


Abstract
We report an unusual severe systemic reaction that occurred in a woman after a 99mTc-methylene diphosphonate bone scan and for which no alternative explanation could be found. The bone scintigram showed diffusely increased uptake in the liver and kidneys accompanied by reversible dysfunction of these organs and dermatologic manifestations. We speculate that an immune-mediated mechanism may have caused this unusual reaction.
Bone scintigraphy using 99mTc-labeled diphosphonates is safe, but there have been rare reports in the literature of adverse effects after the procedure. The documented events include headache, chills, fever, nausea, vomiting, skin rash, itching, urticaria (erythematous, raised skin), hypotension, anaphylaxis, and, rarely, cardiac arrest. They tend to occur generally 2–24 h after the radiopharmaceutical injection.
CASE REPORT
A 42-y-old woman with a history of recurrent breast cancer was referred to the nuclear medicine department for a bone scintigram to exclude skeletal metastasis. She had undergone a right simple mastectomy followed by axillary clearance 18 mo previously. No adverse reaction had been reported after the initial bone scan, which had been performed at the time of surgery and showed normal findings. After recurrence of the cancer, she completed a course of high-dose chemotherapy with epirubicin (100 mg/m2 × 4) 1 wk before being referred for the second bone scan. She was not receiving any medication and had no history of iron overloading or hypercalcemia.
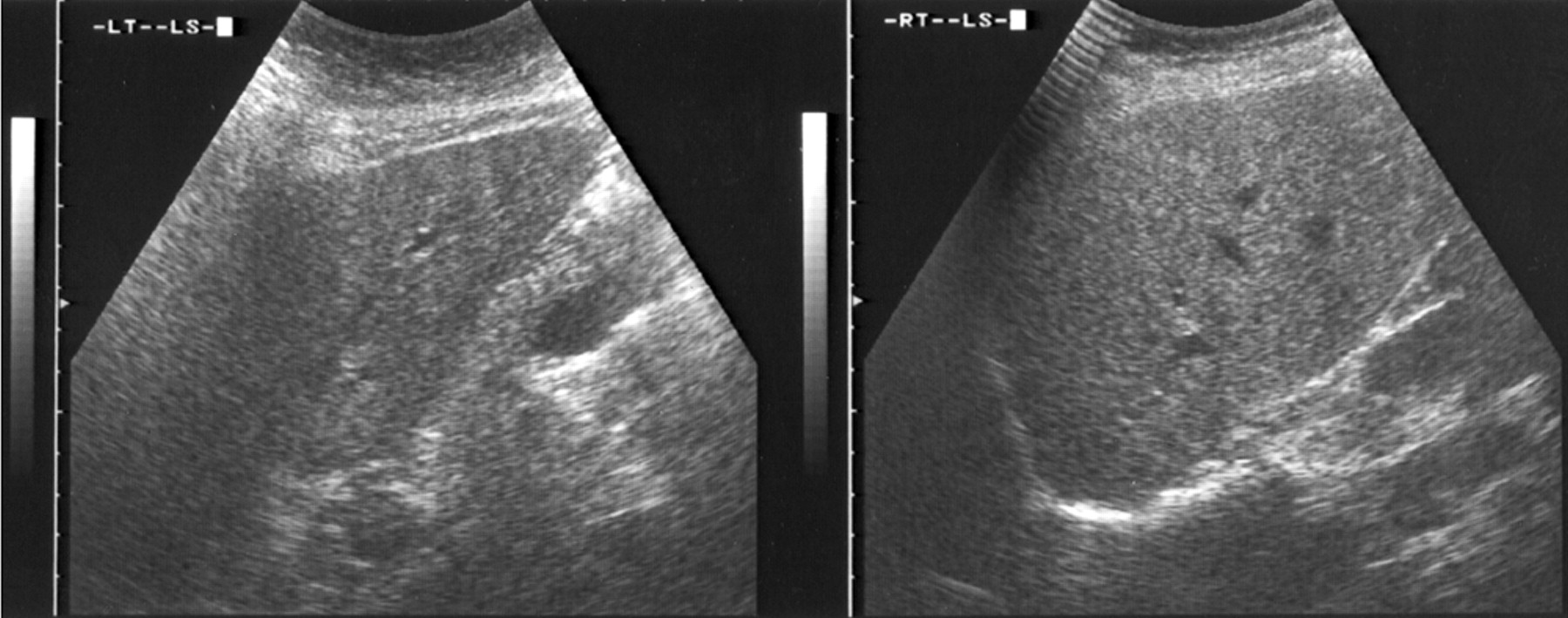
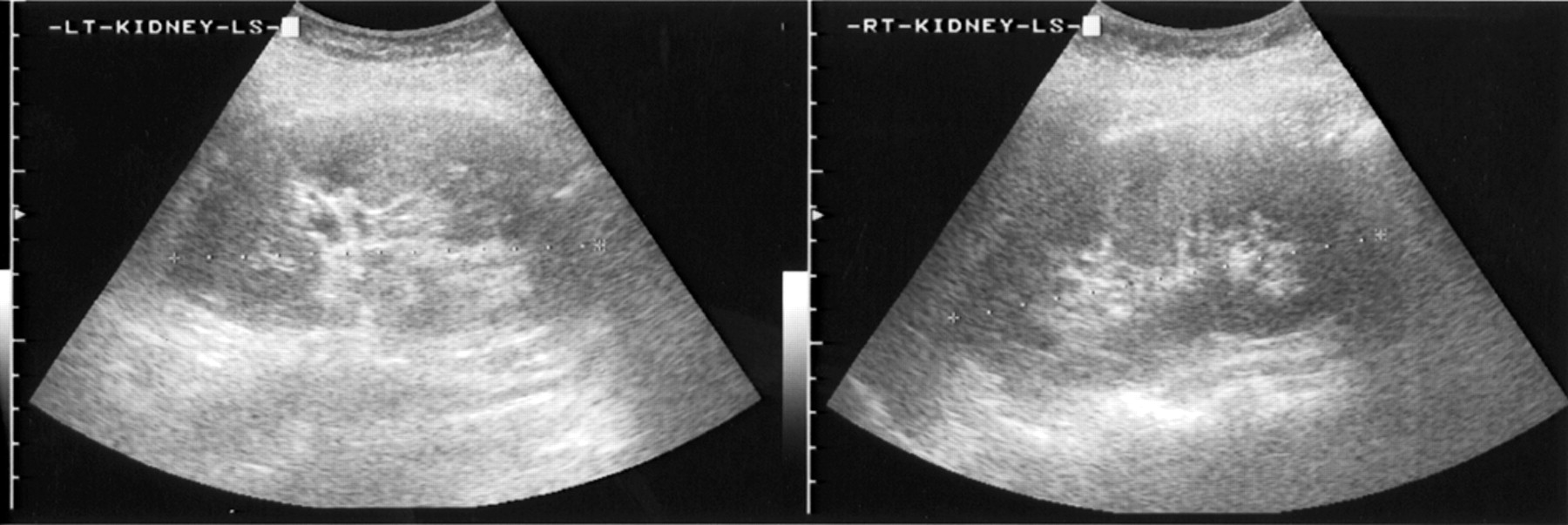
Gamma camera images performed 4 h after intravenous injection of 555 MBq (15 mCi) 99mTc-methylene diphosphonate (MDP) (Amerscan Medronate II Agent; Nycomed Amersham) showed homogeneously increased tracer uptake in the liver and kidneys (Fig. 1). In addition, a solitary hot spot on the left side of the sacrum was suggestive of a metastasis. No abnormal extraosseous uptake or adverse symptoms were reported in other patients who underwent a bone scan on the same day. Twenty-four hours later the patient felt unwell, and puffiness developed around the eyes, along with oliguria, jaundice, and an erythematous skin rash on the trunk and around the eyes. Biochemical tests at that time, compared with those before the bone scan, suggested abnormal liver and kidney function (Table 1). Ultrasound examination of the abdomen (Figs. 2 and 3) did not reveal any abnormality in the liver or kidneys. The patient responded to a regime of intravenous fluids and corticosteroids, with a return to normal renal function 15 d after the bone scan and to normal liver function 21 d after the bone scan (Table 1). The dermatologic manifestations resolved within 1 wk.
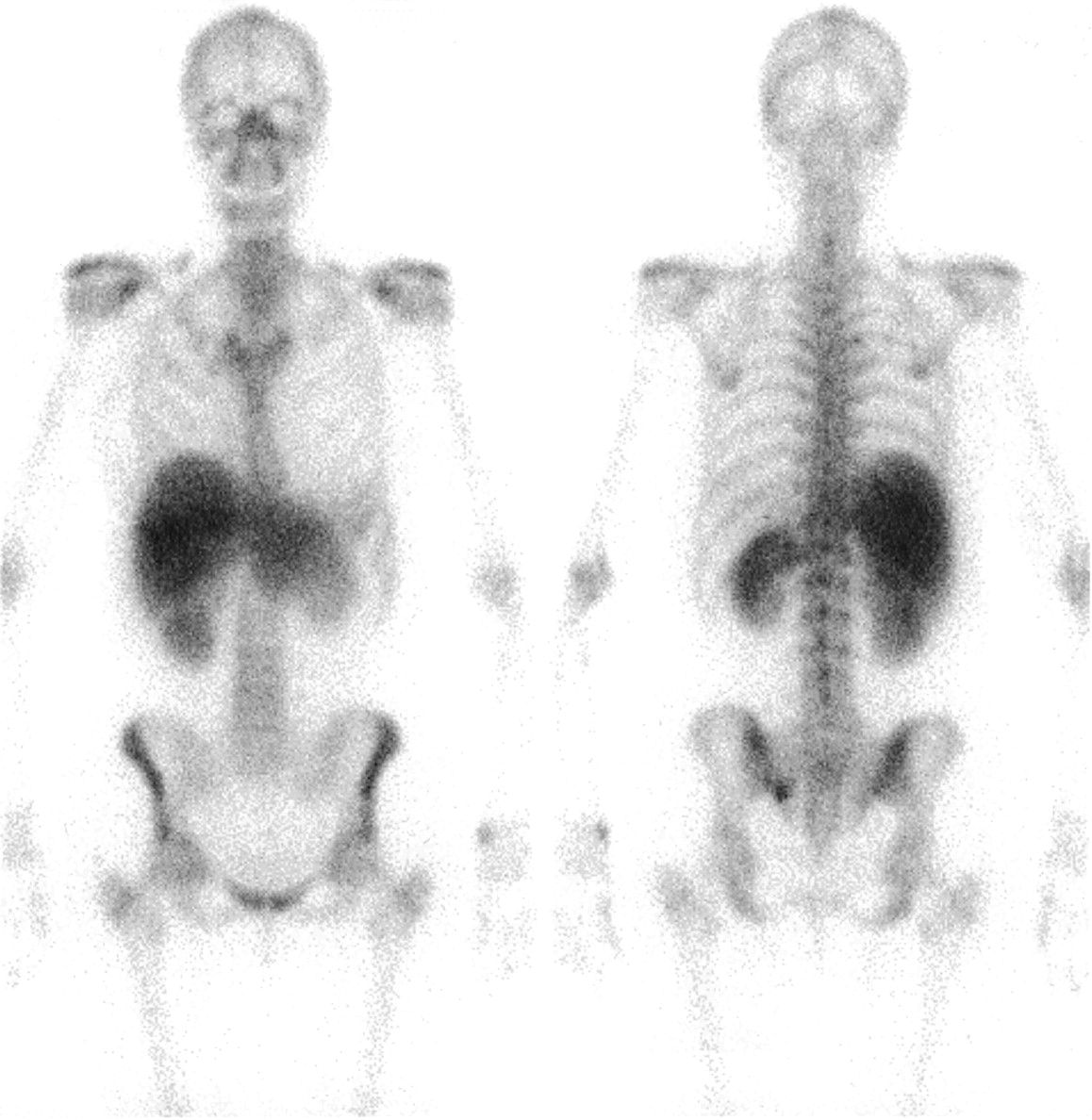
Whole-body bone scintigram demonstrates diffuse increased tracer uptake in liver and kidneys. Solitary metastasis is seen on left side of sacrum.

Ultrasound scan of abdomen shows normal liver.
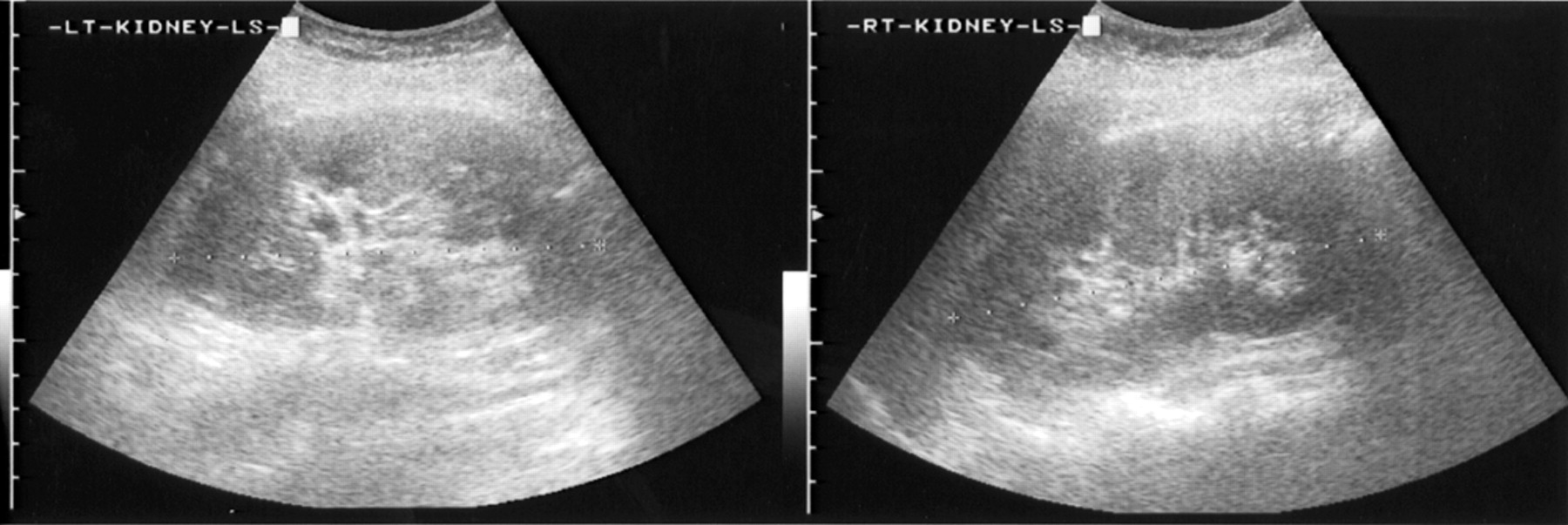
Ultrasound scan of abdomen shows normal kidneys.
Results of Blood Tests Before and After Bone Scan
DISCUSSION
Bone imaging agents accounted for nearly one third of the adverse reactions to radiopharmaceuticals reported in the United Kingdom over the 20 y between 1976 and 1996 (1). This figure is probably an overestimate, as the reactions also included vasovagal episodes and less clear-cut signs and symptoms. Diphosphonates were the major cause of skin reactions, but adverse effects also included a “cardiopulmonary arrest,” from which the patient was successfully resuscitated. The occurrence of similar reactions has been published in the past (2,3). None of the previous reports, however, described the potential for a severe reaction to diphosphonates, as experienced by our patient. Although it is difficult to prove a causal relationship between 99mTc-MDP injection and the development of a dermatologic reaction associated with hepatorenal failure, the temporal relation between the two and the quick response of the patient to rehydration and steroids and the lack of sequelae suggest an adverse reaction to the bone tracer. One may nevertheless argue that the uptake in the liver and spleen was probably related to previous chemotherapy and that the subsequent events were due to an adverse drug reaction, but there is no sure way of proving this argument. Normal ultrasound findings for the liver and kidneys, however, exclude tumor infiltration as the possible cause of abnormal uptake.
As to the exact mechanism that induced this reaction, one can only speculate. The fact that there was previous exposure to the agent points to an immunologic basis. An antigen (possibly one of the constituents of the injection)–antibody reaction has probably taken place, resulting in tissue deposition of immune complexes that, in turn, might have caused the organ damage and dermatologic changes. The situation, often called serum sickness from its original cause and description, is an important form of reaction seen with radiopharmaceuticals and presents as low-grade fever, urticaria, skin rash, and joint pain. The liver and kidney dysfunction observed in this patient may be a severe manifestation of the same problem. Further support for this assumption comes from the fast response to corticosteroids.
Diffuse accumulation of 99mTc-MDP in the liver after methotrexate treatment has been described (4). The index patient also had severe, but reversible, hepatic dysfunction attributed to methotrexate toxicity. Although not previously reported, epirubicin, the cytotoxic antibiotic used in our patient, has the potential to impair liver and kidney function. Furthermore, ischemic hepatitis is known to take up bone tracer (5). Similarly, Watanabe et al. have demonstrated diffuse increased renal uptake in acute renal tubular necrosis (6). These case reports clearly demonstrate that tissue injury, immunologic or otherwise, was the possible cause of increased liver and kidney uptake in our patient. The time scale of events, association of dermatologic reaction with hepatorenal dysfunction, and, finally, excellent response to steroid treatment, however, point to a hitherto unreported immunologic reaction to 99mTc-MDP unrelated to previous chemotherapy.
The present case is unique because it is, to our knowledge, the first report of an adverse reaction to bone tracer that resulted in reversible organ failure.
Footnotes
For correspondence or reprints contact: Kottekkattu K. Balan, MD, Department of Nuclear Medicine, Box 170, Addenbrooke’s Hospital, Cambridge CB2 2QQ, U.K.
E-mail: kottekkattu.balan{at}addenbrookes.nhs.uk





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.