


Abstract
The adrenals are often a site of metastatic spread of cancer, and evaluation of the adrenals is important in assessing the extent of disease involvement in several malignancies. PET with 18F-FDG has been found extremely effective in detecting adrenal involvement not identified on CT or not meeting the CT size criteria for malignancy. However, evaluation of the adrenals and of retroperitoneal adenopathy or other pathologic conditions with 18F-FDG PET can be complicated at times by normal accumulation of the tracer in the uppermost renal calyx because of its somewhat posterior orientation, particularly when it is dilated. It is not infrequent for physicians to report doubt about adrenal involvement and to suggest that the PET findings be correlated with CT findings. This problem can often be circumvented clinically by administering intravenous furosemide (dosage adjusted according to body weight) to remove 18F-FDG activity from the renal pelvicalyceal system and by rescanning approximately 15–20 min later using 1–2 bed positions that include the renal area. We present 5 case vignettes, with representative illustrations, providing convincing evidence of the usefulness of this simple, noninvasive interventional procedure in ruling out suspected adrenal involvement that is otherwise difficult to assess, thereby obviating any further confirmation.
Abdominal and pelvic 18F-FDG PET images are prone to artifacts due to urinary tract and bowel activity. These artifacts are, in our experience, a real obstacle to differential diagnosis in centers having no CT coregistration and can lead to false-positive results. Lesions might often be overlooked because they are obscured by 18F-FDG accumulation along the colon or in the kidneys, ureters, or bladder. Uptake by the adrenal is often mistaken for normal retention in an upper-pole calyx and vice versa, leading to erroneous reporting. To solve this problem, we propose a simple interventional adjunct that involves injecting furosemide and obtaining a localized 18F-FDG PET acquisition of 1–2 bed positions about 15–20 min after injection. We have found that the focus of uptake washes out in cases of caliceal accumulation and either is not modified or becomes more clearly delineated in cases of disease involvement.
MATERIALS AND METHODS
Patients
The 5 cases illustrated (Figs. 1–5) were selected from proven cases of various malignancies studied using the proposed interventional procedure at the single largest PET center in India.
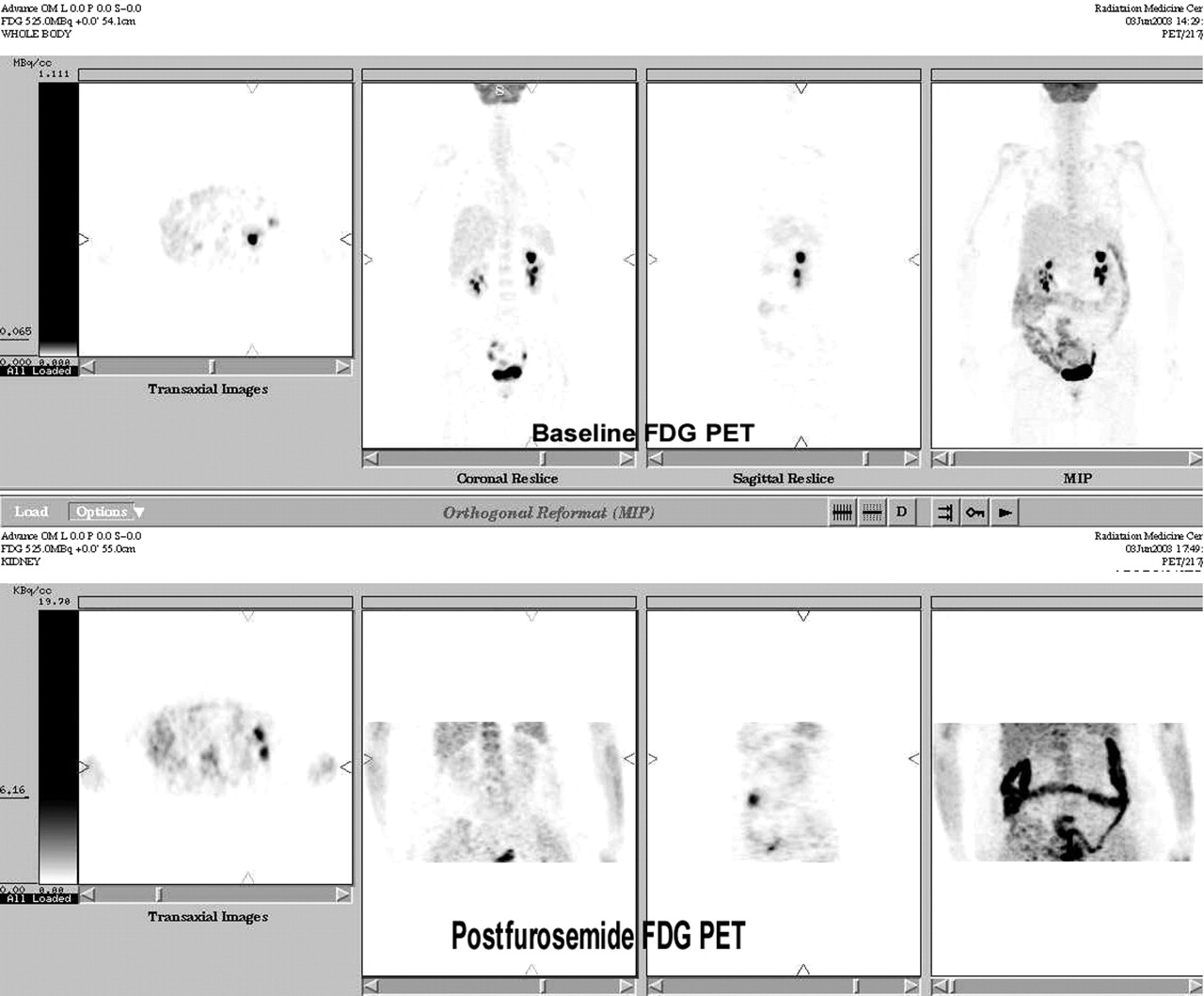
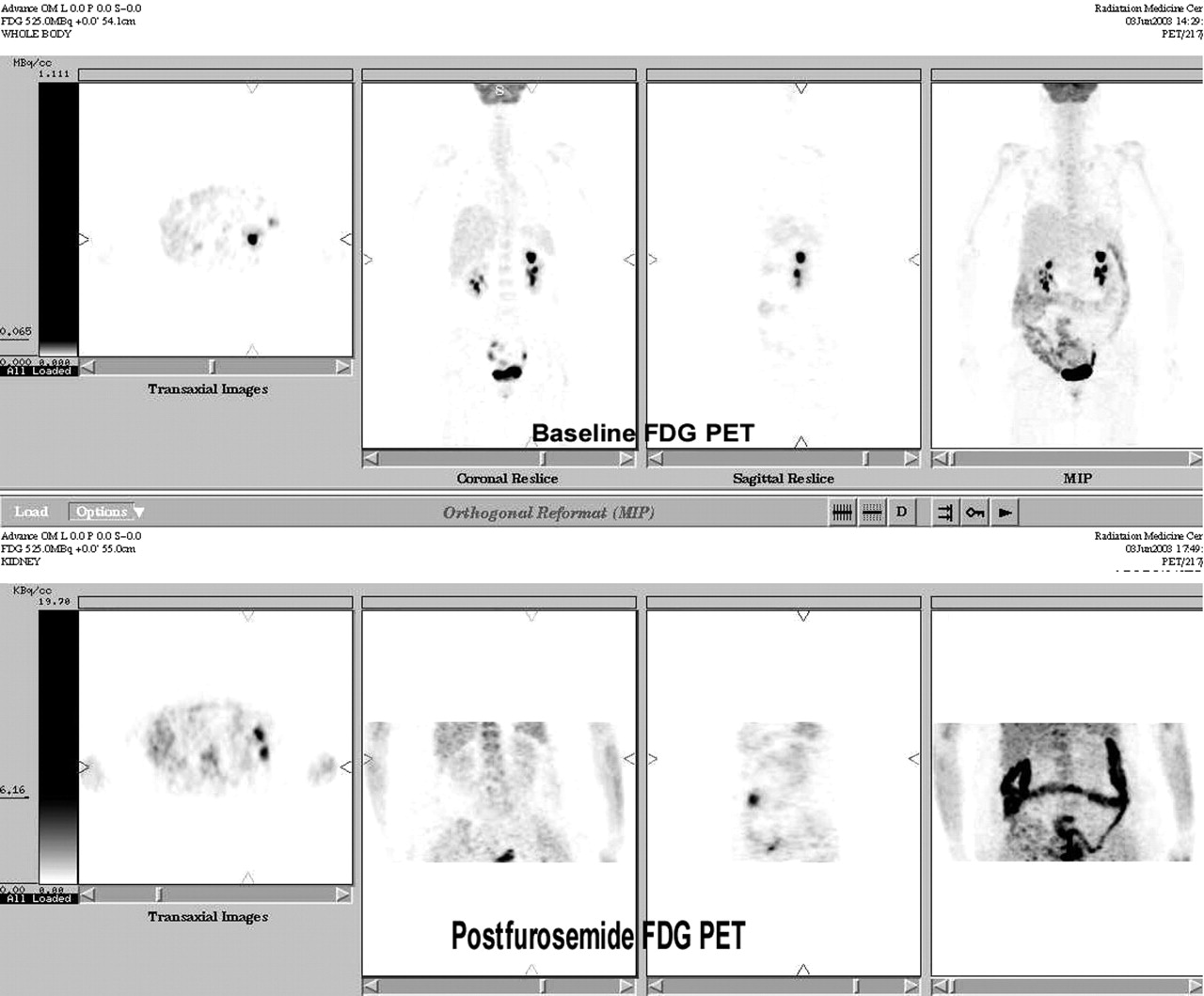
Whole-body PET images of 49-y-old woman in whom adenocarcinoma of right ovary was diagnosed in 1992 and high-grade leiomyosarcoma of left ovary was diagnosed in 2003. She underwent hysterectomy and right salpingo-oophorectomy for the former and left salpingo-oophorectomy and omentectomy for the latter. Postoperatively, she was treated with external radiotherapy and ifosfamide (Holoxan; Baxter Oncology)-based chemotherapy. Her recent abdominal CT findings were normal, and tumor markers were within normal limits. PET was performed to search for any residual disease.
PET Studies
The patients were imaged on a dedicated bismuth germanate-based PET scanner (Advance; GE Healthcare). Images were reconstructed using an attenuation-weighted ordered-subsets expectation maximization (OSEM) algorithm. Patients voided before each PET study as part of the regular protocol.
For the first study, the patients were imaged 60 min after injection of 444 MBq of 18F-FDG. Around 10–15 min before completion of the study, furosemide was administered intravenously (40 mg for adults and 1 mg/kg of body weight for children). The patients then left the imaging table and voided before the second study, which was performed 15–20 min after injection of the furosemide.
Image Interpretation
Axial, coronal, sagittal, and 3-dimensional PET images were visually interpreted by 2 experienced nuclear medicine physicians who were unaware of the results of CT and of other conventional morphologic imaging modalities but knew the location of the primary tumor. Foci of uptake seen on the first study were concluded to be due to activity in the renal pelvicalyceal system if they were not evident on the second study.
RESULTS
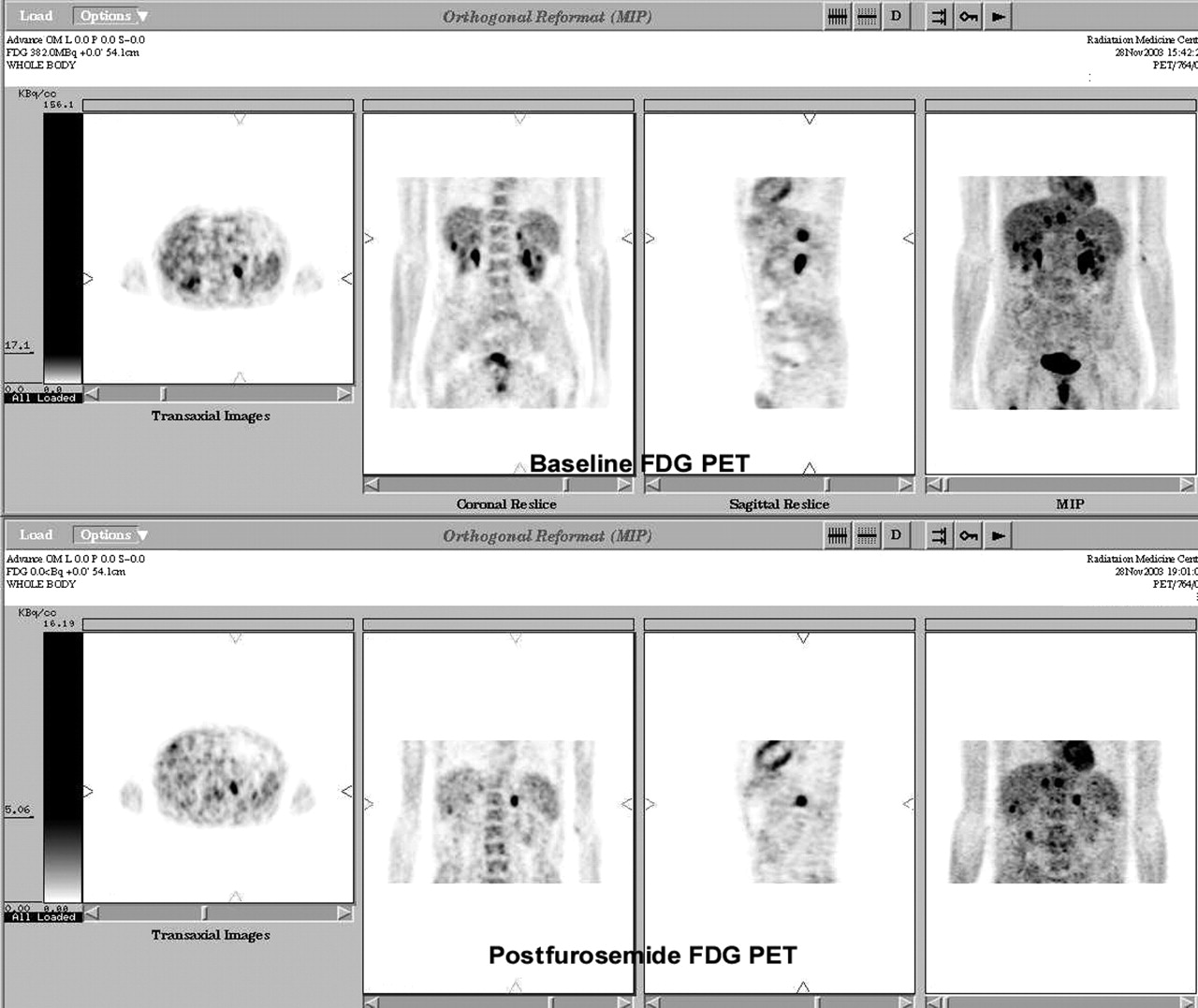
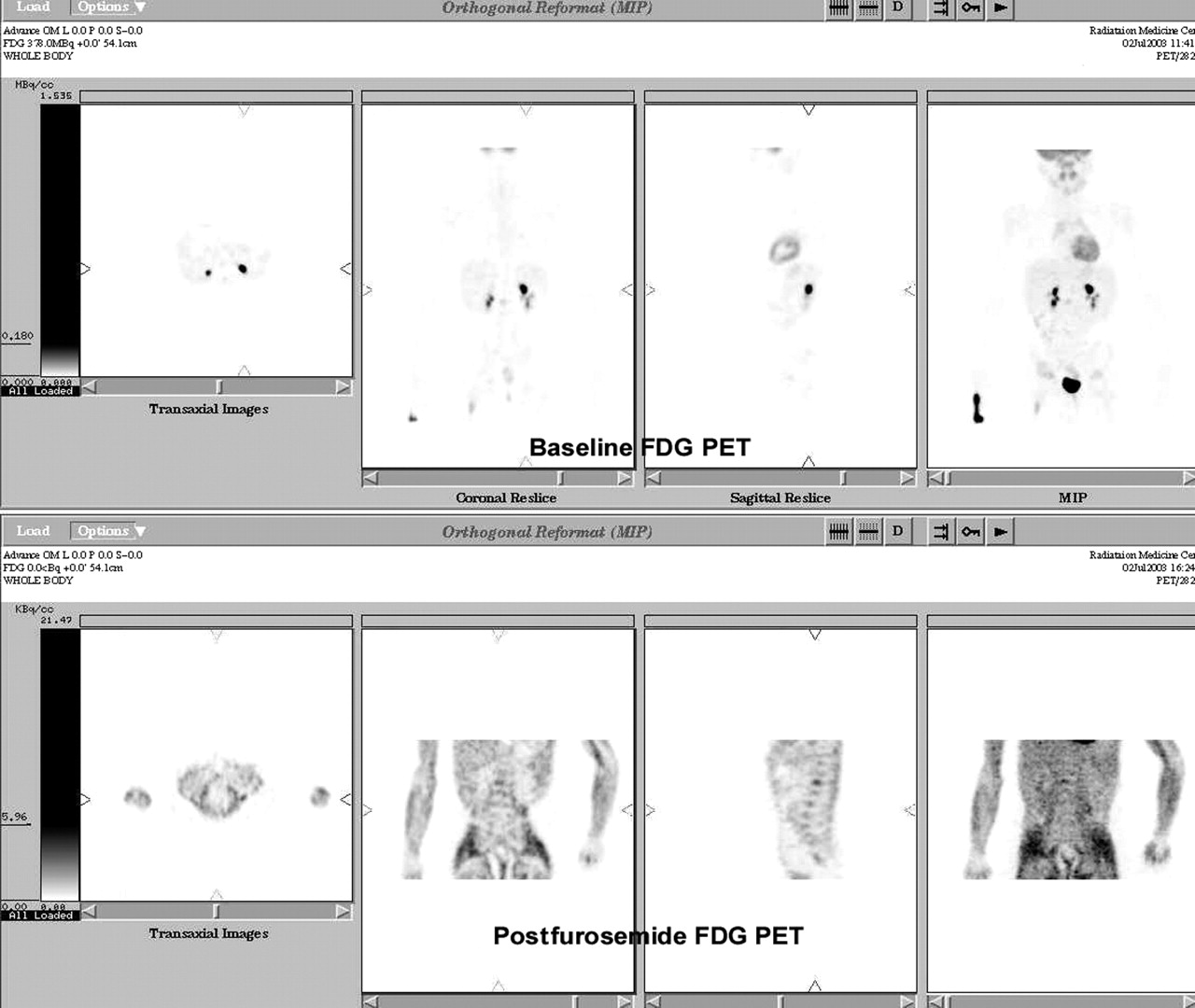
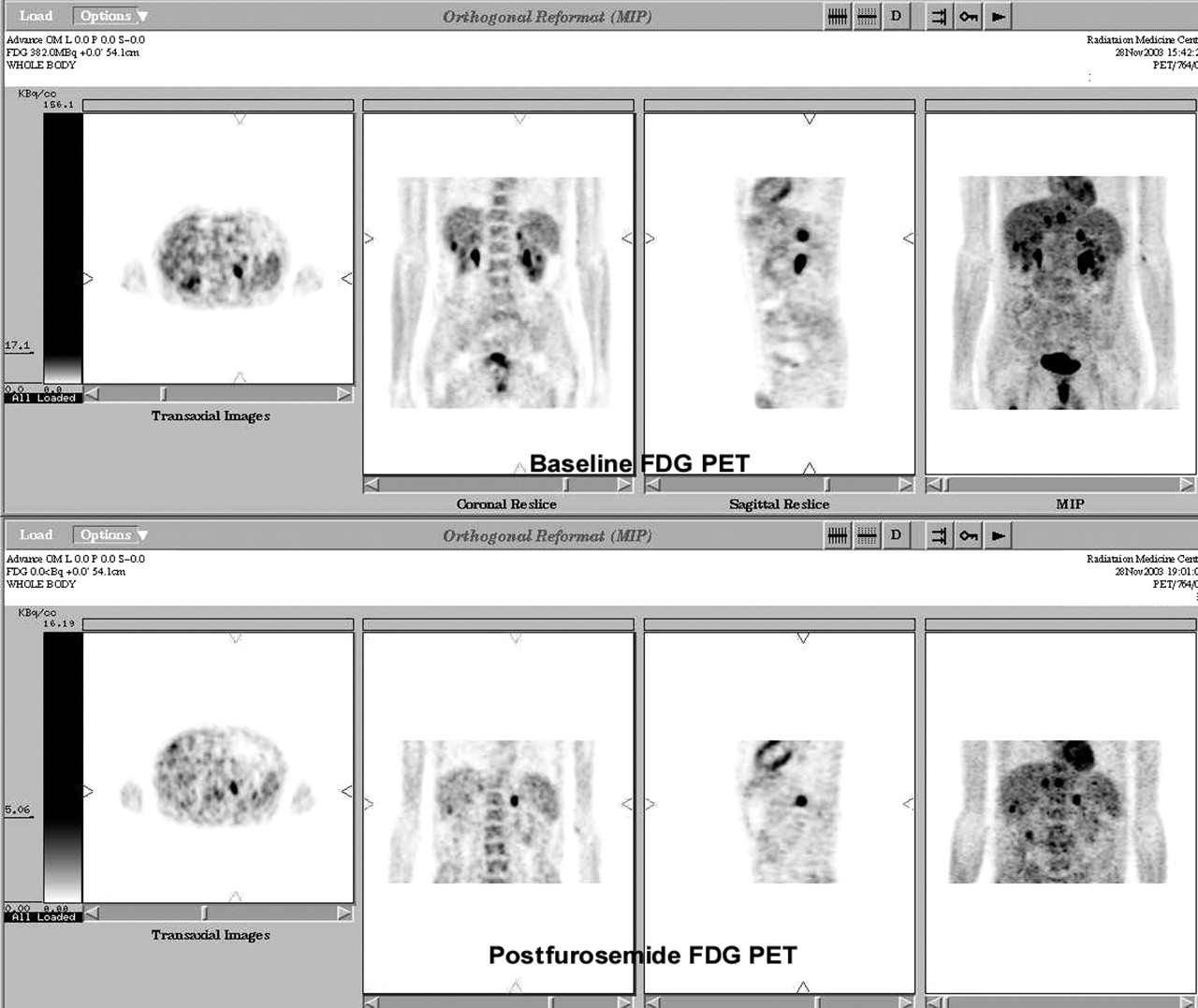
In the 5 cases presented, diagnostic conflict existed as to whether the hyperintense 18F-FDG uptake seen on baseline 18F-FDG PET represented a metastatic deposit in the adrenals or kidneys or physiologic tracer accumulation in the upper caliceal system. In the patients of Figures 1–3 and 5, the hyperintense uptake was on the left side, whereas in the patient of Figure 4, 18F-FDG uptake on the right side was the reason for the diagnostic dilemma. In the patient of Figure 2, because the primary was a left adrenal neuroblastoma, the ipsilateral 18F-FDG uptake in the upper renal calyx posed a dilemma as to whether local recurrence was present. The postfurosemide PET scans of the patients of Figures 1, 2, and 4 showed clearance of activity from the suspected site, confirming that tracer accumulation had indeed been in the renal pelvicalyceal system. In none of these was adrenal or renal disease radiologically evident at the first follow-up visit, at 1 y. In the patient of Figure 3, in addition to the increased 18F-FDG uptake observed at the primary site, in multiple nodes in the chest, in the right scapula (not shown in the figure), in the liver, in a few abdominal lymph nodes, and in the proximal right femoral shaft, an intense hot spot was seen at the upper pole of the left kidney. In the patient of Figure 5, whole-body 18F-FDG PET revealed multiple hypermetabolic foci in the right chest wall and left lower neck, diffuse uptake at the surgical site, and a doubtful focus at the upper pole of the left kidney. In both the patient of Figure 3 and the patient of Figure 5, the postfurosemide scan eliminated the possibility that 18F-FDG activity stemmed from the renal pelvicalyceal system. Because uptake around the upper pole was unaffected, adrenal involvement was held out as the most probable cause of the 18F-FDG uptake, as was subsequently proven by abdominal CT.
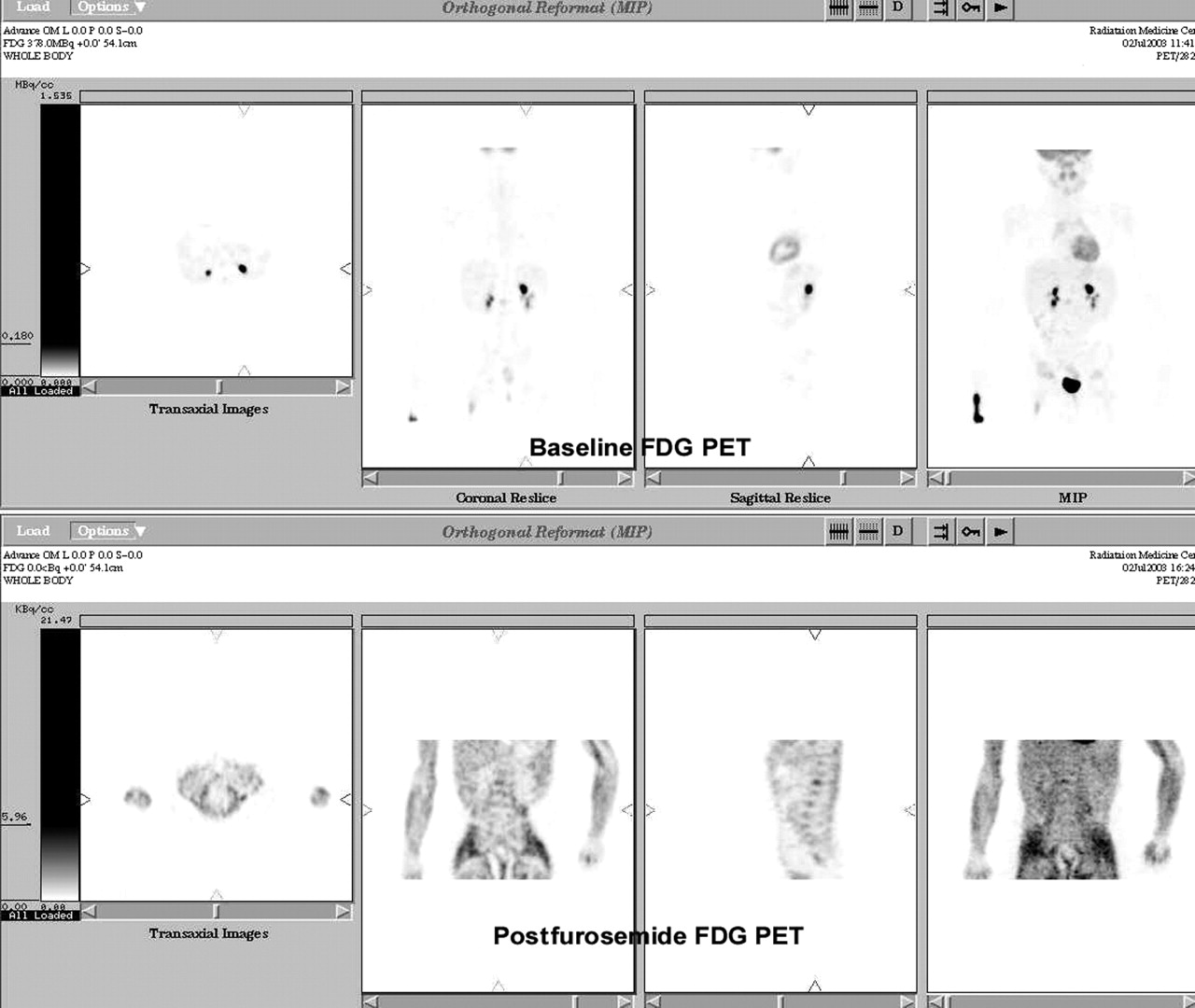
18F-FDG PET images of 4-y-old boy in whom, 3 y previously, left adrenal neuroblastoma was diagnosed and treated with left adrenalectomy. Histopathologic examination revealed differentiated, stroma-poor neuroblastoma, and all sampled retroperitoneal nodes were free of disease. Bone marrow was not involved. Patient was not subjected to chemotherapy or radiotherapy in view of localized disease. The 24-h urinary vanillylmandelic acid level had recently been rising and was 19.5 mg/g of creatinine (reference range, 1–10 mg/g) at time of PET.
18F-FDG PET images of 64-y-old man with 2.5-mo history of right-sided chest pain, cough, and hemoptysis. Thoracic CT revealed 5.5 × 3.8 cm spiculated mass in right upper lobe and extending to hilum. Cytology of CT-guided fine-needle aspirate was suggestive of adenocarcinoma. He was referred for metastatic survey with PET.

18F-FDG PET images of 15-y-old boy in whom non-Hodgkin’s lymphoma had been diagnosed at the age of 6 y and who had been disease free and asymptomatic for the past 8 y. Recent abdominal CT performed as part of routine follow-up had shown hypodense, minimally enhancing 1-cm area in right kidney most likely representing a cystic lesion. However, PET was performed because, considering patient’s history, a lymphomatous deposit could not be ruled out.
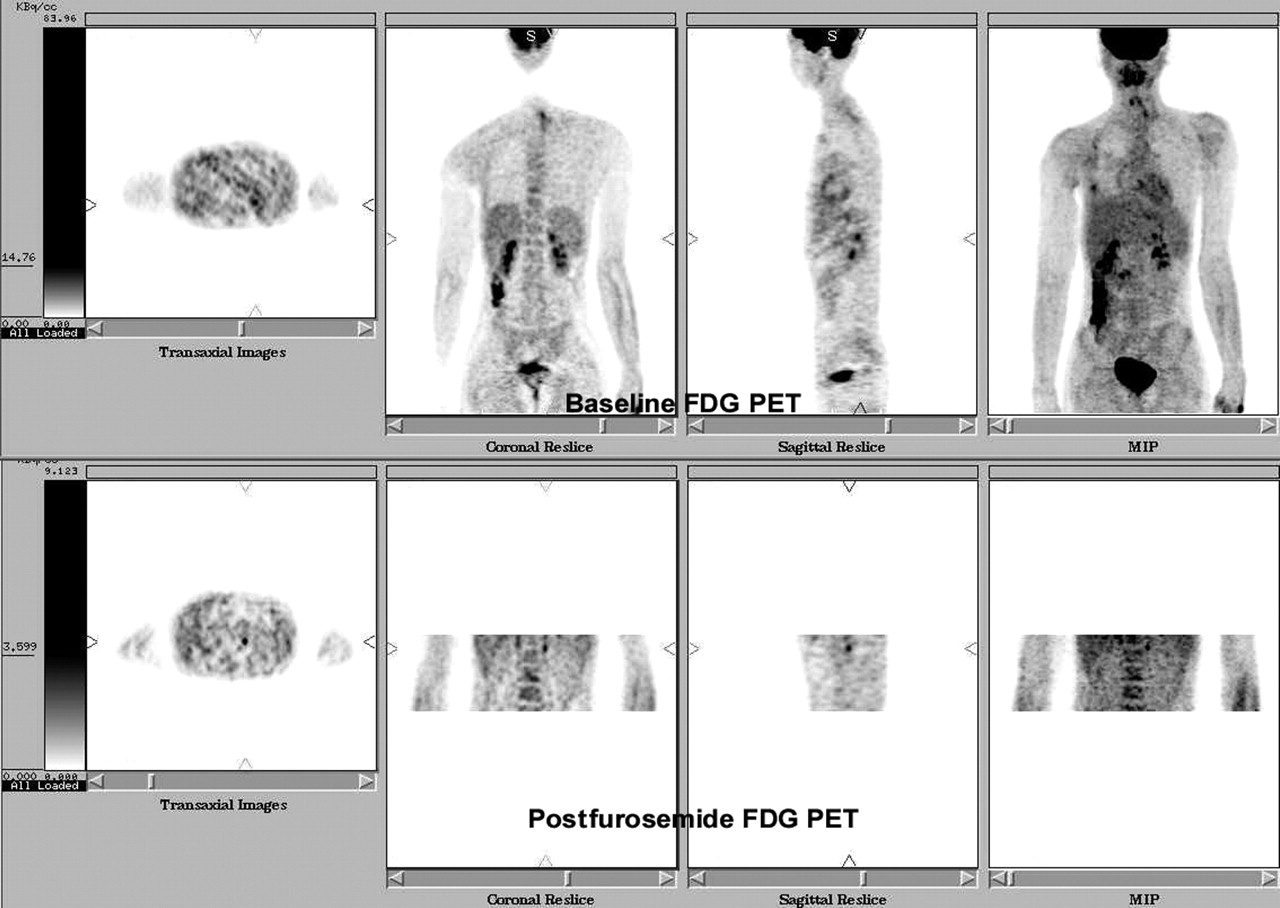
18F-FDG PET images of 15-y-old boy with primitive neuroectodermal tumor of right chest wall. PET was performed to evaluate the disease after surgery and chemotherapy. Recent thoracic CT had shown evidence of partial collapse and consolidation of anterior segment of right upper and middle lobes, with thickening of right minor fissure.
DISCUSSION
Elimination of artifactual accumulation of 18F-FDG in the colon and urinary system is essential for appropriate staging of cancer using PET. Evaluation of the pelvis is vital in clinically organ-confined prostate cancer, documented pelvic adenopathy, and recurrence of cervical carcinoma in the stump. Intense urinary bladder activity impairs interpretation in all these clinical settings by masking the adjacent lesional uptake. Several studies (1–5) have addressed this issue. Simple ways to avoid it include intravenous hydration, administration of furosemide, and catheterization and retrograde filling of the bladder with saline solution. These methods ensure a clean scanning field and provide a well-defined anatomic landmark for study interpretation (4). Some authors (5) have observed, in animal studies, that although pretreatment with l-lysine or furosemide failed to decrease renal activity of 18F-FDG, saline injection without furosemide markedly decreased urinary activity.
Adrenal gland involvement, which is often an important issue in clinical decision making in oncology, can be assessed simply and reliably by administration of intravenous furosemide and rescanning at 1–2 bed positions. This interventional procedure can reduce 18F-FDG PET misinterpretation by eliminating confounding renal caliceal uptake that may at times mimic adrenal lesions or a metastatic deposit in the kidney. Though this procedure is possible with both filtered backprojection and OSEM, image quality is significantly better with OSEM. We suggest that adoption of this procedure be considered on a case-to-case basis, especially when intense 18F-FDG activity is present in or around the superior pole of the kidney and is difficult to designate as adrenal involvement or activity in the upper calyx. To the best of our knowledge, no comprehensive study dealing with this differential diagnosis by this method has been published.
CONCLUSION
Furosemide administration and limited rescanning is a simple, noninvasive, yet highly effective technique in cases of doubtful adrenal involvement on baseline 18F-FDG PET. The present study can be extrapolated to resolve other doubtful perirenal foci and can have a significant bearing on subsequent decisions about patient management.
Footnotes
For correspondence or reprints contact: Sandip Basu, MBBS (Hons), DRM, DNB, Radiation Medicine Centre, Bhabha Atomic Research Centre, Tata Memorial Centre Annexe, Jerbai Wadia Rd., Parel, Bombay 400 012, India.
E-mail: drsanb{at}yahoo.com





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}