


Abstract
The aim of this study was to assess the practical role of a low-fat-meal gastric emptying protocol and its effect on a patient's compliance and comfort, number of patient referrals, daily nuclear medicine scheduling, patient throughput, and cost-effectiveness. Methods: We retrospectively reviewed the charts of patients who underwent low-fat-meal gastric emptying studies between February 2003 and February 2004. The study was approved by the University of Texas Medical Branch institutional review board. Results: A total of 117 studies were identified. There were 36 males and 81 females. A total of 36 patients had prolonged gastric emptying (30.8%), and 5 patients had rapid emptying (4.3%). The test meal was well tolerated by 112 of 117 patients (95.8%); 5 patients were unable to complete the meal (4.3%). Conclusion: We found that patient tolerance, compliance, and comfort with the low-fat-meal gastric emptying protocol were excellent, increasing the number of patient referrals. In addition, the low-fat-meal protocol can accommodate more patients and hence can be beneficial for busy nuclear medicine sections with a necessity for high patient volumes; the protocol also is cost-effective.
Diabetic gastroparesis (DG) is a known complication of long-standing insulin-dependent diabetes mellitus. Patients with this clinical condition often present with early satiety, postprandial abdominal bloating, nausea, and vomiting. Diagnosing this entity is often challenging because several other conditions mimic the symptomatology. Besides diabetes, there are several acute and chronic conditions that cause functional gastric stasis or delayed gastric emptying. Nonradioactive methods have limited value in diagnosing DG. A radionuclide gastric emptying study is the gold standard for the evaluation of DG. It is accurate and easy to perform and analyze. However, several imaging methods and different meals are available for performing radionuclide solid gastric emptying studies. Different institutions and practices use different test meals with various compositions and different imaging protocols. There is no standardization, and it is difficult to compare the studies performed at different institutions. The various imaging protocols are expensive and time-consuming.
At our institution, we have adopted the low-fat-meal gastric emptying protocol described by Tougas et al. (1) and have evaluated its practical role in a busy nuclear medicine section. The preliminary results were reported earlier as a brief letter-to-the-editor communication (2). The final, detailed results are presented here.
MATERIALS AND METHODS
A total of 117 low-fat-meal gastric emptying studies were performed from February 2003 to February 2004. The data were reviewed retrospectively. The study was approved by the University of Texas Medical Branch institutional review board.
There were 36 males and 81 females, ranging in age from 5 to 91 y. After overnight fasting, the studies were started in the morning between 8 am and 9 am. A test meal consisted of egg substitute (120 g of egg substitute, 252 kJ [60 kcal], equal to the volume of 2 large eggs), 2 slices of bread (504 kJ [120 kcal]), strawberry jam (30 g, 315 kJ [75 kcal]), and water (120 mL). The meal has a caloric value of 1,071 kJ (255 kcal) (a nutritional composition of 72% carbohydrates, 24% protein, 2% fat, and 2% fiber) (1). A total of 37 MBq (1 mCi) of 99mTc-sulfur colloid was mixed with the egg substitute, and the mixture was cooked on a skillet and used as the meal. The test meal usually was consumed by the patients within 10 min. Before the adoption of the low-fat-meal protocol, the test meal consisted of 2 scrambled eggs, 2 pieces of thin white bread toast, and 120–180 mL (4–6 oz) of water.
Scintigraphy
Anterior and posterior images of the abdomen were taken immediately after the completion of the meal (defined as time 0) in the upright sitting position. Further images were obtained after 60, 120, and 240 min in all patients. With the patient sitting or standing upright, 1-min anterior and posterior images were taken with a single-head camera in the 140-keV 99mTc peak with a 20% window.
Analysis of Gastric Emptying
Data were corrected for time decay. The region of interest was drawn around the image of the stomach for each time frame. For each time frame, the geometric mean was calculated as the square root of the product of the counts measured on the anterior and posterior images. The main parameters measured were percentages of gastric retention at 0, 60, 120, and 240 min.
Statistical Analysis
All results are reported as median and 95th percentile. The 95th percentile values for gastric retention at 1, 2, and 4 h are 90%, 60%, and 10%, respectively.
RESULTS
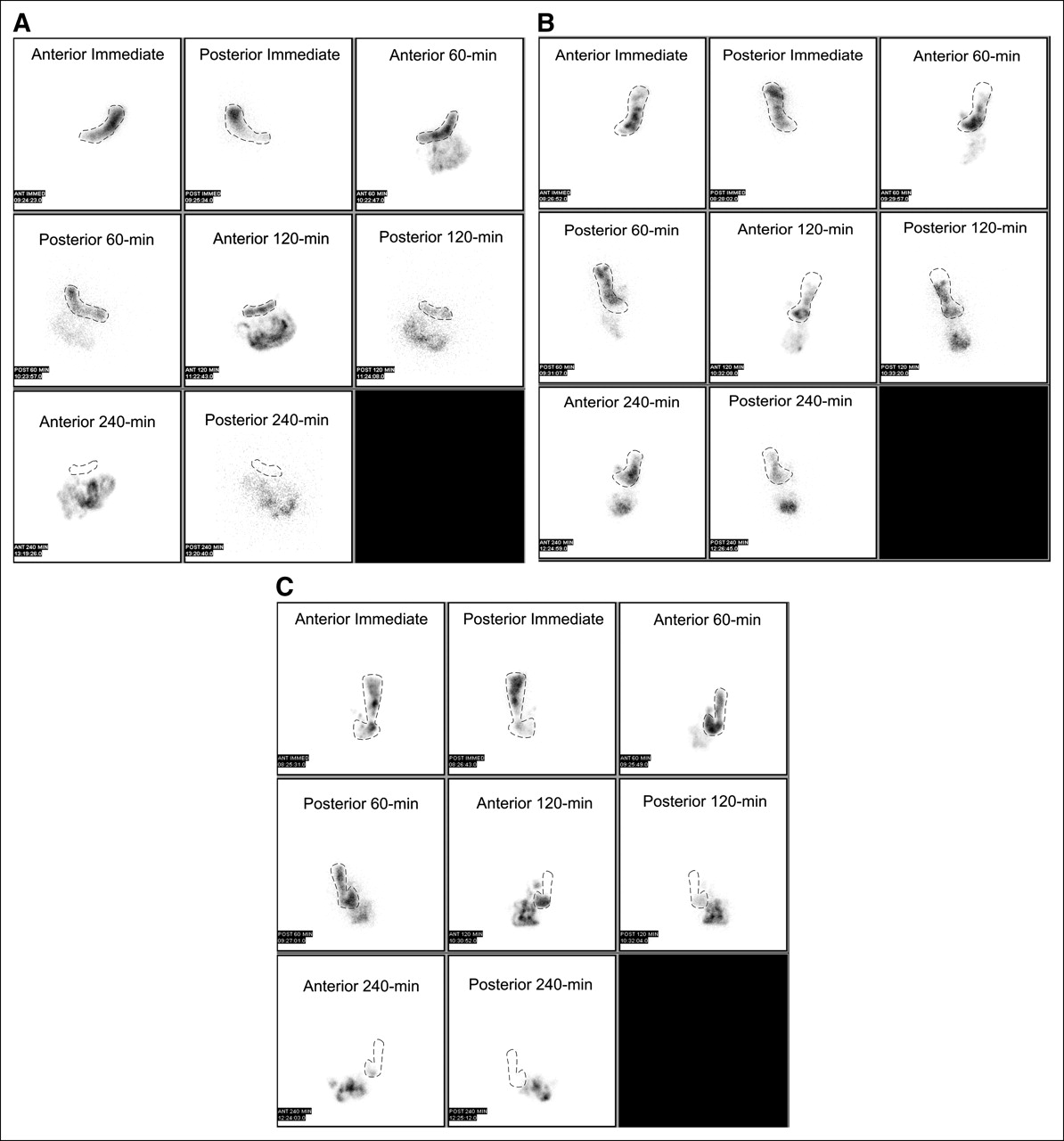
Among the 117 patients, 36 patients had prolonged gastric emptying (30.8%). Five patients had rapid early emptying (dumping) (4.3%). The test meal was well tolerated by 112 of 117 patients (95.8%); 5 patients (4.3%) were not able to consume the meal completely. The imaging and data analysis were completed successfully in all 112 patients who completed the test meal. None of the patients complained about the duration of the imaging protocol or any other discomfort. Examples of normal (Fig. 1A), delayed (Fig. 1B), and rapid (Fig. 1C) gastric emptying are shown. The 95th percentile values for gastric retention at 1, 2, and 4 h, respectively, were 56%, 18%, and 0.38% for normal gastric emptying (Fig. 1A); 93%, 78%, and 43% for delayed gastric emptying (Fig. 1B); and 64%, 0.38%, and 0.24% for rapid gastric emptying (Fig. 1C).

Anterior and posterior static images of stomach obtained immediately and at 60, 120, and 240 min demonstrate normal (A), delayed (B), and rapid (C) solid gastric emptying. Gastric region of interest in each image is indicated by dotted line.
DISCUSSION
In 30%–50% of patients with long-standing type I or type II diabetes, delayed gastric emptying or gastroparesis is reported (3). Radionuclide scintigraphy remains the gold standard for the diagnosis of gastroparesis (3–5). However, there is no standardization of meal or imaging protocols. Standard meal protocols often require lengthy patient waiting time, camera time, and technologist time (4). Efficient and simplified methods were evaluated recently (5–7). The commonly used dynamic or static imaging protocol requires a patient to lie supine on the imaging table for 90–180 min, causing tremendous discomfort for the patient and leading to patient motion during the study. In addition, this protocol takes significant γ-camera time. Before 2001, our institution was using a continuous 3-h gastric emptying imaging protocol requiring a single γ-camera during the entire time. Because of the prolonged camera time, it was possible to perform only 1 gastric emptying study per day. With the current imaging protocol that has been adopted, we are able to perform 2 or more gastric emptying studies per day. The protocol of Tougas et al. (1), with short acquisition times in the upright position, is very well tolerated by patients. However, patients must be on the premises for 4 h compared with 2 to 3 h for standard meal protocols. However, the γ-camera is not tied up during those 4 h for individual patients, and other procedures can be performed in between the static imaging procedures for gastric emptying, thus increasing patient throughput. Therefore, the gastroenterologists at our institution approve of this low-fat-meal imaging protocol and refer more patients for imaging.
Another major drawback of other protocols is the composition of the meal. Most patients are unable to tolerate a high-fat-content egg meal early in the morning. The egg substitute that we use with the current protocol is very well tolerated; only a few patients (4.3%) were unable to complete the meal. The meal is easy to prepare. In addition, the egg substitute meal is less expensive than other meals and therefore is cost-effective.
In addition to different meal contents and imaging acquisition protocols, gastric emptying also varies with body posture (8), sex (9,10), age (10), time of day, and medications (11). Lag-phase calculation also influences gastric emptying. Various other factors influence solid gastric emptying; these include motor control, electrical activity, hormones, composition of the meal, and body mass index (11,12). Several technical factors also play a major role in the evaluation of radionuclide gastric emptying studies; these include the type of radiopharmaceutical used and its decay characteristics, the attenuation method, the image acquisition method, single- versus dual-head γ-camera, single radioisotope versus dual radioisotope, the length and interval of acquisition and, finally, the method used for data analysis (13,14).
Finally, there are several other important aspects of the protocol of Tougas et al. (1). The study of Tougas et al. (1) was a multicenter study with participation from 4 different countries, including 123 healthy volunteers, a group that provided a database for normal values. In addition, the test meal used was standardized and well tolerated. Furthermore, the protocol was simple, with just 4 images over 4 h providing an accurate measure of delayed gastric emptying compared with a 2-h study. It was also concluded from this protocol that physiologic information (lag phase and rate of emptying) are not as important as the availability of a simple screening test.
CONCLUSION
The radionuclide low-fat-meal solid gastric emptying imaging protocol of Tougas et al. (1) is well tolerated by patients in terms of the egg substitute meal and comfort during imaging (short imaging time in an upright position). It increases available camera time, thus improving patient throughput. Image analysis is simple and easy to interpret, increasing patient referrals by gastroenterologists. The only major disadvantage of the protocol is that patients must be on the premises for 4 h to complete the study. Overall, this imaging protocol is beneficial for patients as well as for nuclear medicine sections and is cost-effective.
Acknowledgments
This work was presented at the 52nd Annual Meeting of the Society of Nuclear Medicine, Toronto, Ontario, Canada, June 18–22, 2005.
References
- Received for publication September 19, 2005.
- Accepted for publication March 27, 2006.





{kind=link}