


Abstract
Recently, the use of 18F-FDG PET has progressed rapidly as a standard diagnostic imaging tool in many types of cancer. The purpose of this study was to evaluate the patterns and prevalence of muscle uptake as a result of muscle activity shortly before the 18F-FDG injection or during the uptake phase. Methods: From October 2002 to October 2003, whole-body 18F-FDG PET scans (4-min emission and 3-min transmission per bed position) were performed on 1,164 patients with known or suspected malignancy. Images were acquired on a dedicated PET scanner 45−60 min after an intravenous injection of a weight-adjusted dose of 7.4 MBq/kg (0.2 mCi/kg) with a maximum of 925 MBq (25 mCi) 18F-FDG. A log of any nonphysiologic muscle activity during the uptake phase or reported excessive muscle activity the day before scanning was kept by the technologists. In addition, PET scans were reviewed retrospectively to evaluate any undesirably increased muscle uptake. Results: A total of 146 of 1,164 patients (12.5%) had excessively increased muscle uptake detected on the PET scan that corresponded to the technologists' notes of muscle activity during the uptake phase or before 18F-FDG injection. Encountered patterns of muscle uptake due to muscle activity included uptake in neck, secondary to neck strain from being on a stretcher; masseter, secondary to chewing gum; vocal cords, secondary to speaking; chest wall, secondary to labored breathing; forearms and hands, secondary to reading; and lower extremities, secondary to nervous tapping of the feet. Conclusion: Undesirably increased physiologic muscle uptake is frequently encountered on 18F-FDG PET scans. In this study, 12.5% of patients were affected. It is prudent to instruct the patient to avoid any excessive physical activity at least 48 h before injection as well as to not exert muscle activity during the uptake phase. Furthermore, a record should be kept by the technologist of any observed excessive muscle activity during the uptake phase and reported to the reading physician—thus, eliminating a potential source of false-positive findings on interpreting PET scans.
PET has been growing as a standard diagnostic tool in detecting and staging many types of cancer. The most common PET radiotracer used in oncology is the glucose analog 18F-FDG. 18F-FDG activity in muscle is frequently encountered on PET scans (1). Normal muscles accumulate little 18F-FDG, but muscles exercised just before or around the time of 18F-FDG injection can exhibit intense 18F-FDG uptake (2).
Muscle uptake can be attributed to voluntary or involuntary muscle activity, increased insulin, and surgical interventions (3,4). Voluntary muscle activity consists of activities such as talking, chewing, and exercising. Involuntary muscle activity would include labored breathing or stress-induced muscle spasms. Increased activity in muscles can potentially create problems in differentiating between normal and pathologic uptake of 18F-FDG.
Several studies have described how 18F-FDG has been used to evaluate muscle activity due to exercise (5–9). In addition, more recently, 18F-FDG uptake in adipose tissue and muscle has been described as potential sources of false-positive results (10). The aim of this study was to evaluate the prevalence and common patterns of increased physiologic muscle uptake due to excessive muscle activity during or shortly before the uptake phase.
MATERIALS AND METHODS
Patients
From October 2002 to October 2003, 1,164 consecutive whole-body (WB) 18F-FDG PET scans were performed in our institution for patients with known or suspected cancer. Brain studies were excluded from this study population. All WB scans were acquired on a dedicated PET scanner (Advance; GE Healthcare). Patients fasted for a minimum of 4 h before the 18F-FDG injection. Blood glucose levels were routinely measured. The maximum acceptable level was 200 mg/dL. Each patient was intravenously injected with 7.4 MBq/kg (0.2 mCi/kg) of 18F-FDG, with a maximum of 925 MBq (25 mCi). All patients sat in a quiet room during a 45- to 60-min uptake phase. Finally, the technologists recorded any excessive physical activity reported by the patient during the 24 h before the examination and any excessive activity they observed during the uptake phase.
Image Acquisition
68Ge transmission scans were acquired for 3 min per bed position. The transmission scans were acquired to generate an attenuation correction map to correct the emission images. Emission scans were acquired at 4 min per bed position. The field of view (FOV) was typically from the base of the skull to midthigh with the exception of melanoma patients, who were imaged from the top of the head to the bottom of the feet. The 2-dimensional WB acquisition parameters consisted of a 128 × 128 matrix and 15-cm FOV with a 3-slice overlap. Processing consisted of the ordered-subsets expectation maximization (OSEM) method using 21 subsets and 2 iterations.
Image Analysis
PET scans were analyzed retrospectively by 2 authors for the prevalence and patterns of muscle uptake. Any evidence of abnormally increased muscle activity was noted. Cases suspected of uptake in brown fat were excluded from this study. After the visual assessment, the PET reports and technologists' notes were reviewed for references to the observed increased muscle uptake.
RESULTS
The retrospective evaluation found that 146 (82 male, 64 female; mean age, 59.0 y; age range, 10−85 y) of the 1,164 (12.5%) patients demonstrated excessively increased 18F-FDG muscle uptake. Increased muscle uptake was further divided into 5 anatomic groups (Table 1): head and neck (n = 76), thorax (n = 33), upper extremities (n = 61), lower extremities (n = 20), and diffuse (n = 9). Therefore, the 146 patients accounted for a total of 199 encounters of increased muscle activity. This was attributed to some patients having muscle uptake in multiple categories.
Patterns of Increased Metabolic Muscle Activity
DISCUSSION
PET detects metabolic or molecular alterations common in malignancy. 18F-FDG PET takes advantage of one such alteration—namely, accelerated glucose metabolism. 18F-FDG PET diagnoses, stages, and restages many cancers with accuracies ranging from 80% to 90% and is often more accurate than anatomic imaging (11). However, increased 18F-FDG avidity is not limited to malignancy, resulting in false-positive findings. Muscle uptake of 18F-FDG is a well-known cause of false-positive findings on PET (12).
In our study, increased muscle activity was frequently seen on 18F-FDG PET scans (12.5%). We found common patterns of physiologic muscle uptake in 5 general anatomic regions. Most common areas of increased uptake were the head and neck, thorax, and upper extremities. Less common areas of increased muscle uptake were the lower extremities and diffuse WB uptake (Table 1).
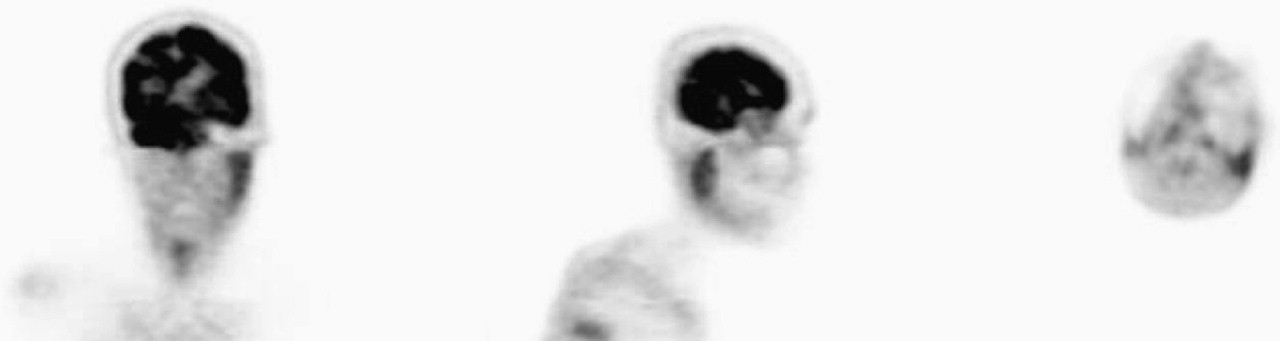
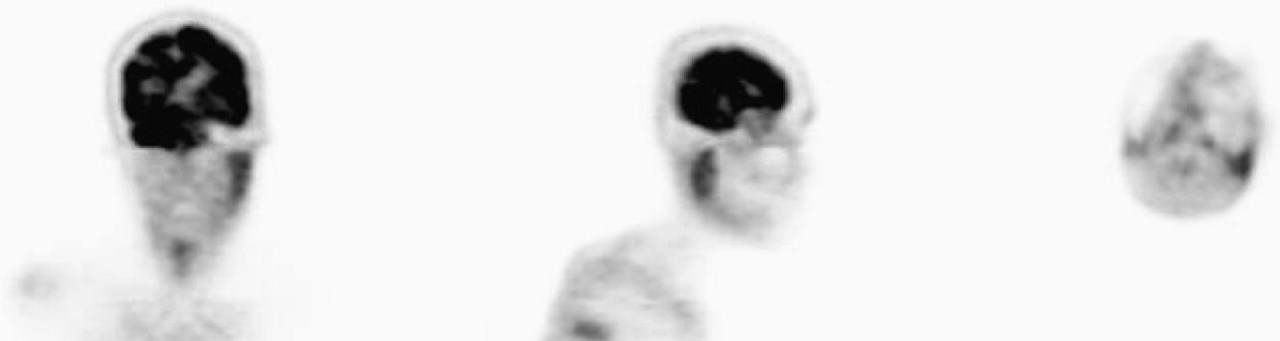
Physiologic 18F-FDG uptake in the neck and supraclavicular area has previously been described as “USA-fat” (13) as well as scalene muscle uptake (14). Cohade et al. (13) found that 5.8% of their patients had increased muscle uptake in the neck, which closely relates to the 6.5% found in the head and neck in our study. Anxiety has also been reported to cause muscle uptake in the neck muscles (12). Specific examples of head and neck uptake were found to be masseter muscle, sternocleidomastoid muscle, scalene muscle, and vocal cord activity. Increased masseter muscle uptake may be secondary to talking or chewing (Fig. 1). Increased activity of the sternocleidomastoid muscle may be caused by straining the neck or intense breathing or coughing. Neck strain was seen in patients on a stretcher when they raised their head to talk to the technologists during, and before, the uptake phase (Fig. 2). The scalene muscle helps assist in breathing by elevating the first 2 ribs. Because the scalene and sternocleidomastoid muscles are the prominent neck muscles used in breathing (15), one would expect to observe increased uptake in patients with labored breathing or intense coughing (Figs. 3 and 4). Bilaterally increased vocal cord activity was seen secondary to patients talking during the uptake phase (Fig. 5A). Unilateral uptake in the vocal cord has been described previously to be caused by compensatory laryngeal muscle activation secondary to contralateral recurrent laryngeal nerve palsy (16). Figure 5B is an example of unilateral vocal cord activity. Activity in the neck region needs to be looked at carefully so that it is not misinterpreted as malignancy.
An 84-y-old woman with history of lung cancer. Technologist noticed the patient chewing gum during uptake phase of examination. Unilateral masseter uptake is most likely secondary to the patient chewing with only the left side of her mouth.

A 67-y-old male patient with history of brain lesions. Urinary catheter indicates that this was an inpatient who came to PET department on a stretcher. Patient used sternocleidomastoid muscles while straining to lift his head to talk to technologists.
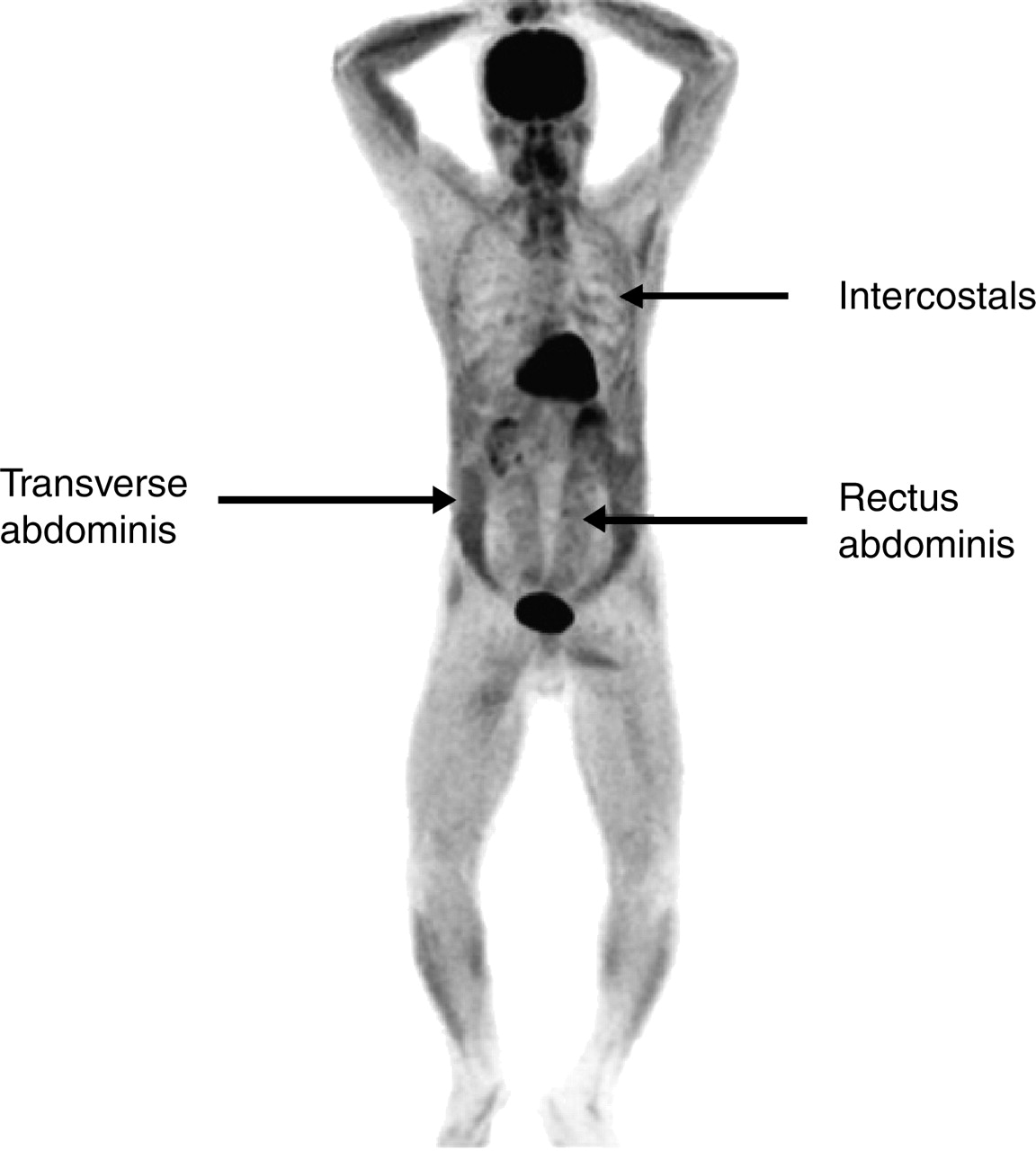
A 66-y-old man with history of severe chronic obstructive pulmonary disease. Patient had chronic cough that continued during uptake phase, straining abdominal and respiratory muscles.

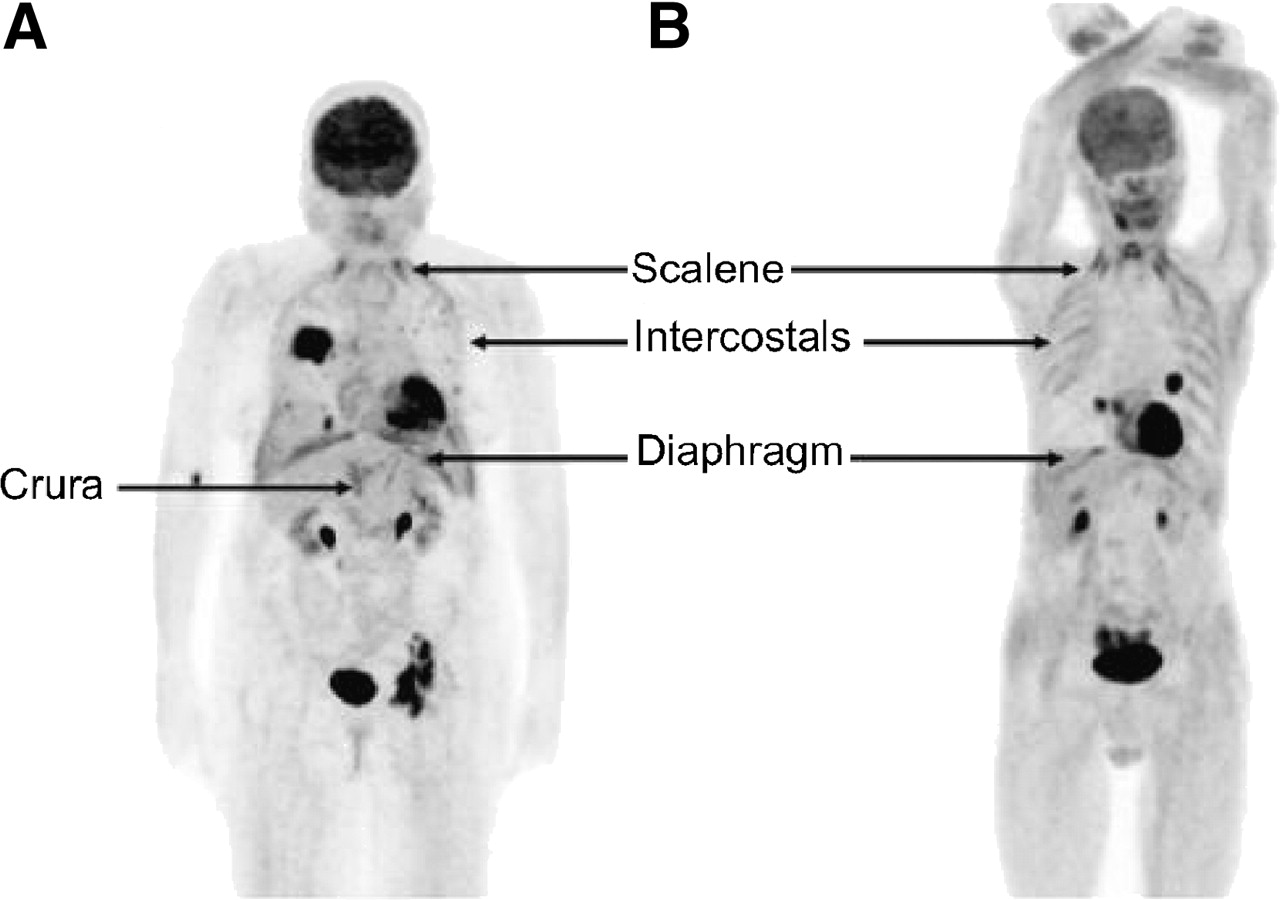
(A) A 78-y-old woman with history of non–small cell carcinoma. Patient complained of extreme shortness of breath and presented with intense coughing. (B) An 80-y-old man with history of squamous cell lung carcinoma. Increased uptake of diaphragm, crura, and accessory muscles of respiration is most likely due to labored breathing secondary to pulmonary disease.

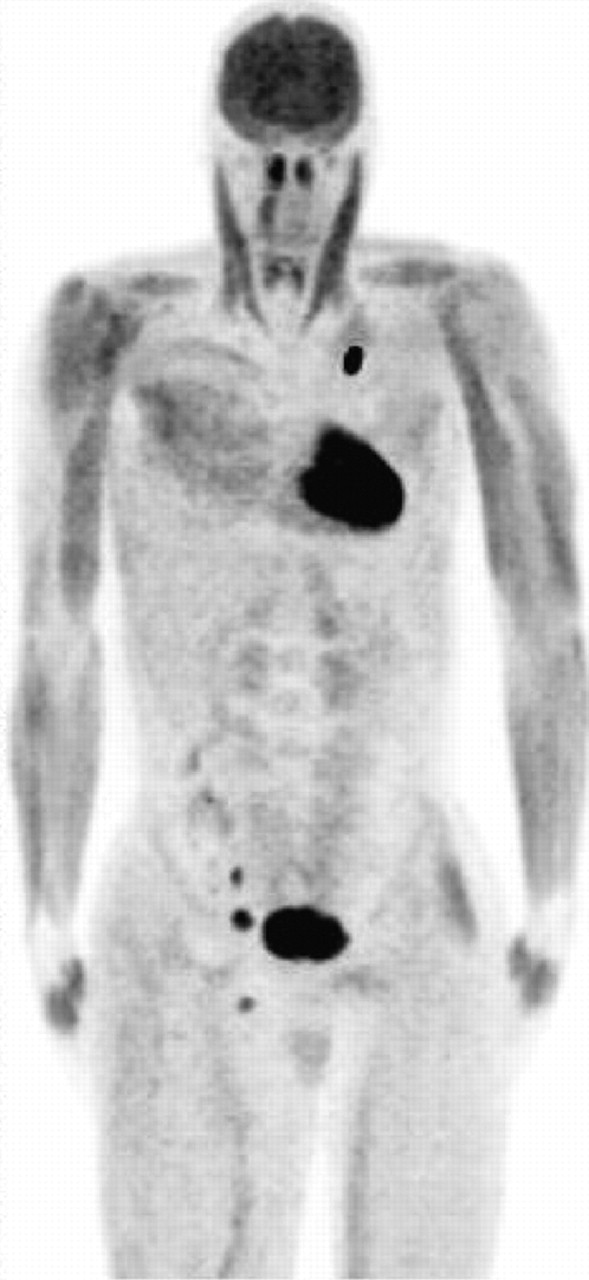
(A) A 65-y-old man was talking during uptake phase, which demonstrates increased bilateral vocalis muscle uptake. (B) A 75-y-old man with history of non–small cell lung cancer of left lung. Unilateral vocalis muscle uptake most likely is explained by laryngeal nerve palsy due to chemotherapy and radiation.
A recent study evaluated excessive metabolic activity of thoracic and abdominal muscles on 18F-FDG PET in patients with chronic obstructive pulmonary disease (COPD) (17). In our study, the thoracic muscles visualized were the intercostals and the diaphragm (Fig. 4). Increased uptake of the intercostal muscles was seen most commonly in patients with labored breathing secondary to COPD. The diaphragm would also show increased uptake in patients with labored breathing or coughing. Increased activity in these muscles may represent a potential source of false-positive interpretations. For example, bone metastases could easily be mistaken for intercostal muscle uptake or vice versa. Also, the crura of the diaphragm could easily be mistaken for adrenal lesions.
The flexor carpi and digitorum muscles, extensor carpi and digitorum muscles, and muscles of the hand were the most common muscles visualized in the upper extremities. These muscles would show increased uptake secondary to writing or turning pages while reading a book or magazine (Fig. 6). Figure 7 illustrates an example of a patient who pushed herself to the PET department in a wheelchair, which explains the increased activity in the triceps.
A 60-y-old man with history of lung cancer. Technologist noticed patient reading a small book during uptake phase. Bilateral extensor and hand muscle uptake is most likely due to holding the book and turning pages.

A 71-y-old woman with history of lung cancer and COPD. Patient was noticed pushing herself to PET department in a wheel chair, which explains increased activity in triceps.
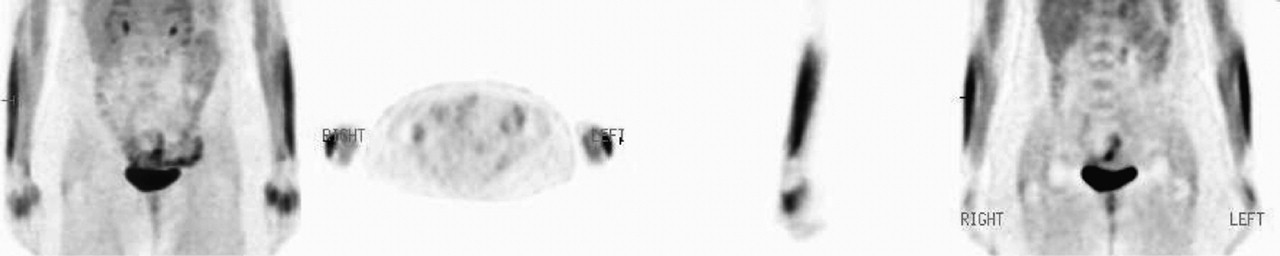
In the lower extremities, the muscles of the anterior compartment (tibialis anterior, extensor digitorum longus, and extensor hallucis longus) were the most frequently visualized muscles (Fig. 8). Muscle uptake in these areas was attributed to the patient tapping her feet during the uptake phase. However, uptake in this area could also be attributed to activities as simple as excessive walking before 18F-FDG injection.

Muscles of anterior compartment of lower extremities were commonly seen in patients who walked excessively or tapped their feet before or during uptake phase. (A) A 48-y-old woman with history of melanoma was tapping her feet during uptake phase. (B) A 25-y-old male patient with Ewing's sarcoma who recently had right femur prosthesis. Increased activity in left anterior tibialis muscle was most likely due to altered weight bearing.
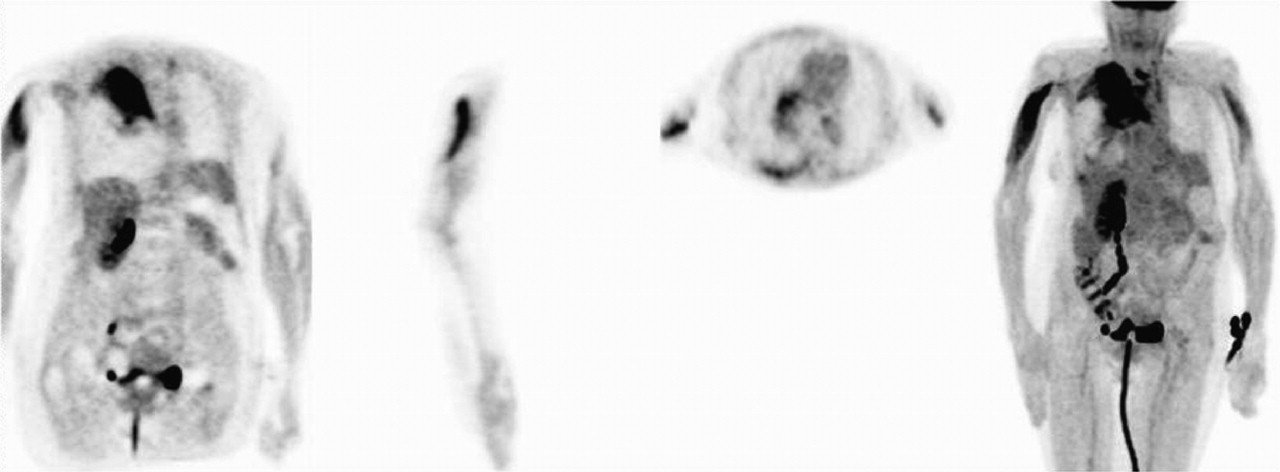
Diffuse WB muscle uptake can be caused by insulin, recent food intake, and strenuous exercise that involves many muscle groups (Fig. 9). Although this type of increased muscle uptake was seen in <1% of the patients, it can be very problematic when attempting to interpret the PET study, particularly in patients with melanoma or soft-tissue malignancies.

A 25-y-old man with history of Ewing's sarcoma. Diffuse muscle activity was most likely due to walking with crutches before 18F-FDG injection.
Because increased muscle uptake is commonly seen (12.5%), it illustrates the importance of the role of the technologist. To lower the amount of false-positive interpretations, it is important for the technologist to record any muscle activity that is noticed during the uptake phase. For example, if the technologist sees the patient performing physical activities before the study or during the uptake phase, documentation is necessary so that the reading physician can incorporate such information into the PET scan interpretation. It was also found that increased muscle uptake can be caused by excessive muscle activity shortly before the PET scan. Increased muscle uptake has been detected even 48 h after excessive physical activity (18). Knowing this, it is important to instruct the patient to refrain from any avoidable muscle activity during the uptake phase as well as avoid excessive physical activity for a minimum of 48 h before the 18F-FDG injection. Note that, although increased muscle uptake occurred in one eighth of our patients, in many patients it did not represent a problem in interpretation.
PET was the only modality considered in this study. The accuracy of describing muscle location and differentiating between specific muscles was somewhat limited in our study because of the use of PET, not PET/CT, images. Furthermore, our study was also limited in that our WB FOV covered only from the base of the skull to the upper thigh and did not include most of the lower extremities in many cases. These limited lower extremity data may help explain why increased uptake in the muscles of the lower extremities was less common than that of the upper extremities. The fact that not as many patients had muscle uptake in the thigh muscles of the lower limbs is not surprising because lower extremity muscle uptake is found below the knee (19). Currently, we are replicating this study on a PET/CT scanner using a true WB protocol, covering from the top of the head to the bottom of the feet, for all of our patients.
CONCLUSION
Increased metabolic activity in muscle secondary to excessive muscle activity during the uptake phase and shortly before 18F-FDG injection was commonly seen (12.5%) in our studied population. Thus, we believe that it is prudent for the technologists not only to instruct the patients to minimize muscle activity during the uptake phase but also to telephone the patients ahead of their appointments to advise them to refrain from any excessive muscle activity at least 48 h before the PET scan. In addition, it is necessary for the technologists to observe the patients during the uptake phase and report any noted avoidable or excessive muscle activity to the reading physician. When present, any unexpected or unexplained excessive muscle uptake should initiate communications between technologists and reading physicians to avoid false-positive PET scan interpretations.
Acknowledgments
We thank technologists Penny Yost, Crystal Botkin, and Stephanie Anastas for their technical support.
References
- Received for publication June 30, 2005.
- Accepted for publication December 9, 2005.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Clinical values of FDG PET in polymyositis and dermatomyositis syndromes: imaging of skeletal muscle inflammation
- Detection of Inflammatory Lesions by F-18 Fluorodeoxyglucose Positron Emission Tomography in Patients with Polymyositis and Dermatomyositis
- Does 18F-FDG Uptake by Respiratory Muscles on PET/CT Correlate with Chronic Obstructive Pulmonary Disease?
- Prospective Evaluation of Physiologic Uptake Detected with True Whole-Body 18F-FDG PET/CT in Healthy Subjects