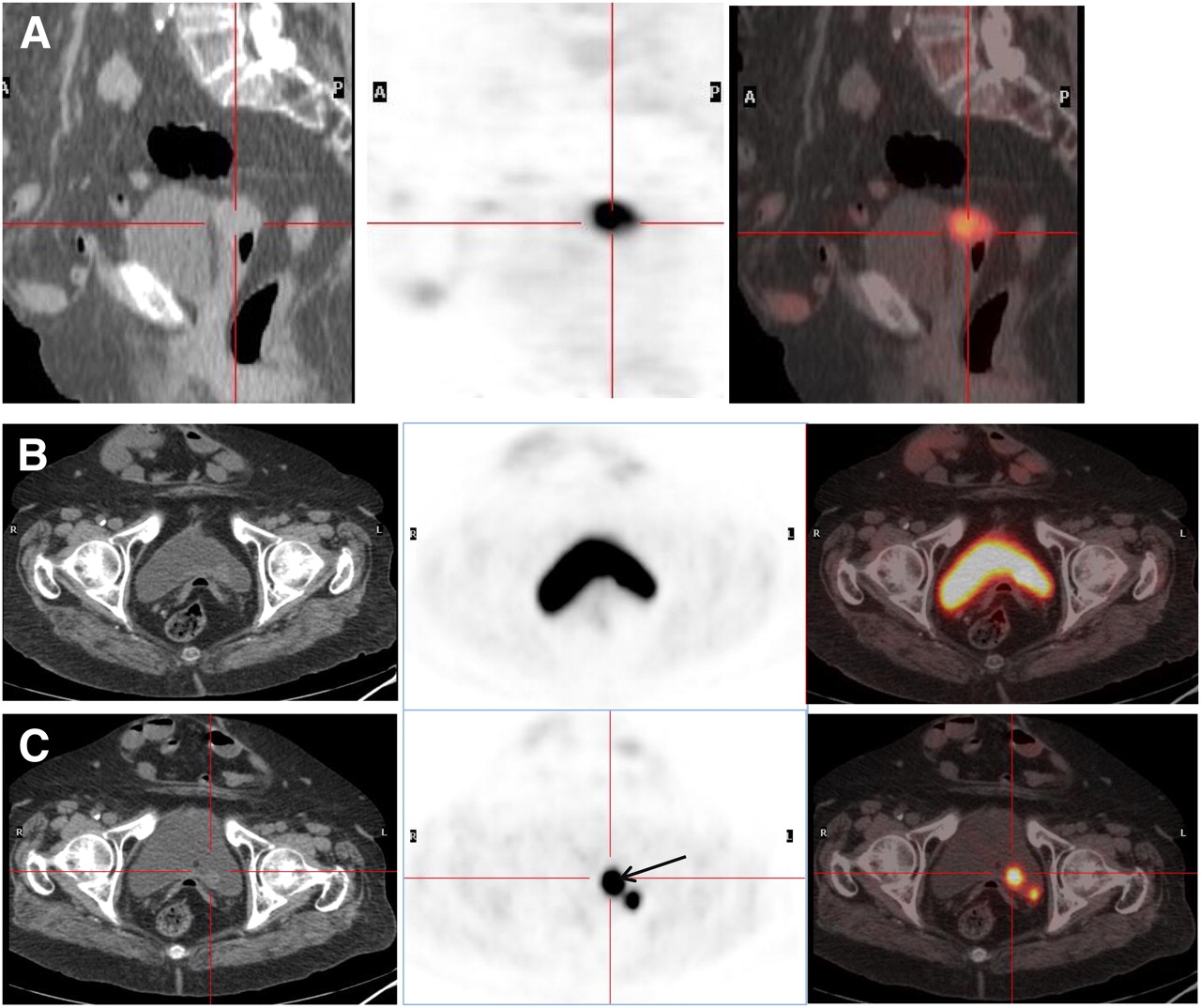
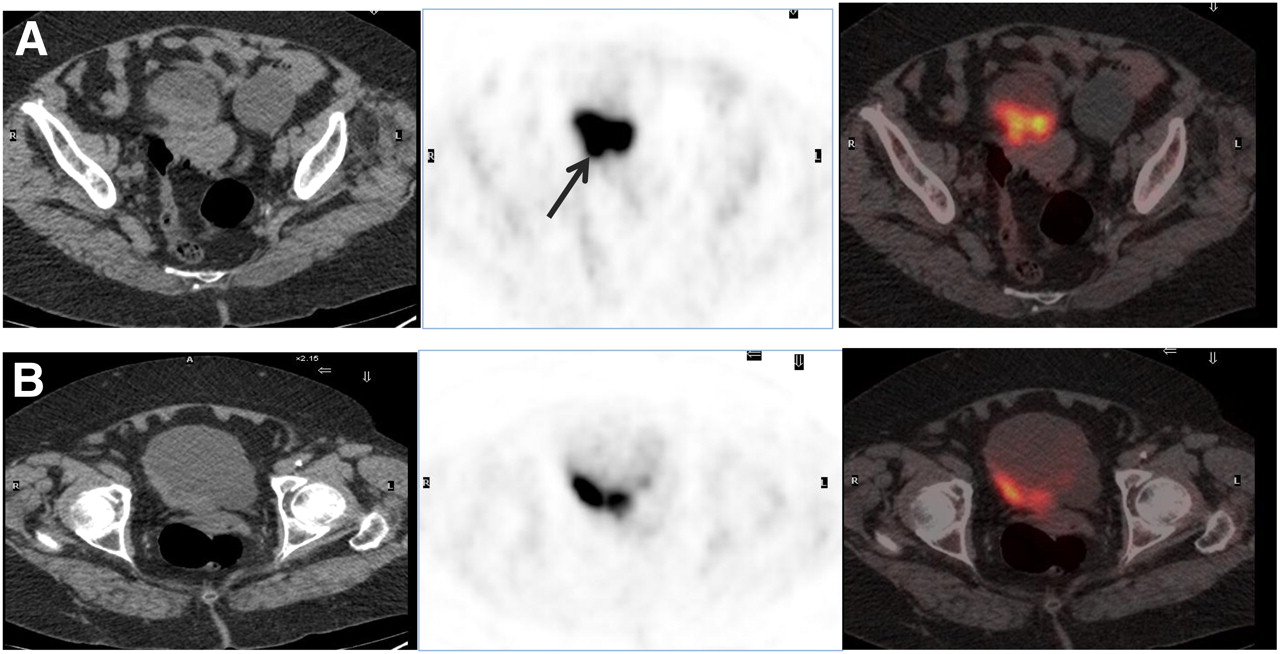
Patient with invasive colon cancer (sigmoid) that had gynecologic and ureteral involvement and was treated with surgery and chemotherapy. PET was requested because of suspected disease progression (vaginal mass on diagnostic CT scan). Images after retrograde filling of bladder (A and C) show vaginal involvement in sagittal projections (A) and two 18F-FDG foci in posterior bladder wall in axial projections (C) that were missed in standard acquisition (B). Lateral 18F-FDG deposit corresponds to ureter, and medial deposit (arrow), with a nodular lesion on CT image, corresponds to physiologic ureteral junction (false-positive).
Pelvic disease was ruled out by PET in 24 patients, none of whom demonstrated disease in the clinical evaluation; thus, no false-negative results were detected.
Table 2 shows the diagnostic impact of the procedure in relation to the suspected pathology. The most prevalent indication for the procedure was to rule out or verify bladder involvement (Fig. 3), followed by the other indications: ruling out or verifying gynecologic (Fig. 4) and rectal (Fig. 5) involvement.
Diagnostic Impact of Filled-Bladder Technique in Relation to Suspected Pathology

Impact of retrograde filling of urinary bladder in ruling out or verifying bladder involvement. Patient had bladder cancer, and PET was requested for staging. (A) Pelvic axial PET image (right) shows bladder activity in anterior wall corresponding to anterior wall tumor thickening on CT (left). (B) Pelvic axial PET image with retrograde filling shows higher uptake in anterior wall, better defining lesion.
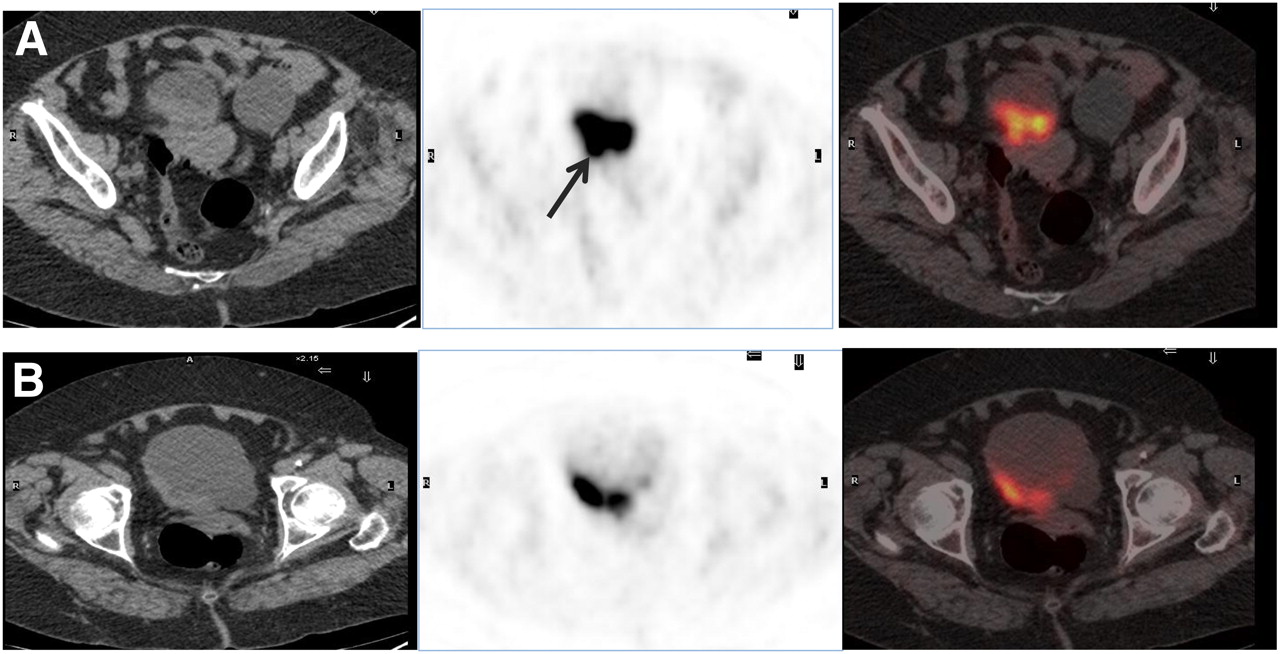
Impact of retrograde filling of urinary bladder in ruling out or verifying gynecologic involvement. Patient had bladder cancer and was treated with transurethral resection. Diagnostic CT scan showed diffuse bladder wall thickening and hypodense lesion in left ovary. (A) Standard PET image (center) shows uptake in posterior bladder wall, corresponding to wall thickening on CT (left), although image seems to show metabolic involvement of uterus (arrow). (B) Images with retrograde bladder filling better define bladder lesion and exclude uterus involvement. Histopathologic assessment (cystectomy plus hysterectomy) showed only residual bladder cancer.
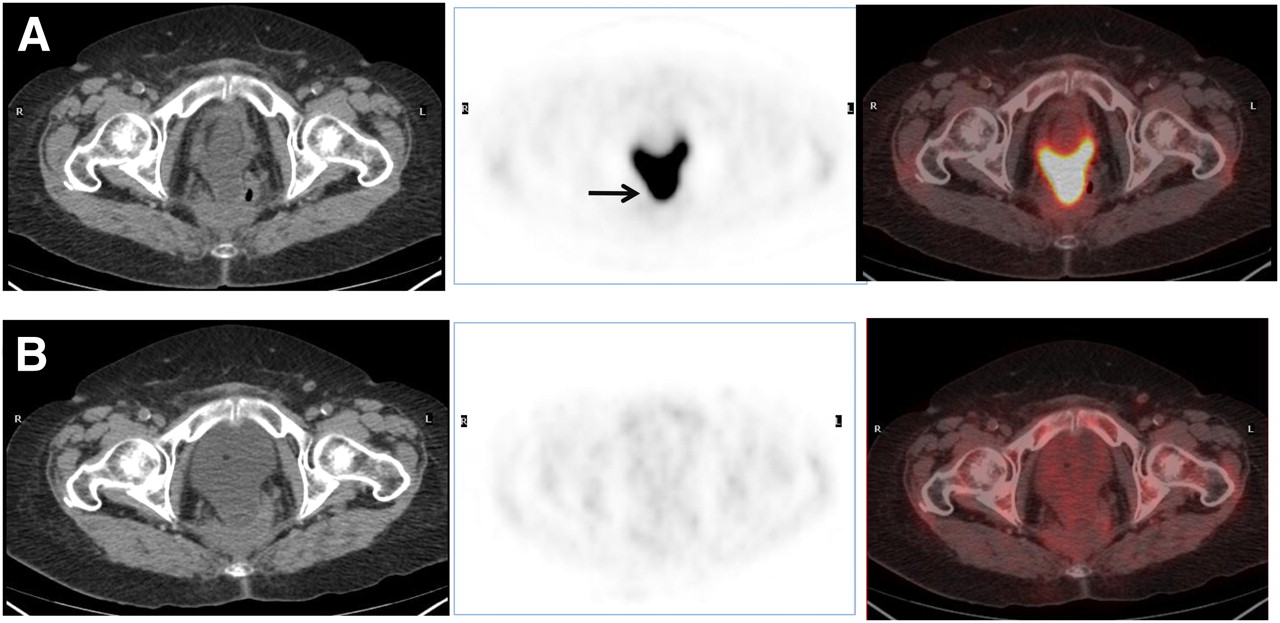
Impact of retrograde filling of urinary bladder in ruling out or verifying rectal involvement. Patient had surgically treated rectal cancer, and liver metastases were suspected. (A) Standard PET pelvic image (center) shows almost emptied bladder, with posterior extension close to rectal wall (arrow). (B) PET image with retrograde bladder filling shows complete disappearance of bladder 18F-FDG activity, ruling out rectal malignancy.
Because only 2 patients showed residual urinary activity (due to suboptimal filled-bladder technique) and this activity did not interfere in the diagnostic evaluation, the filled-bladder technique was considered capable of eliminating residual activity.
The final diagnosis was obtained by histopathologic assessment in 14 patients and by follow-up in the rest.
The sensitivity, specificity, positive and negative predictive values, and accuracy of PET/CT in the pelvis versus overall assessment were 100%, 83%, 74%, 100%, and 76%, respectively, versus 100%, 73%, 78%,100%, and 62%, respectively.
Therefore, in most patients retrograde filling of the bladder led to a better assessment of suspected lesions, avoiding any urinary interference, with a negative predictive value of 100%. Furthermore, in patients with a history or suspicion of bladder malignancy, the filled-bladder technique was crucial to rule out or detect wall involvement.
Regarding the effect of the filled-bladder technique on patient management, 1 patient was able to avoid unnecessary biopsy and 3 avoided pelvic surgery. Moreover, the procedure correctly indicated the need for pelvic surgery in 1 patient who had distant metastases suspected before undergoing PET and in another patient whose unsuspected pelvic disease was diagnosed on PET. In a patient whose bone disease had been diagnosed on the CT portion of PET/CT and confirmed on bone scanning and MRI, the filled-bladder technique revealed the need for systemic treatment. Therefore, overall, the technique was shown to have had an effect on the management of 7 of 38 (18%) patients.
DISCUSSION
The high 18F-FDG activity in the urinary bladder not only makes interpretation difficult but also may, in many cases, obscure or obliterate pelvic lesions (14). Therefore, eliminating high 18F-FDG activity in the urinary tract is important in the diagnosis of pelvic tumors using PET.
Several technical modifications—including adequate hydration, diuretic administration, and bladder irrigation—have been used in an attempt to limit background activity and increase the sensitivity of PET (15). Sugawara et al. (16) reported that the acquisition of images immediately after urination decreased the artifacts due to 18F-FDG accumulation in the urinary bladder and gave PET a satisfactory diagnostic ability, with 100% sensitivity. Other authors have reported that water loading and intravenous diuretic administration can decrease the retention of 18F-FDG in the urinary tract and that diuretic administration with placement of a catheter in the bladder is effective in eliminating image artifacts originating from the urinary tract (12,17).
Among these methods, bladder irrigation is the most direct and has been reported to be a useful tool in minimizing bladder activity from excreted 18F-FDG (10,14).
Several studies reported the usefulness of irrigation in the 18F-FDG PET diagnosis of locally recurrent rectal cancer (14,18) and primary gynecologic tumors (19–22). Koyama et al. (10) evaluated the utility of 18F-FDG PET with continuous urinary bladder irrigation to eliminate the artifacts from the urinary bladder in patients with gynecologic lesions and reported good results. In contrast, some authors have reported that retrograde filling of the urinary bladder may not completely eliminate urinary 18F-FDG activity resembling hypermetabolic lesions, causing even greater difficulty in interpretation (5,23). In our case, only 5 false-positive lesions were detected and none of them was due to urinary activity; these false-positive results were rather due to inflammatory processes that allowed an increase in 18F-FDG uptake in delayed PET acquisitions using the filled-bladder technique. However, with respect to a semiquantitative approach, these lesions had significant 18F-FDG uptake; thus, the modification of the standardized uptake value threshold would not have changed the final metabolic results or the accuracy of the technique.
Kosuda et al. (11) used retrograde saline irrigation of the urinary bladder to remove 18F-FDG radioactivity in 9 patients with suspected recurrent or residual bladder cancer, but these authors were unable to reduce tracer activity to background levels and reported a 40% false-negative rate for detection of recurrent or residual tumor in the bladder. Koyama et al. (10) observed that at least 8 (20%) of 41 studied patients failed to eliminate all 18F-FDG activity from the urinary tract, despite continuous bladder irrigation using prewarmed physiologic saline solution. In our study, no false-negative results were detected.
The saline fluid reduces the pitfalls caused by residual urine in retrograde irrigation; however, an accumulation of 18F-FDG in the dependent area of the bladder, complicating the evaluation of the posterior wall, is sometimes observed (24). Miraldi et al. (14) and Leisure et al. (12) reported that bladder irrigation alone may still permit pooling of 18F-FDG activity in the bladder. To palliate this effect, an alternative procedure has been explored. The prone position may eliminate the residual urine or move it from the posterior to the anterior aspect of the urinary bladder and verify that a result is false-positive (23,24).
Of our patients, only 2 showed diffuse activity from residual urine, and this finding did not affect the interpretation; few patients required the prone position. Therefore, an optimized procedure and knowledge of the normal patterns of urine distribution are necessary to minimize residual activity, misinterpretation, and false-negative and false-positive results.
Another aspect to consider is the diffuse 18F-FDG activity seen in the urinary bladder in some patients despite bladder irrigation or retrograde filling. This activity is probably due to the continuous excretion of 18F-FDG from the kidney to the urinary bladder. According to a study by Moran et al. (25), approximately 10% of the injected 18F-FDG is excreted between 30 and 60 min after 18F-FDG injection. Hence, bladder irrigation and retrograde filling during this time cannot dilute the urinary 18F-FDG activity, because there is still continuous excretion of high concentrations of 18F-FDG from the serum. Some authors have solved this situation with a delayed second bladder irrigation and retrograde filling (24). We preferred to obtain a delayed scan and fill the bladder when the residual urine was minimal. This practice perhaps explains the low rate of residual activity in our study.
Unlike diffuse activity, focal activity in the urinary bladder after irrigation and retrograde filling is of uncertain cause. Most authors have reported focal urinary 18F-FDG accumulations in the dependent portions of the urinary bladder (24), with different densities between the residual urine and refilled sterile saline possibly explaining the foci. Nevertheless, anterior layering of excreted 18F-FDG in the urinary bladder has also been described and may be explained by the lower density of urine than of sterile saline (26). One of the possible causes for urine of low specific gravity is the state of hydration, as Moran et al. (25) reported.
In addition, bladder irrigation is not without shortcomings. Some authors reported that retrograde filling of the bladder was invasive, caused discomfort to the patient, may cause infection (because these cancer patients are often immunocompromised), and increased radiation exposure to the staff performing the irrigation (10,12). On the other hand, repeated pelvic CT is estimated to produce a dose of 2.6 mSv—much less than a routine CT dose (average, 9 mSv) or average PET dose with (370 MBq [9 mSv] of 18F-FDG) (27).
Delayed bladder filling with respect to 18F-FDG administration, as used in this work, reduces 18F-FDG activity in the bladder and minimizes dosimetry for the nurse and technician.
There are few reports about the application of hybrid equipment in the evaluation of pelvic malignancies. The combined PET/CT scan may provide additional information to ascertain the nature of the 18F-FDG accumulation in the urinary bladder in patients with bladder wall thickening. However, CT images may not be useful in patients with distorted anatomy or postsurgical inflammation or radiation treatment. In our casuistic study, the mean time between the end of treatment and PET and CT studies, in patients with CT pelvic abnormalities, was enough to avoid any interference due to inflammatory therapeutic changes.
Furthermore, unfilled bladders may cause difficulties in the evaluation of the bladder wall on CT scans; thus, a full bladder is required to avoid false thickening of the walls (28). On the other hand, no wall thickening is detectable in any neoplastic processes, as Anjos et al. (29) reported. Therefore, in our experience, PET has shown better specificity and sensitivity than has CT in the evaluation of bladder wall lesions and other pelvic malignancies, although it is necessary to increase the number of patients to obtain more clinically useful information for each particular tumor type.
Some investigators have also found pelvic assessment using PET/CT to be challenging because the positions of pelvic organs may change between the PET and CT acquisitions (30). Heiba et al. (31), in reviewing integrated PET/CT images, observed considerable variation in the shape of the urinary bladder between the CT and PET scans and reported that this error can be significantly minimized by repeating the PET and CT scans of the pelvis in a single bed within a short period of one another. We did not observe any problem related to coregistration, even in a patient with a false-positive result (Fig. 2). In this patient, the accumulation of 18F-FDG as seen on PET matched perfectly with the final portion of the ureter in the bladder wall as seen on CT.
CONCLUSION
Retrograde filling reduces urinary 18F-FDG activity and improves the quality of 18F-FDG PET/CT images for pelvic tumor interpretation. Therefore, this technique is recommended to assess bladder wall lesions and malignancies in other pelvic locations.
REFERENCES
- Received for publication December 29, 2009.
- Accepted for publication May 18, 2010.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.